S-ar putea să vă placă și
- Historical Develop and Issues and Trends in Health EducationDocument10 paginiHistorical Develop and Issues and Trends in Health EducationJonalyn Cielito FranciscoÎncă nu există evaluări
- Nursing As An Academic DisciplineDocument20 paginiNursing As An Academic DisciplineJules Antonette RNÎncă nu există evaluări
- CU 11. Ethico Moral and Legal Foundations of Client EducationDocument5 paginiCU 11. Ethico Moral and Legal Foundations of Client Educationcloe blancaÎncă nu există evaluări
- Theories in Health EducationDocument3 paginiTheories in Health EducationA CÎncă nu există evaluări
- Cu 2 Issues & Trends in HeDocument4 paginiCu 2 Issues & Trends in HeMichelle Gliselle Guinto MallareÎncă nu există evaluări
- TFNDocument12 paginiTFNMardina A AbdulmaulaÎncă nu există evaluări
- H.A LAB - Midterm H.ADocument6 paginiH.A LAB - Midterm H.AYep YepÎncă nu există evaluări
- 2 A Healthy CommunityDocument12 pagini2 A Healthy CommunityJmarie Brillantes PopiocoÎncă nu există evaluări
- ALL ABOUT Dorothea OremDocument4 paginiALL ABOUT Dorothea OremRosemarie R. ReyesÎncă nu există evaluări
- Health Assessment Lab Chapter 1Document3 paginiHealth Assessment Lab Chapter 1Japsay Francisco GranadaÎncă nu există evaluări
- ErikssonDocument3 paginiErikssonRoshin TejeroÎncă nu există evaluări
- 1 Institutional Nursing - Field in NursingDocument18 pagini1 Institutional Nursing - Field in NursingsannsannÎncă nu există evaluări
- Health Education PerspectiveDocument4 paginiHealth Education PerspectiveXyrelle Navarro100% (1)
- Thesis StatementDocument1 paginăThesis StatementRhaine EstebanÎncă nu există evaluări
- DiscussDocument2 paginiDiscussruthlessly_inloveÎncă nu există evaluări
- The Nurse As An EducatorDocument4 paginiThe Nurse As An EducatorAlbean DelojeroÎncă nu există evaluări
- Sub & Supra SystemDocument1 paginăSub & Supra SystemPrasanna SharmaÎncă nu există evaluări
- All Nursing TheoriesDocument26 paginiAll Nursing TheoriesMabesÎncă nu există evaluări
- Describe How The Given IT Trends Affect The FilipinoDocument2 paginiDescribe How The Given IT Trends Affect The FilipinoCarlene Joyce Aguihap100% (1)
- Principles of Teaching and Learning Related To Health Education 2019-2020Document106 paginiPrinciples of Teaching and Learning Related To Health Education 2019-2020Lyssa Marie Ege100% (2)
- NCM 104-Community Health Nursing: Prepared By: Ezra Angeli C. Joaquin, RNDocument13 paginiNCM 104-Community Health Nursing: Prepared By: Ezra Angeli C. Joaquin, RNRaRe TVÎncă nu există evaluări
- Laws Related To Family PlanningDocument17 paginiLaws Related To Family PlanningMary Chris Bacnis CabuangÎncă nu există evaluări
- Scope of Theories and AnalysisDocument10 paginiScope of Theories and AnalysismesdejenÎncă nu există evaluări
- Periods of Nursing HistoryDocument5 paginiPeriods of Nursing HistoryKrizia Cruz Gonzaga100% (1)
- Philosophical and Theoretical Foundation of Nursing: The Philippine Perspective Group 4Document20 paginiPhilosophical and Theoretical Foundation of Nursing: The Philippine Perspective Group 4Rinelky Agacid Dandasan0% (2)
- Different Views of Non-Nursing TheoriesDocument12 paginiDifferent Views of Non-Nursing Theorieskikay_nurse7850% (2)
- Acquisition of Knowledge: Combinations Learning ExperiencesDocument2 paginiAcquisition of Knowledge: Combinations Learning ExperiencesTADZMALYN JINANGÎncă nu există evaluări
- TCRLDocument16 paginiTCRLMa Ceres P Sison100% (2)
- History of Health EducationDocument3 paginiHistory of Health Education3amabelle arevaloÎncă nu există evaluări
- Assessing General Status Vital Signs 1Document20 paginiAssessing General Status Vital Signs 1Geylla FaeldoniaÎncă nu există evaluări
- STS Chapter 7 Outline and ReviewerDocument5 paginiSTS Chapter 7 Outline and ReviewerClarke MaxwellÎncă nu există evaluări
