S-ar putea să vă placă și
- 2019 Jellycat Catalogo1Document59 pagini2019 Jellycat Catalogo1Cláudia100% (1)
- The Science of Psychic Healing - RamacharakaDocument133 paginiThe Science of Psychic Healing - RamacharakaAnoop NarayananÎncă nu există evaluări
- Urinary System Test BankDocument30 paginiUrinary System Test BankVinz TombocÎncă nu există evaluări
- Pom Pom Animals From Martha Stewart S Favorite Crafts For Kids PDFDocument10 paginiPom Pom Animals From Martha Stewart S Favorite Crafts For Kids PDFVladimirovÎncă nu există evaluări
- Case Presentation: A Malnourished ChildDocument35 paginiCase Presentation: A Malnourished ChildShaliniÎncă nu există evaluări
- Pathophysiology PneumoniaDocument2 paginiPathophysiology PneumoniaSheila Mae Escalante67% (3)
- A Case of Cerebral PalsyDocument26 paginiA Case of Cerebral PalsyAnas MohiuddinÎncă nu există evaluări
- Growth and DevelopmentDocument64 paginiGrowth and DevelopmentRahul Dhaker100% (1)
- A Case of ThalassemiaDocument10 paginiA Case of ThalassemiaAnas MohiuddinÎncă nu există evaluări
- Case Study TyphoidDocument10 paginiCase Study TyphoidArchana Sahu100% (3)
- Sword Breaker Issue No 1 - The Tyrant MachineDocument14 paginiSword Breaker Issue No 1 - The Tyrant MachineTrashDogÎncă nu există evaluări
- Care Plan On PneumoniaDocument22 paginiCare Plan On PneumoniaDimpal Choudhary100% (3)
- Failure To ThriveDocument93 paginiFailure To ThriveMuhammad Siddiq100% (1)
- Physical Growth and Development: Different Aspects and AssessmentDocument60 paginiPhysical Growth and Development: Different Aspects and AssessmentDipti RamiÎncă nu există evaluări
- Heart: Padangusthasana (Big Toe Pose)Document3 paginiHeart: Padangusthasana (Big Toe Pose)passion26Încă nu există evaluări
- Assessments of ToodlerDocument8 paginiAssessments of ToodlerYashoda SatputeÎncă nu există evaluări
- Nephrotic SyndromeDocument42 paginiNephrotic SyndromeSushmaÎncă nu există evaluări
- Morning Report: Disusun Oleh: Ria MaulindasariDocument37 paginiMorning Report: Disusun Oleh: Ria MaulindasaririamaulindasariÎncă nu există evaluări
- Morning Report: Fakultas Kedokteran Universitas Muhammadiyah Surakarta 2017Document43 paginiMorning Report: Fakultas Kedokteran Universitas Muhammadiyah Surakarta 2017devyÎncă nu există evaluări
- Cerebral Palsy Amdekar SirDocument42 paginiCerebral Palsy Amdekar SirVishalSapateÎncă nu există evaluări
- Growth and Development of NewbornDocument26 paginiGrowth and Development of Newbornroshen02Încă nu există evaluări
- One Symptom Only.: Use MK Dose For Pediatric MedicationsDocument12 paginiOne Symptom Only.: Use MK Dose For Pediatric MedicationsStewart Garneth Reston RancesÎncă nu există evaluări
- Down SyndromeDocument48 paginiDown SyndromeJohn Paul Parungao CrisostomoÎncă nu există evaluări
- Growth and Developments PDFDocument3 paginiGrowth and Developments PDFAlok SharmaÎncă nu există evaluări
- Growth &developmentDocument89 paginiGrowth &developmentAlaa JaibatÎncă nu există evaluări
- CP Acute and Chornic DiseaseDocument27 paginiCP Acute and Chornic DiseaseTopeshwar TpkÎncă nu există evaluări
- Rickets Case Discussion-Dr. Venkatesh Reddy-1Document31 paginiRickets Case Discussion-Dr. Venkatesh Reddy-1DrkaleembrimsÎncă nu există evaluări
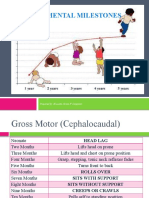
- Developmental Milestones: Prepared By: Krissette Grace F. CampilanDocument20 paginiDevelopmental Milestones: Prepared By: Krissette Grace F. CampilanshakiraÎncă nu există evaluări
- CM GRP - 8 - PresentationDocument44 paginiCM GRP - 8 - Presentationhpcdhp4wkmÎncă nu există evaluări
