S-ar putea să vă placă și
- ICU Scoring Systems A Complete Guide - 2020 EditionDe la EverandICU Scoring Systems A Complete Guide - 2020 EditionÎncă nu există evaluări
- Critical Care SedationDe la EverandCritical Care SedationAngelo Raffaele De GaudioÎncă nu există evaluări
- Initial Assesment and Management ATLS (Marissa)Document57 paginiInitial Assesment and Management ATLS (Marissa)jfsngdjÎncă nu există evaluări
- Initial Assessment and ManagementDocument8 paginiInitial Assessment and ManagementAlvin De LunaÎncă nu există evaluări
- Primary Trauma Care Manual: Standard Edition 2010 A Manual For Trauma Management in District and Remote LocationsDocument37 paginiPrimary Trauma Care Manual: Standard Edition 2010 A Manual For Trauma Management in District and Remote Locationsdavid wyantoÎncă nu există evaluări
- Chest TraumaDocument1 paginăChest TraumaelaÎncă nu există evaluări
- Trauma OverviewDocument48 paginiTrauma OverviewFrancescoBarbero100% (1)
- Management of The EVDDocument7 paginiManagement of The EVDplethoraldork100% (1)
- Emergency Trauma CareDocument49 paginiEmergency Trauma Careandrei neagÎncă nu există evaluări
- Primary SurveyDocument19 paginiPrimary SurveyCaroline ChauÎncă nu există evaluări
- Pneumothorax: DR - Naveen Vennilavan R Pg-IiiDocument95 paginiPneumothorax: DR - Naveen Vennilavan R Pg-Iiinaveen vennilavanÎncă nu există evaluări
- Skin Integrity and Wound CareDocument47 paginiSkin Integrity and Wound CareCHALIE MEQUÎncă nu există evaluări
- Polytrauma: DR A.R.Baka Department of Surgery Federal Medical Center, YolaDocument57 paginiPolytrauma: DR A.R.Baka Department of Surgery Federal Medical Center, YolaAbuhafezbaka100% (1)
- ShockDocument25 paginiShockAvneet Maan100% (1)
- Critically Ill PatientDocument31 paginiCritically Ill PatientSameh Aziz100% (1)
- Advanced Airway Management: Leaugeay Webre, BS, CCEMT-P, Nremt-PDocument35 paginiAdvanced Airway Management: Leaugeay Webre, BS, CCEMT-P, Nremt-Pbasic100% (4)
- Management Acute StrokeDocument108 paginiManagement Acute StrokeratuhamimÎncă nu există evaluări
- RSI For Nurses ICUDocument107 paginiRSI For Nurses ICUAshraf HusseinÎncă nu există evaluări
- Major Goals of Emergency Medical TreatmentDocument124 paginiMajor Goals of Emergency Medical TreatmentTuTit100% (1)
- Renal TransplantationDocument50 paginiRenal Transplantationregie cuaresmaÎncă nu există evaluări
- Emergency DevicesDocument28 paginiEmergency DevicescorsaruÎncă nu există evaluări
- Chapter 8 - Emergency CareDocument16 paginiChapter 8 - Emergency CareAlyssa MadriagaÎncă nu există evaluări
- Triage and Disaster: Nur Masyeerah Abdul JalilDocument22 paginiTriage and Disaster: Nur Masyeerah Abdul JalilnavenÎncă nu există evaluări
- Diagnosis & Management of Shock: SuriyadiDocument17 paginiDiagnosis & Management of Shock: SuriyadiDeady NurdiantoÎncă nu există evaluări
- Emergency AssessmentDocument27 paginiEmergency AssessmentJoanna RachelÎncă nu există evaluări
- Final Common Medical Surgical EmergenciesDocument99 paginiFinal Common Medical Surgical Emergenciesapi-195799092Încă nu există evaluări
- Primary Care in Trauma PatientDocument109 paginiPrimary Care in Trauma PatientSumit AgarwalÎncă nu există evaluări
- Infective Diseases of Heart: Wella KarolinaDocument47 paginiInfective Diseases of Heart: Wella KarolinahayosiapaÎncă nu există evaluări
- Hemodynamic MonitoringDocument28 paginiHemodynamic MonitoringKimberlie Dela Merced Tomas100% (1)
- TriageDocument40 paginiTriagemody94546Încă nu există evaluări
- Malaysiantriagescalenewrevised2019!1!221014090642 28d8e1aeDocument18 paginiMalaysiantriagescalenewrevised2019!1!221014090642 28d8e1aenaqibsakila4286Încă nu există evaluări
- TraumaDocument10 paginiTraumaNur Liyana Ahmad ZakiÎncă nu există evaluări
- Hepatic Encephalopathy and ComaDocument19 paginiHepatic Encephalopathy and ComaJas Castro JoveroÎncă nu există evaluări
