S-ar putea să vă placă și
- Acute Appendicitis in ChildrenDocument71 paginiAcute Appendicitis in ChildrenMohamed KamaraÎncă nu există evaluări
- Blighted OvumDocument31 paginiBlighted OvumHeri FarnasÎncă nu există evaluări
- Laporan Kasus PPOKDocument23 paginiLaporan Kasus PPOKbahrinaÎncă nu există evaluări
- Internal Medicine: Dr. Nindyasari Diajeng Larasati Tim UKMPPD FKU MalahayatiDocument209 paginiInternal Medicine: Dr. Nindyasari Diajeng Larasati Tim UKMPPD FKU MalahayatiSilvi Qiro'atul AiniÎncă nu există evaluări
- Morning ReportDocument107 paginiMorning ReportMuhammad RezaÎncă nu există evaluări
- Urosepsis: Dr. Tameem Mohammed Department of Anesthesia and Intensive Care San Fernando General HospitalDocument22 paginiUrosepsis: Dr. Tameem Mohammed Department of Anesthesia and Intensive Care San Fernando General HospitalRicky AliÎncă nu există evaluări
- MANAGEMENT ACUTE ISCHEMIC STROKE (Simpo rTPA RSHS) - LisdaDocument63 paginiMANAGEMENT ACUTE ISCHEMIC STROKE (Simpo rTPA RSHS) - LisdadianÎncă nu există evaluări
- Acute Pulmonary Edema - NEJMDocument4 paginiAcute Pulmonary Edema - NEJMSuzika Dewi0% (1)
- Hipertiroid HarrisonDocument8 paginiHipertiroid HarrisonravenskaÎncă nu există evaluări
- Hypovolemic Shock and DicDocument53 paginiHypovolemic Shock and Dicapi-3743483100% (6)
- Case Report MTH HydroceleDocument9 paginiCase Report MTH Hydrocelesamuel_hildaÎncă nu există evaluări
- Hemorrhoids Case ReportDocument8 paginiHemorrhoids Case ReportTetipuspita SariÎncă nu există evaluări
- Dr. Sunatrio - Management Hypovolemic ShockDocument59 paginiDr. Sunatrio - Management Hypovolemic ShockArga Putra SaboeÎncă nu există evaluări
- Tinea CorporisDocument23 paginiTinea CorporisDita lewaherillaÎncă nu există evaluări
- Intubasi Endoktrakheal 2020Document53 paginiIntubasi Endoktrakheal 2020Octa VianiÎncă nu există evaluări
- AnestesiDocument59 paginiAnestesiJeffrey EkaÎncă nu există evaluări
- Albumin in Liver Cirrhosis, SADocument37 paginiAlbumin in Liver Cirrhosis, SADwinita ViviantiÎncă nu există evaluări
- Abdominal Pain in Children - Dr. Hermanto SP - BaDocument41 paginiAbdominal Pain in Children - Dr. Hermanto SP - Bajimmy_junÎncă nu există evaluări
- Responsi HemoroidDocument26 paginiResponsi HemoroidJessica Alexandria WuÎncă nu există evaluări
- Cme Acs 2. Stemi (Izzah)Document36 paginiCme Acs 2. Stemi (Izzah)Hakimah K. SuhaimiÎncă nu există evaluări
- Fistel Vesicovaginalis, Ureterocutaneous, Dan UreterorectalisDocument24 paginiFistel Vesicovaginalis, Ureterocutaneous, Dan Ureterorectalismizz_jcÎncă nu există evaluări
- Krisis Tiroid FixDocument38 paginiKrisis Tiroid FixVita DesriantiÎncă nu există evaluări
- HSP and ITPDocument2 paginiHSP and ITPSara Vowels-Hattaway100% (3)
- CBD Hilman Suhaili (Dr. Saugi SP - PD, KKV)Document40 paginiCBD Hilman Suhaili (Dr. Saugi SP - PD, KKV)HiLmanÎncă nu există evaluări
- Trauma Thorax Atls 9 Edition: Amatillah RaifahDocument20 paginiTrauma Thorax Atls 9 Edition: Amatillah RaifahAnnifa RaifaÎncă nu există evaluări