- Pediatric Hand Foot and Mouth Disease With Acute GastroenteritisDocument68 paginiPediatric Hand Foot and Mouth Disease With Acute GastroenteritisMelcah Marie NacionalesÎncă nu există evaluări
- Growth and DevelopmentDocument60 paginiGrowth and DevelopmentIsabel CastilloÎncă nu există evaluări
- CP MatterDocument11 paginiCP MatterShikhar SinghÎncă nu există evaluări
- Acute (1) 3Document56 paginiAcute (1) 3sivabharathijeyapaulÎncă nu există evaluări
- Anthropometry FinalDocument44 paginiAnthropometry FinalDeepthi ViswaroopanÎncă nu există evaluări
- Growth and Development in Children FinalDocument48 paginiGrowth and Development in Children FinalEricson KipronoÎncă nu există evaluări
- Konsep Pertumbuhan Dan Perkembangan Anak Infant: Blok KDK 1 A2020Document37 paginiKonsep Pertumbuhan Dan Perkembangan Anak Infant: Blok KDK 1 A2020Fajriyatul KamalÎncă nu există evaluări
- Department of Community Medicine Gandhi Medical College Under - 5 Proforma (Sam - NRC)Document4 paginiDepartment of Community Medicine Gandhi Medical College Under - 5 Proforma (Sam - NRC)kavya sriÎncă nu există evaluări
- LCC PediaDocument71 paginiLCC PedianucahersheyskatÎncă nu există evaluări
- Case Report Bacterial MeningitisDocument13 paginiCase Report Bacterial Meningitisbonziebuddy100% (1)
- AminaDocument35 paginiAminaNeethu VincentÎncă nu există evaluări
- Upgraded Parenting and Child Development GuideDocument24 paginiUpgraded Parenting and Child Development GuidedrsabarigireeshÎncă nu există evaluări
- Childs Growth DevelopmentDocument51 paginiChilds Growth Developmentmd191031Încă nu există evaluări
- DMD IE PediaDocument9 paginiDMD IE Pediamagee syÎncă nu există evaluări
- Pedia AssessmentDocument10 paginiPedia AssessmentPatel PrakrutiÎncă nu există evaluări
- 1.2. Normal Growth and DevelopmentDocument66 pagini1.2. Normal Growth and DevelopmentMUSLIHAH MD DESAÎncă nu există evaluări
- Lec 9growth and DevelopmentDocument31 paginiLec 9growth and DevelopmentUmme HabibaÎncă nu există evaluări
- Growth and DevelopmentDocument96 paginiGrowth and DevelopmentLloyd Rafael EstabilloÎncă nu există evaluări
- 001 Growth and DevelopmentDocument51 pagini001 Growth and Developmentshimeles teferaÎncă nu există evaluări
- Infectious Diseases Proforma (Child)Document4 paginiInfectious Diseases Proforma (Child)kavya sriÎncă nu există evaluări
- Growth - and - Development - of - Children (1) - 043010Document144 paginiGrowth - and - Development - of - Children (1) - 043010Abas AhmedÎncă nu există evaluări
- Growth and Devlopment of ChildrenDocument33 paginiGrowth and Devlopment of Children6krjzrgq8bÎncă nu există evaluări
- GROWTH AND DEVELOPMENT Cheet SheetDocument12 paginiGROWTH AND DEVELOPMENT Cheet SheetminisumÎncă nu există evaluări
- Zn8r8sg7tqk8womankyd Signature Poli 170526144712Document50 paginiZn8r8sg7tqk8womankyd Signature Poli 170526144712shravaniÎncă nu există evaluări
- Dengue Hemorrhagic Fever: Dian Rahayu Ningtias 030.14.052 Pembimbing: Dr. Andri Firdaus, Sp.ADocument35 paginiDengue Hemorrhagic Fever: Dian Rahayu Ningtias 030.14.052 Pembimbing: Dr. Andri Firdaus, Sp.Adirani rahmanÎncă nu există evaluări
- Growth-Developmen 2020 FKGDocument62 paginiGrowth-Developmen 2020 FKGGuuroÎncă nu există evaluări
- Undrestanding The Focus Pediatric Nursing Common TermsDocument11 paginiUndrestanding The Focus Pediatric Nursing Common Termsyasodha maharajÎncă nu există evaluări
- GrowthDocument28 paginiGrowthPriyanka AmonkarÎncă nu există evaluări