- TraumaBurn ClinicalGuidelines Final PDFDocument34 paginiTraumaBurn ClinicalGuidelines Final PDFJuan Antonio GarcíaÎncă nu există evaluări
- Ostomy Care in Home Health1Document39 paginiOstomy Care in Home Health1api-315120220100% (1)
- ShockDocument7 paginiShockmara5140Încă nu există evaluări
- GCS Assessment - Information SheetDocument4 paginiGCS Assessment - Information SheetVeronica TanuwijayaÎncă nu există evaluări
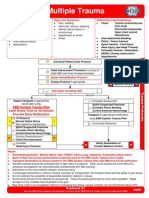
- Multiple Trauma ManagementDocument1 paginăMultiple Trauma ManagementSetiawan Arif WibowoÎncă nu există evaluări
- Cerebrovascular Accident (CVA)Document71 paginiCerebrovascular Accident (CVA)nur muizzah afifah hussinÎncă nu există evaluări
- Cardiac Emergencies: American Red Cross Emergency Response ClassDocument36 paginiCardiac Emergencies: American Red Cross Emergency Response ClassFia lisa MarindaÎncă nu există evaluări
- BTLS TraumaDocument41 paginiBTLS TraumaArif Dika MahendraÎncă nu există evaluări
- Burn ManagementDocument64 paginiBurn Managementabdullah100% (1)
- Tension Pneumothorax 170102133730Document21 paginiTension Pneumothorax 170102133730novelraaaÎncă nu există evaluări
- RECMOD2 Primary and Secondary SurveyDocument56 paginiRECMOD2 Primary and Secondary Surveydragon66Încă nu există evaluări
- Emergency Cart and Code BlueDocument10 paginiEmergency Cart and Code BlueKath100% (1)
- Cardiac EmergencyDocument56 paginiCardiac Emergency21rayhanf100% (1)
- Fall PreventionDocument24 paginiFall Preventionlittleshortgurl100% (1)
- Valve Repair & ReplacementDocument27 paginiValve Repair & ReplacementmaibejoseÎncă nu există evaluări
- Trauma and Its ComplicationsDocument80 paginiTrauma and Its Complicationsjoe BouGhazaliÎncă nu există evaluări
- Patient SafetyDocument18 paginiPatient SafetySuhatman AhÎncă nu există evaluări
- Multiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationDocument1 paginăMultiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationKelly JacksonÎncă nu există evaluări
- Hemodynamic MonitoringDocument35 paginiHemodynamic MonitoringWiz SamÎncă nu există evaluări
- Acute Stroke Nursing GuidelineFINAL 1 2Document5 paginiAcute Stroke Nursing GuidelineFINAL 1 2radanikmaÎncă nu există evaluări
- Heart Block PPT by SibaDocument36 paginiHeart Block PPT by Sibaritumitu_ritumitu100% (1)
- Assessment and Initial Management of The Trauma Patient: Courtesy of BTLS OntarioDocument42 paginiAssessment and Initial Management of The Trauma Patient: Courtesy of BTLS OntarioAlexandria100% (1)
- Bladder InjuryDocument7 paginiBladder InjurycorsaruÎncă nu există evaluări
- Abdominal Trauma SeminarDocument16 paginiAbdominal Trauma SeminarNavya BolluÎncă nu există evaluări
- Early Warning Score & Rapid Response TeamDocument26 paginiEarly Warning Score & Rapid Response TeamAsim IdreesÎncă nu există evaluări
- Code Blue PresentationDocument22 paginiCode Blue PresentationNurhayatiÎncă nu există evaluări
- Medical Emergencies OMFSDocument72 paginiMedical Emergencies OMFSkatnev100% (1)
- Management of Tetanus Prone Wounds: SheetDocument1 paginăManagement of Tetanus Prone Wounds: SheetOkkie Mharga SentanaÎncă nu există evaluări
- Ispub 14140Document7 paginiIspub 14140Okkie Mharga SentanaÎncă nu există evaluări
- Muhni PrintDocument1 paginăMuhni PrintOkkie Mharga SentanaÎncă nu există evaluări
- Innovation in Total Knee ReplacementDocument11 paginiInnovation in Total Knee ReplacementOkkie Mharga SentanaÎncă nu există evaluări
- Abdominal TraumaDocument74 paginiAbdominal TraumaOkkie Mharga SentanaÎncă nu există evaluări
- Chest TraumaDocument79 paginiChest TraumaAnusha VergheseÎncă nu există evaluări
- Military Trauma Research Gaps FinalDocument22 paginiMilitary Trauma Research Gaps FinalOkkie Mharga SentanaÎncă nu există evaluări
- Arm HandDocument25 paginiArm HandOkkie Mharga SentanaÎncă nu există evaluări