- PVC Stoelting Coex 1Document29 paginiPVC Stoelting Coex 1Rudy SiahaanÎncă nu există evaluări
- Omphalocele GastroschisisDocument12 paginiOmphalocele GastroschisisOlivelhynn Bernaldo100% (1)
- (INFEKSI) - FKUI - Nelwan Score Typhoid Fever.2016Document10 pagini(INFEKSI) - FKUI - Nelwan Score Typhoid Fever.2016Yolanda FitrianiÎncă nu există evaluări
- Management of Local Anaesthetic Toxicity Update 2009Document6 paginiManagement of Local Anaesthetic Toxicity Update 2009leviosagalÎncă nu există evaluări
- Laporan Kasus CHF NYHA III, Diabetes MellitusDocument42 paginiLaporan Kasus CHF NYHA III, Diabetes MellitusGitha Ayu AstarikaÎncă nu există evaluări
- Acute Limb IschaemiaDocument32 paginiAcute Limb IschaemiaAnonymous 9wHscM100% (1)
- Anginal EquivalentsDocument6 paginiAnginal EquivalentsGrant Wynn ArnucoÎncă nu există evaluări
- Clinical Aspects of PneumothoraxDocument3 paginiClinical Aspects of PneumothoraxelisabethÎncă nu există evaluări
- Apendice Maingots Abdominal Operations 12th EditionDocument26 paginiApendice Maingots Abdominal Operations 12th EditionSimonGonzalezAponteÎncă nu există evaluări
- Assessment and Initial Management Trauma PatientDocument69 paginiAssessment and Initial Management Trauma PatientdrpagrawÎncă nu există evaluări
- n378.008 Iris Website Staging of CKD PDFDocument8 paginin378.008 Iris Website Staging of CKD PDFrutebeufÎncă nu există evaluări
- Daftar Kode Diagnosa & TindakanDocument7 paginiDaftar Kode Diagnosa & Tindakannovi andriyaniÎncă nu există evaluări
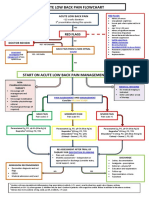
- Acute Low Back Pain Flowchart January 2017Document1 paginăAcute Low Back Pain Flowchart January 20171234chocoÎncă nu există evaluări
- JNC 6 Vs 7Document2 paginiJNC 6 Vs 7Diwan AyuÎncă nu există evaluări
- Spindle Cell TumorsDocument138 paginiSpindle Cell TumorsMadhura ShekatkarÎncă nu există evaluări
- Blighted OvumDocument4 paginiBlighted Ovummaria50% (2)
- Polycythemia Vera: Nurmaratu Thahirah Suaib C014172174Document12 paginiPolycythemia Vera: Nurmaratu Thahirah Suaib C014172174amiraÎncă nu există evaluări
- FIXED PPT Case Report EsterDocument39 paginiFIXED PPT Case Report Esterririn esterinaÎncă nu există evaluări
- Hipertensi JNC 8Document7 paginiHipertensi JNC 8Elisse StephanieÎncă nu există evaluări
- Portal HypertensionDocument60 paginiPortal HypertensionParul VarshneyÎncă nu există evaluări
- Case Report Gastritis ErosifDocument14 paginiCase Report Gastritis ErosifVela Nazar100% (1)
- Brenner Adjustment DoseDocument34 paginiBrenner Adjustment Dosecygnus112Încă nu există evaluări
- VBACDocument45 paginiVBACJuan Habli SoufalÎncă nu există evaluări
- Basic Life Support (BLS) Support (Acls) : Dan Advance Cardiac LifeDocument27 paginiBasic Life Support (BLS) Support (Acls) : Dan Advance Cardiac LifeRuth AngeliaÎncă nu există evaluări
- Kolestasis Intrahepatal Vs EkstrahepatalDocument4 paginiKolestasis Intrahepatal Vs EkstrahepatalrikarikaÎncă nu există evaluări
- LimfadenitisDocument36 paginiLimfadenitisAtikah Insani TaqwaÎncă nu există evaluări