- Home Visit PDFDocument4 paginiHome Visit PDFHannahleth GorzonÎncă nu există evaluări
- Obtaing Subjective & Objective Data On Assessing Breast and Lymphatic SystemDocument8 paginiObtaing Subjective & Objective Data On Assessing Breast and Lymphatic SystemKathlyne Jhayne100% (1)
- Module 1: Foundations of Health Assessment: Lesson 1: Physical Examination and History Taking: OverviewDocument10 paginiModule 1: Foundations of Health Assessment: Lesson 1: Physical Examination and History Taking: OverviewEmily BernatÎncă nu există evaluări
- Bioethics 1Document51 paginiBioethics 1ericaÎncă nu există evaluări
- Historicism and Relativism in NursingDocument21 paginiHistoricism and Relativism in NursingJoshua Capps100% (2)
- Fundamentals of Nursing Practice-Rle A. Environmental CleaningDocument5 paginiFundamentals of Nursing Practice-Rle A. Environmental CleaningViea Pacaco SivaÎncă nu există evaluări
- GNED 02: Ethics: Second Semester, Academic Year 2022 - 2023Document23 paginiGNED 02: Ethics: Second Semester, Academic Year 2022 - 2023horizon horizonÎncă nu există evaluări
- Competency-Based Approach To The BSN CurriculumDocument23 paginiCompetency-Based Approach To The BSN CurriculumMac Paul AlariaoÎncă nu există evaluări
- Theory of Nursing Practice and Career: (Cecilia Laurente)Document33 paginiTheory of Nursing Practice and Career: (Cecilia Laurente)Erica Velasco100% (1)
- Essay Explaining My Risk Stratification and The Exercise Intensity That Fits My ClassificationDocument2 paginiEssay Explaining My Risk Stratification and The Exercise Intensity That Fits My ClassificationZia DumalagueÎncă nu există evaluări
- TFN - Joyce TravelbeeDocument8 paginiTFN - Joyce TravelbeeBenette Clare CoÎncă nu există evaluări
- LAB EXERCISE 1 Organization of The Human BodyDocument8 paginiLAB EXERCISE 1 Organization of The Human Bodyley leynÎncă nu există evaluări
- Life Perspective Rhythm Model Joyce FitzpatrickDocument44 paginiLife Perspective Rhythm Model Joyce FitzpatrickKristian Dave DivaÎncă nu există evaluări
- Script For TSB GRDDocument9 paginiScript For TSB GRDJuvel OrquinazaÎncă nu există evaluări
- 3 Target Setting Vaccine ComputationDocument5 pagini3 Target Setting Vaccine ComputationPHOEBE ANN ROCHE100% (1)
- Health Ed - Chapter 1Document29 paginiHealth Ed - Chapter 1Kevin Camiloza100% (5)
- Cardiovascular RD ScriptDocument9 paginiCardiovascular RD ScriptMary Joy Anne LucasÎncă nu există evaluări
- Open Gloving With RationaleDocument2 paginiOpen Gloving With RationaleSean Rene DuayÎncă nu există evaluări
- NCM 103 - Fundamentals of Nursing Practice M1 (PPT Notes)Document39 paginiNCM 103 - Fundamentals of Nursing Practice M1 (PPT Notes)Geylla FaeldoniaÎncă nu există evaluări
- Script Skin Hairand Nail Assessment PDFDocument5 paginiScript Skin Hairand Nail Assessment PDFKolours KoloursÎncă nu există evaluări
- TFN Notes 2ND LESSONDocument5 paginiTFN Notes 2ND LESSONAlisa FujibayashiÎncă nu există evaluări
- Collection of Objective DataDocument6 paginiCollection of Objective DataChuche Marie TumarongÎncă nu există evaluări
- Doh Health Programs (Adolescent Program)Document9 paginiDoh Health Programs (Adolescent Program)Wilma Nierva BeraldeÎncă nu există evaluări
- A.Nola Pender Nola Pender Health Promotion ModelDocument12 paginiA.Nola Pender Nola Pender Health Promotion ModelNathaniel PulidoÎncă nu există evaluări
- Health Education Team 1 2Document14 paginiHealth Education Team 1 2Mark Justin Leal0% (1)
- CHEM14LAB - Experiment 1Document10 paginiCHEM14LAB - Experiment 1Lemon AdeÎncă nu există evaluări
- Communication Processes, Principles, and Ethics: Study Guide For Module No.Document6 paginiCommunication Processes, Principles, and Ethics: Study Guide For Module No.Darlene Dacanay David100% (1)