- Pharcare Human Dev.Document23 paginiPharcare Human Dev.Gracelyn GatusÎncă nu există evaluări
- Anak Stase UinDocument38 paginiAnak Stase UinSaisabelaPrmÎncă nu există evaluări
- PrefaceDocument38 paginiPrefaceAmanda PutriÎncă nu există evaluări
- Anuja Gyne CsestudyDocument11 paginiAnuja Gyne CsestudyAnuja KumariÎncă nu există evaluări
- Unit 2 Growth and Development of Children, Educational PlatformDocument131 paginiUnit 2 Growth and Development of Children, Educational Platformsufian ahmadÎncă nu există evaluări
- Case Report AnemiaDocument54 paginiCase Report AnemiahaekalÎncă nu există evaluări
- Growth &development ShaluDocument36 paginiGrowth &development ShaluNIRANJANA SHALINIÎncă nu există evaluări
- Case Presentation TWINS - 123010Document25 paginiCase Presentation TWINS - 123010Syeda AliyaÎncă nu există evaluări
- February 7 AdconDocument6 paginiFebruary 7 AdconRONALDO CUAÎncă nu există evaluări
- Fit Happens with Nutrition!: Four Weeks of Success for Every ToddlerDe la EverandFit Happens with Nutrition!: Four Weeks of Success for Every ToddlerÎncă nu există evaluări
- Morning Report: Disusun Oleh Devy Puspo WardoyoDocument35 paginiMorning Report: Disusun Oleh Devy Puspo WardoyodevyÎncă nu există evaluări
- Malignant GlaukomaDocument8 paginiMalignant GlaukomadevyÎncă nu există evaluări
- ADINDADocument36 paginiADINDAdevyÎncă nu există evaluări
- Crim - Nephrology2013 387293Document3 paginiCrim - Nephrology2013 387293devyÎncă nu există evaluări
- J Risk Factr PDFDocument4 paginiJ Risk Factr PDFdevyÎncă nu există evaluări
- Morning Report: Disusun Oleh: Ratna Ayu WulandariDocument43 paginiMorning Report: Disusun Oleh: Ratna Ayu WulandaridevyÎncă nu există evaluări
- Morning Report: Disusun Oleh Devy Puspo WardoyoDocument35 paginiMorning Report: Disusun Oleh Devy Puspo WardoyodevyÎncă nu există evaluări
- Kerajaan Mughal Kegemilangan Sejarah Islam Di IndiaDocument15 paginiKerajaan Mughal Kegemilangan Sejarah Islam Di IndiadevyÎncă nu există evaluări
- Scarlet FeverrrrrrrrrrrDocument8 paginiScarlet FeverrrrrrrrrrrdevyÎncă nu există evaluări
- Malignant GlaukomaDocument8 paginiMalignant GlaukomadevyÎncă nu există evaluări
- Graves OphthalmopathyDocument27 paginiGraves Ophthalmopathydevy100% (1)
- Morning Report: Disusun Oleh: Devy Puspo WardoyoDocument17 paginiMorning Report: Disusun Oleh: Devy Puspo WardoyodevyÎncă nu există evaluări
- CC Morning by Anik YuliaDocument22 paginiCC Morning by Anik YuliadevyÎncă nu există evaluări
- Morning Report: Disusun Oleh Devy Puspo WardoyoDocument35 paginiMorning Report: Disusun Oleh Devy Puspo WardoyodevyÎncă nu există evaluări
- Pertolongan Pertama Pada Kecelakaan Di Perusahaan: Fakultas Kedokteran Universitas Muhammadiyah Surakarta 2018Document14 paginiPertolongan Pertama Pada Kecelakaan Di Perusahaan: Fakultas Kedokteran Universitas Muhammadiyah Surakarta 2018devyÎncă nu există evaluări
- Diagnosa Sindrom NefrotikDocument10 paginiDiagnosa Sindrom NefrotikdevyÎncă nu există evaluări
- Morning Report: Disusun Oleh: Devy Puspo WardoyoDocument36 paginiMorning Report: Disusun Oleh: Devy Puspo WardoyodevyÎncă nu există evaluări
- TetanusDocument10 paginiTetanusdevyÎncă nu există evaluări
- Sindrom NefrotikDocument12 paginiSindrom NefrotikdevyÎncă nu există evaluări
- Morning Report: Disusun Oleh: Devy Puspo WardoyoDocument43 paginiMorning Report: Disusun Oleh: Devy Puspo WardoyodevyÎncă nu există evaluări
- L04 Femur Shaft ST FXDocument100 paginiL04 Femur Shaft ST FXdevyÎncă nu există evaluări