- The Listening Part A and B QuestionsDocument20 paginiThe Listening Part A and B QuestionsOkkie Mharga SentanaÎncă nu există evaluări
- Anatomy of The Spine and Some Common PathologiesDocument72 paginiAnatomy of The Spine and Some Common PathologiesTHESSNAVARROÎncă nu există evaluări
- The Elbow Wrist and HandDocument38 paginiThe Elbow Wrist and HandOkkie Mharga SentanaÎncă nu există evaluări
- TOEFL Written Expression QuestionsDocument40 paginiTOEFL Written Expression QuestionsOkkie Mharga SentanaÎncă nu există evaluări
- TOEFL Written Expression QuestionsDocument40 paginiTOEFL Written Expression QuestionsOkkie Mharga SentanaÎncă nu există evaluări
- Central SensitizationDocument14 paginiCentral SensitizationdracoscribdÎncă nu există evaluări
- Dover 3000 ReviewerDocument30 paginiDover 3000 ReviewerroseÎncă nu există evaluări
- Fractura Columnae VertebralisDocument4 paginiFractura Columnae VertebralisTheo DapamedeÎncă nu există evaluări
- Spinal Exercise Home ProgrammeDocument19 paginiSpinal Exercise Home ProgrammePrabha VetrichelvanÎncă nu există evaluări
- First Aid TrainingDocument202 paginiFirst Aid TrainingTheFreeSpiritÎncă nu există evaluări
- Spinal Cord InjuryDocument25 paginiSpinal Cord InjurySolsona Natl HS Maananteng100% (2)
- Basic First Aid TrainingDocument109 paginiBasic First Aid TrainingFarrukh AhmedÎncă nu există evaluări
- Pepp Als PretestDocument4 paginiPepp Als PretestDave BoppÎncă nu există evaluări
- Literature ReviewDocument6 paginiLiterature Reviewapi-563243682Încă nu există evaluări
- Acute Traumatic Spinal Cord InjuryDocument18 paginiAcute Traumatic Spinal Cord InjurymedilearnersÎncă nu există evaluări
- Svoa Ne 02 020Document10 paginiSvoa Ne 02 020Trina ViskhawatÎncă nu există evaluări
- ASIA ISCOS Worksheet - 10.2019 - PRINT Page 1 2Document2 paginiASIA ISCOS Worksheet - 10.2019 - PRINT Page 1 2Ade Marvira PutriÎncă nu există evaluări
- Spinal TraumaDocument81 paginiSpinal TraumaharilÎncă nu există evaluări
- Patho Physiology Spinal Cord InjuryDocument2 paginiPatho Physiology Spinal Cord InjuryIris Caberte100% (1)
- Spinal Injury1 2 PPT PDFDocument60 paginiSpinal Injury1 2 PPT PDFIqra IftikharÎncă nu există evaluări
- GPC Fractura VertebralDocument44 paginiGPC Fractura VertebralEdgar Vargas GranadosÎncă nu există evaluări
- Spine TraumaDocument96 paginiSpine TraumaSherlockHolmesSezÎncă nu există evaluări
- Fractures of SpineDocument47 paginiFractures of Spinefaizal samadÎncă nu există evaluări
- Spinal Cord Injury - Symptoms and Prevention MethodsDocument1 paginăSpinal Cord Injury - Symptoms and Prevention MethodsMathew SargentÎncă nu există evaluări
- Development of A Swallowing Risk ScreeningDocument15 paginiDevelopment of A Swallowing Risk ScreeningTécnicos CredineÎncă nu există evaluări
- Spinal Cord Injury PDFDocument14 paginiSpinal Cord Injury PDFNiaÎncă nu există evaluări
- Principles of Surgical Management TreatmentDocument4 paginiPrinciples of Surgical Management Treatmenttamilvanan3Încă nu există evaluări
- Medical Surgical Nursing Nclex Questions Neuro1Document13 paginiMedical Surgical Nursing Nclex Questions Neuro1dee_day_80% (1)
- Spinal Injury and Spine Motion Restriction: Standard CompetencyDocument51 paginiSpinal Injury and Spine Motion Restriction: Standard CompetencyMichael DharshwinÎncă nu există evaluări
- Aos A1poster UpperCervCS Mar18Document1 paginăAos A1poster UpperCervCS Mar18Aussie AuliaÎncă nu există evaluări
- E3 - OrthoDocument49 paginiE3 - OrthoLuvleen KaurÎncă nu există evaluări
- NURSING PRACTICE 3 Edited AnswerkeyDocument9 paginiNURSING PRACTICE 3 Edited Answerkeykim_liñanÎncă nu există evaluări
- DNB Qs 10 Yrs PDFDocument65 paginiDNB Qs 10 Yrs PDFHaribabu ArumugamÎncă nu există evaluări
- Orthopedic Impairment 2Document2 paginiOrthopedic Impairment 2api-242024640Încă nu există evaluări
- Neurologic NCLEX Practice Test Part 1Document10 paginiNeurologic NCLEX Practice Test Part 1mpasague100% (2)