- HEALTH EDUCATION Prelims TopicsDocument44 paginiHEALTH EDUCATION Prelims TopicsRYAN FONTANILLAÎncă nu există evaluări
- Health PromotionDocument30 paginiHealth PromotionBeverLy0% (1)
- Ni For LMSDocument10 paginiNi For LMSAmiel Francisco ReyesÎncă nu există evaluări
- Semis 2 - Drugs Acting On The Endocrine System 2Document11 paginiSemis 2 - Drugs Acting On The Endocrine System 2Amiel Francisco Reyes100% (1)
- An Overview of Nursing Informatics ..Document4 paginiAn Overview of Nursing Informatics ..Amiel Francisco ReyesÎncă nu există evaluări
- Chapter 1Document11 paginiChapter 1Amiel Francisco ReyesÎncă nu există evaluări
- NI FOR LMS CHAPTER 3 Computer SoftwareDocument6 paginiNI FOR LMS CHAPTER 3 Computer SoftwareAmiel Francisco ReyesÎncă nu există evaluări
- Semis - Nervous SystemDocument16 paginiSemis - Nervous SystemAmiel Francisco ReyesÎncă nu există evaluări
- Activity and ExerciseDocument45 paginiActivity and ExerciseAmiel Francisco ReyesÎncă nu există evaluări
- Adv of Distance LearningDocument1 paginăAdv of Distance LearningAmiel Francisco ReyesÎncă nu există evaluări
- Ni For LMS Chapter 2Document11 paginiNi For LMS Chapter 2Amiel Francisco ReyesÎncă nu există evaluări
- Temperature RegulationDocument48 paginiTemperature RegulationAmiel Francisco ReyesÎncă nu există evaluări
- OxygenationDocument56 paginiOxygenationHerald Clarence M. AmbayecÎncă nu există evaluări
- Nclex TipsDocument93 paginiNclex TipsAmiel Francisco Reyes86% (7)
- TutorialsDocument3 paginiTutorialsAmiel Francisco ReyesÎncă nu există evaluări
- Safety and SecurityDocument44 paginiSafety and SecurityAmiel Francisco ReyesÎncă nu există evaluări
- Learning TheoriesstudentsDocument4 paginiLearning TheoriesstudentsAmiel Francisco ReyesÎncă nu există evaluări
- Ra 10173Document24 paginiRa 10173Princess Villasis BaciaÎncă nu există evaluări
- Learning Theories SsDocument3 paginiLearning Theories SsAmiel Francisco ReyesÎncă nu există evaluări
- Literature Matrix Travel BehaviorDocument1 paginăLiterature Matrix Travel BehaviorAmiel Francisco ReyesÎncă nu există evaluări
- Internal Examination: Course Audit FHC Mid 2Document4 paginiInternal Examination: Course Audit FHC Mid 2Amiel Francisco ReyesÎncă nu există evaluări
- Ni Semifinals Topics 1Document7 paginiNi Semifinals Topics 1Amiel Francisco ReyesÎncă nu există evaluări
- BloomrevisedDocument9 paginiBloomrevisedAmiel Francisco ReyesÎncă nu există evaluări
- Table of The Cognitive Domain (Original)Document8 paginiTable of The Cognitive Domain (Original)Amiel Francisco ReyesÎncă nu există evaluări
- BloomrevisedDocument9 paginiBloomrevisedAmiel Francisco ReyesÎncă nu există evaluări
- Ni Semifinals Topics 2 COVID 19Document11 paginiNi Semifinals Topics 2 COVID 19Amiel Francisco ReyesÎncă nu există evaluări
- BloomrevisedDocument9 paginiBloomrevisedAmiel Francisco ReyesÎncă nu există evaluări
- Strat For HealthDocument9 paginiStrat For HealthAmiel Francisco ReyesÎncă nu există evaluări
- R-Difficult ClientsDocument15 paginiR-Difficult ClientsAmiel Francisco ReyesÎncă nu există evaluări
- Health StratDocument11 paginiHealth StratAmiel Francisco Reyes100% (1)
- Strat For HealthDocument9 paginiStrat For HealthAmiel Francisco ReyesÎncă nu există evaluări
- Health StratDocument11 paginiHealth StratAmiel Francisco Reyes100% (1)
- Customer IdentifyingDocument11 paginiCustomer Identifyinganon_363811381100% (2)
- Block Syllabus S. ST Grade 5 FIRST TERM 2024Document4 paginiBlock Syllabus S. ST Grade 5 FIRST TERM 2024fatimaijaz928Încă nu există evaluări
- Phil-IRI POST TEST Reading Selection Form A4Document6 paginiPhil-IRI POST TEST Reading Selection Form A4ariel mateo monesÎncă nu există evaluări
- Yasmin Akhtar - Speech Therapy For Kids - Libgen - LiDocument84 paginiYasmin Akhtar - Speech Therapy For Kids - Libgen - Liickng7100% (1)
