S-ar putea să vă placă și
- Basic NeuroanatomyDocument189 paginiBasic NeuroanatomyShael ZoletaÎncă nu există evaluări
- Ectopic PregnancyDocument19 paginiEctopic PregnancyShael ZoletaÎncă nu există evaluări
- EmbryologyDocument152 paginiEmbryologyShael ZoletaÎncă nu există evaluări
- Motions For IMDC 2018Document3 paginiMotions For IMDC 2018Shael ZoletaÎncă nu există evaluări
- Lupang Hinirang SATBDocument3 paginiLupang Hinirang SATBModie MasangkayÎncă nu există evaluări
- Obstetrical HemorrhageDocument107 paginiObstetrical HemorrhageShael ZoletaÎncă nu există evaluări
- Bone Repair: Mishael V. ZoletaDocument6 paginiBone Repair: Mishael V. ZoletaShael ZoletaÎncă nu există evaluări
- Ethics ProfessionalDocument47 paginiEthics ProfessionalShael ZoletaÎncă nu există evaluări
- What Makes It BeautifulDocument52 paginiWhat Makes It BeautifulShael ZoletaÎncă nu există evaluări
- Adolescent Epidemiology DR PeraltaDocument55 paginiAdolescent Epidemiology DR PeraltaShael ZoletaÎncă nu există evaluări
- Herbal Medicine For Medical StudentsDocument83 paginiHerbal Medicine For Medical StudentsShael ZoletaÎncă nu există evaluări
- HelpingDocument19 paginiHelpingShael ZoletaÎncă nu există evaluări
- Throat Pharynx Palatine Tonsils ENT LecturesDocument45 paginiThroat Pharynx Palatine Tonsils ENT Lecturessankarsuper83Încă nu există evaluări
- Elastic and FibrocartilageDocument5 paginiElastic and FibrocartilageShael ZoletaÎncă nu există evaluări
- Legal Status of Traditional Medicine and Alternative MedicineDocument293 paginiLegal Status of Traditional Medicine and Alternative MedicineShael ZoletaÎncă nu există evaluări
- 19th CenturyReVISED 09262016Document54 pagini19th CenturyReVISED 09262016Shael ZoletaÎncă nu există evaluări
- 1 23 17 DNA MetabolismDocument49 pagini1 23 17 DNA MetabolismShael ZoletaÎncă nu există evaluări
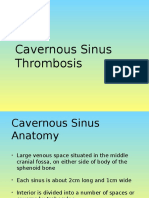
- Cavernous Sinus ThrombosisDocument21 paginiCavernous Sinus ThrombosisShael Zoleta100% (1)
- 15 Toughest Interview Questions and Answers!: 1. Why Do You Want To Work in This Industry?Document8 pagini15 Toughest Interview Questions and Answers!: 1. Why Do You Want To Work in This Industry?johnlemÎncă nu există evaluări
- Connective Tissue StructureDocument8 paginiConnective Tissue StructureShael ZoletaÎncă nu există evaluări
- Psychiatry Report - Neural Impulse and Synaptic TransmissionDocument19 paginiPsychiatry Report - Neural Impulse and Synaptic TransmissionShael ZoletaÎncă nu există evaluări
- WAIS R ExaminationDocument12 paginiWAIS R ExaminationShael ZoletaÎncă nu există evaluări
- Dna Genetic Anomalies ReportDocument11 paginiDna Genetic Anomalies ReportShael ZoletaÎncă nu există evaluări
- 18th Century Revised 2016Document41 pagini18th Century Revised 2016Shael ZoletaÎncă nu există evaluări
- Quasi ExperimentDocument20 paginiQuasi ExperimentShael ZoletaÎncă nu există evaluări
- Kohlberg 29Document32 paginiKohlberg 29hakkem bÎncă nu există evaluări
- Descriptive ResearchDocument11 paginiDescriptive ResearchShael ZoletaÎncă nu există evaluări
- The Nature of A HypothesisDocument4 paginiThe Nature of A HypothesisShael ZoletaÎncă nu există evaluări
- Host Script SamplesDocument4 paginiHost Script SamplesShael Zoleta100% (5)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Patient PositioningDocument35 paginiPatient PositioningDajour CollinsÎncă nu există evaluări
- 1495 2020 Anesthesiology Resident MDocument158 pagini1495 2020 Anesthesiology Resident MPL NLÎncă nu există evaluări