- Morning Report: Disusun Oleh: Devy Puspo WardoyoDocument17 paginiMorning Report: Disusun Oleh: Devy Puspo WardoyodevyÎncă nu există evaluări
- Morning Report: Disusun Oleh: Noermawati DewiDocument38 paginiMorning Report: Disusun Oleh: Noermawati DewidevyÎncă nu există evaluări
- Morning Report: Disusun Oleh Devy Puspo WardoyoDocument35 paginiMorning Report: Disusun Oleh Devy Puspo WardoyodevyÎncă nu există evaluări
- Morning Report: Disusun Oleh: Noermawati DewiDocument37 paginiMorning Report: Disusun Oleh: Noermawati DewidevyÎncă nu există evaluări
- Almira DiareDocument38 paginiAlmira DiaredevyÎncă nu există evaluări
- Irsya FeverDocument36 paginiIrsya FeverdevyÎncă nu există evaluări
- Irsya FeverDocument36 paginiIrsya FeverdevyÎncă nu există evaluări
- AV3 - SpeakingDocument11 paginiAV3 - SpeakingHuân MinhÎncă nu există evaluări
- American PronunciationDocument11 paginiAmerican PronunciationgptonsiÎncă nu există evaluări
- Grammar ExercisesDocument2 paginiGrammar ExercisesJ.A.I S.T.A.RÎncă nu există evaluări
- Ex234.1 Ascaris Eggz PDFDocument7 paginiEx234.1 Ascaris Eggz PDFCarlo MendozaÎncă nu există evaluări
- Visualising SiwakDocument14 paginiVisualising Siwakapi-262031303Încă nu există evaluări
- My Small and Large Intestines: © Teacher Created Resources, Inc. #211 My BodyDocument3 paginiMy Small and Large Intestines: © Teacher Created Resources, Inc. #211 My Bodyalana reneÎncă nu există evaluări
- Evaluación Física y Clínica de Sementales Bovinos en Dos Municipios de La Costa Chica de Guerrero, MéxicoDocument7 paginiEvaluación Física y Clínica de Sementales Bovinos en Dos Municipios de La Costa Chica de Guerrero, MéxicoChacharitas IxtapalucachalcoÎncă nu există evaluări
- Druid Handbook Part 3 Druid Spells ExaminedDocument30 paginiDruid Handbook Part 3 Druid Spells Examinedvtz06966Încă nu există evaluări
- Factual Report TextDocument12 paginiFactual Report TextALIEF AQIL RAZANYÎncă nu există evaluări
- Lonely Lands Throu 00 Birt I A LaDocument274 paginiLonely Lands Throu 00 Birt I A LaCarlos Costa100% (1)
- 7912 ALL TutorialsDocument41 pagini7912 ALL TutorialsHenok BayuÎncă nu există evaluări
- Thy Neighbor's Wife Chap5Document7 paginiThy Neighbor's Wife Chap5Sammymac656Încă nu există evaluări
- Rekam Anusha Et Al.Document3 paginiRekam Anusha Et Al.International Journal of Clinical and Biomedical Research (IJCBR)Încă nu există evaluări
- Khagam - A Story by Satyajit Ray - Bengaluru ReviewDocument13 paginiKhagam - A Story by Satyajit Ray - Bengaluru ReviewBarnali Saha100% (1)
- Hemostatic Derangement in DHFDocument7 paginiHemostatic Derangement in DHFnaveenÎncă nu există evaluări
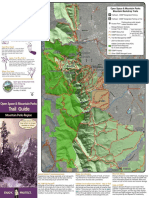
- Trail Guide: Open Space & Mountain ParksDocument2 paginiTrail Guide: Open Space & Mountain ParksKeith GruberÎncă nu există evaluări
- Hotspots Magazine - 2015-09-01Document104 paginiHotspots Magazine - 2015-09-01Holstein PlazaÎncă nu există evaluări
- UJIAN BAHASA INGGERIS - Google FormsDocument6 paginiUJIAN BAHASA INGGERIS - Google FormspzahÎncă nu există evaluări
- Embark ReportDocument28 paginiEmbark Reportapi-149926365Încă nu există evaluări
- Fossils and Dinosaurs UnitDocument45 paginiFossils and Dinosaurs UnitAJMcRostÎncă nu există evaluări
- XekendoDocument205 paginiXekendoDuncan McDermottÎncă nu există evaluări
- What Is Retained PlacentaDocument1 paginăWhat Is Retained PlacentaKitkat Aquino CabugwasÎncă nu există evaluări
- Term 2 Natural Science SaviaDocument8 paginiTerm 2 Natural Science SaviaMartabm29Încă nu există evaluări