- Facilitating Learning - Module 3Document171 paginiFacilitating Learning - Module 3Rema MandaÎncă nu există evaluări
- How Many Hours Should One Study To Crack The Civil Services Exam?Document27 paginiHow Many Hours Should One Study To Crack The Civil Services Exam?654321Încă nu există evaluări
- 1.3 Compare One'S Pecs With Those of A Practitioner/Entrepreneur 1.4 Align One'S Pecs With Those of A Practitioner/EntrepreneurDocument3 pagini1.3 Compare One'S Pecs With Those of A Practitioner/Entrepreneur 1.4 Align One'S Pecs With Those of A Practitioner/EntrepreneurNoli ZamoraÎncă nu există evaluări
- Grad Script of MCDocument3 paginiGrad Script of MCJunde Undang VillegasÎncă nu există evaluări
- FactorsDocument2 paginiFactorsBarbara Mercado ManiagoÎncă nu există evaluări
- Unit Test in Practical Research 11Document3 paginiUnit Test in Practical Research 11Vee Jay Solomon BlanciaÎncă nu există evaluări
- Electrodynamics by Gupta Kumar MSC PDFDocument2 paginiElectrodynamics by Gupta Kumar MSC PDFVivek Kumar0% (7)
- Aby Warburg's, Bilderatlas Mnemosyne': Systems of Knowledge and Iconography, In: Burlington Magazine 162, 2020, Pp. 1078-1083Document7 paginiAby Warburg's, Bilderatlas Mnemosyne': Systems of Knowledge and Iconography, In: Burlington Magazine 162, 2020, Pp. 1078-1083AntonisÎncă nu există evaluări
- A Unit Study On DinosaursDocument116 paginiA Unit Study On DinosaurszakkaholicÎncă nu există evaluări
- Ten Health Benefits of Getting A Good Nights SleepDocument5 paginiTen Health Benefits of Getting A Good Nights SleepAngelica CiubalÎncă nu există evaluări
- Types of ReadingDocument5 paginiTypes of ReadingfatinfiqahÎncă nu există evaluări
- Policy Brief Social MediaDocument3 paginiPolicy Brief Social MediabygskyÎncă nu există evaluări
- Capstone IdeasDocument9 paginiCapstone IdeastijunkÎncă nu există evaluări
- Impact of Emotional Intelligence and Work Life Integration On Job StressDocument10 paginiImpact of Emotional Intelligence and Work Life Integration On Job StressDr.Ramar VeluchamyÎncă nu există evaluări
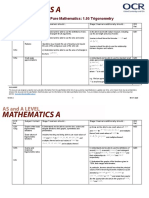
- Teacher Delivery Guide Pure Mathematics: 1.05 TrigonometryDocument16 paginiTeacher Delivery Guide Pure Mathematics: 1.05 TrigonometryHubert SelormeyÎncă nu există evaluări
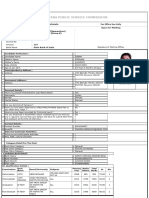
- TAHSILDAR Application FormDocument2 paginiTAHSILDAR Application FormAmit PanchalÎncă nu există evaluări
- Final - Large Book-LetDocument32 paginiFinal - Large Book-LetSanchit KarveÎncă nu există evaluări
- Room CPA July 2014 PDFDocument166 paginiRoom CPA July 2014 PDFNorman DelirioÎncă nu există evaluări
- MAS90 Consultant Resume - Brett ZimmermanDocument2 paginiMAS90 Consultant Resume - Brett ZimmermanWayne SchulzÎncă nu există evaluări
- Critical Reflective Techniques - Ilumin, Paula Joy DDocument2 paginiCritical Reflective Techniques - Ilumin, Paula Joy DPaula Joy IluminÎncă nu există evaluări
- Linda Gatwiri Kaaria CV and Cover LetterDocument5 paginiLinda Gatwiri Kaaria CV and Cover Letterbenson mwitiÎncă nu există evaluări
- 5 Steps To Use The Memory Palace TechniqueDocument6 pagini5 Steps To Use The Memory Palace TechniqueAnisha Priya De Luxe100% (1)
- Lpe2301 Academic Interaction & Presentation SEMESTER 1, 2019/2020 Lecture Notes 2 (Week 2 - 6)Document8 paginiLpe2301 Academic Interaction & Presentation SEMESTER 1, 2019/2020 Lecture Notes 2 (Week 2 - 6)Hoh Jia DaÎncă nu există evaluări
- Olugbenga's CV EngineerDocument2 paginiOlugbenga's CV EngineerSanni Tajudeen OlugbengaÎncă nu există evaluări
- Cavite State University: Cvsu Vision Cvsu MissionDocument3 paginiCavite State University: Cvsu Vision Cvsu Missionrose may batallerÎncă nu există evaluări
- IC3e Book3 To GIU-BGIU-WorkbooksDocument7 paginiIC3e Book3 To GIU-BGIU-WorkbooksTâm XinhÎncă nu există evaluări