- 5.00 Safe Injection Practices Point of Care DevicesDocument40 pagini5.00 Safe Injection Practices Point of Care DevicesDrVishal BhattÎncă nu există evaluări
- Bronchoscopy For A Foreign Body in A ChildDocument19 paginiBronchoscopy For A Foreign Body in A ChildsileÎncă nu există evaluări
- Course Title: Surgery Tecniques - I & Clinical PracticeDocument4 paginiCourse Title: Surgery Tecniques - I & Clinical PracticeZia KhanÎncă nu există evaluări
- Induction of General Anesthesia - OverviewDocument40 paginiInduction of General Anesthesia - Overviewmayteveronica1000Încă nu există evaluări
- Persistent Paralysis After Spinal Paresthesia PDFDocument6 paginiPersistent Paralysis After Spinal Paresthesia PDFNadia Gina AnggrainiÎncă nu există evaluări
- Drugs ORDocument17 paginiDrugs ORCatherine ZamoraÎncă nu există evaluări
- Pedia Drugs Anes PDFDocument2 paginiPedia Drugs Anes PDFSven OrdanzaÎncă nu există evaluări
- NYSORA Thoracic Paravertebral BlockDocument16 paginiNYSORA Thoracic Paravertebral BlockYee Yeow100% (1)
- Surgery Written Assignment2016Document2 paginiSurgery Written Assignment2016Tyler EmmendorferÎncă nu există evaluări
- LA Nerve DamageDocument6 paginiLA Nerve DamagebabukanchaÎncă nu există evaluări
- MCI - SyllabusDocument11 paginiMCI - Syllabusintaa khabÎncă nu există evaluări
- 4 251320281908383404Document374 pagini4 251320281908383404Ramona PaulaÎncă nu există evaluări
- Craniotomy SurgeryDocument40 paginiCraniotomy Surgeryroba shukreÎncă nu există evaluări
- Atlas of Robotic Urologic SurgeryDocument473 paginiAtlas of Robotic Urologic SurgerySarita Moreno SorribasÎncă nu există evaluări
- Anesthesia History Calendar PDFDocument91 paginiAnesthesia History Calendar PDFgoogle playÎncă nu există evaluări
- Equine Anesthesia Course NotesDocument15 paginiEquine Anesthesia Course NotesSam Bot100% (1)
- Anesthesia For Craniotomy - UpToDateDocument47 paginiAnesthesia For Craniotomy - UpToDateAna Belén Artero CastañoÎncă nu există evaluări
- BAM Exotics ImagesGuide F 12-2016Document4 paginiBAM Exotics ImagesGuide F 12-2016smk0602Încă nu există evaluări
- Closed Treatment of Overriding Distal Radial Fractures Without Reduction in ChildrenDocument7 paginiClosed Treatment of Overriding Distal Radial Fractures Without Reduction in ChildrenPawan MarasiniÎncă nu există evaluări
- Basic Surgical Skills FinalDocument62 paginiBasic Surgical Skills Finalamel015Încă nu există evaluări
- Anesthesia in Pregnancy and ChildbirthDocument10 paginiAnesthesia in Pregnancy and ChildbirthNurul AiniÎncă nu există evaluări
- Thesis On Functional Endoscopic Sinus SurgeryDocument5 paginiThesis On Functional Endoscopic Sinus SurgeryBuyAPaperTulsa100% (2)
- Intra Operative MonitoringDocument4 paginiIntra Operative MonitoringEsamÎncă nu există evaluări
- Updated PGH Guidelines For ReferralsDocument2 paginiUpdated PGH Guidelines For ReferralsRocaya Lucman100% (1)
- Ncm108 Case BulalaqueDocument3 paginiNcm108 Case BulalaqueZee EedÎncă nu există evaluări
- Designing An Ideal Operating Room Complex: Indian Journal of Anaesthesia 2007 51 (3) : 193-199 Special ArticleDocument7 paginiDesigning An Ideal Operating Room Complex: Indian Journal of Anaesthesia 2007 51 (3) : 193-199 Special ArticleTejaswiniÎncă nu există evaluări
- The Nursing Role in Providing Comfort During Labor and BirthDocument18 paginiThe Nursing Role in Providing Comfort During Labor and Birthمريم حجيÎncă nu există evaluări
- Ge 9100C PDFDocument178 paginiGe 9100C PDFHellen Nogueira100% (2)