- THT Bimbel Ukdi Mantap 2015 - NorestrictionDocument227 paginiTHT Bimbel Ukdi Mantap 2015 - NorestrictionpanduÎncă nu există evaluări
- Children With Henoch Schonlein Purpura 2.0Document13 paginiChildren With Henoch Schonlein Purpura 2.0soniaÎncă nu există evaluări
- Shock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentDocument64 paginiShock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentHarika BandaruÎncă nu există evaluări
- k.41 ATRIAL FLUTTERDocument8 paginik.41 ATRIAL FLUTTERjamaliganteng88Încă nu există evaluări
- STEMI Inferior Wall Onset 3 Hours Killip I: Dr. Juzny Alkatiri, SP - PD, SP - JP, Fiha, FinasimDocument33 paginiSTEMI Inferior Wall Onset 3 Hours Killip I: Dr. Juzny Alkatiri, SP - PD, SP - JP, Fiha, FinasimAnwar Mo SajaÎncă nu există evaluări
- Case Report: ST Segment Elevation Inferior Myocardial Infarction Onset 6 Hours Killip IDocument37 paginiCase Report: ST Segment Elevation Inferior Myocardial Infarction Onset 6 Hours Killip IFaradiba NoviandiniÎncă nu există evaluări
- Laporan Kasus StemiDocument41 paginiLaporan Kasus StemiNur Aisyah Soedarmin IieychaÎncă nu există evaluări
- Case Report:: Stemi Anteroseptal Wall OnsetDocument38 paginiCase Report:: Stemi Anteroseptal Wall OnsetAulia Azizah KosmanÎncă nu există evaluări
- Stemi Extensive Anterior LBH 24 Hour Onset Killip IDocument35 paginiStemi Extensive Anterior LBH 24 Hour Onset Killip IIta MaghfirahÎncă nu există evaluări
- Haldex Valve Catalog: Quality Parts For Vehicles at Any Life StageDocument108 paginiHaldex Valve Catalog: Quality Parts For Vehicles at Any Life Stagehoussem houssemÎncă nu există evaluări
- Game On Series BibleDocument28 paginiGame On Series Bibleapi-513832615Încă nu există evaluări
- UntitledDocument17 paginiUntitledSedat100% (1)
- 3S Why SandhyavandanDocument49 pagini3S Why SandhyavandanvivektonapiÎncă nu există evaluări
- 88 Year Old Man Missing in SC - Please ShareDocument1 pagină88 Year Old Man Missing in SC - Please ShareAmy WoodÎncă nu există evaluări
- Writing Short StoriesDocument10 paginiWriting Short StoriesRodiatun YooÎncă nu există evaluări
- UniFi Quick GuideDocument2 paginiUniFi Quick GuideAndhika TharunaÎncă nu există evaluări
- Molecules of Life PDFDocument113 paginiMolecules of Life PDFArpit Pradhan100% (1)
- AC MachinesDocument32 paginiAC Machinesjoeney guardiarioÎncă nu există evaluări
- Buy Wholesale China Popular Outdoor Football Boot For Teenagers Casual High Quality Soccer Shoes FG Ag Graffiti Style & FootballDocument1 paginăBuy Wholesale China Popular Outdoor Football Boot For Teenagers Casual High Quality Soccer Shoes FG Ag Graffiti Style & Footballjcdc9chh8dÎncă nu există evaluări
- Loch ChildrenDocument4 paginiLoch ChildrenLauro De Jesus FernandesÎncă nu există evaluări
- E Commerce and Its Influence in Changing in Purchasing Behavior of Modern ConsumersDocument13 paginiE Commerce and Its Influence in Changing in Purchasing Behavior of Modern ConsumersRichard VillanuevaÎncă nu există evaluări
- Construction of Perimeter Fence of BFP NHQ PDFDocument133 paginiConstruction of Perimeter Fence of BFP NHQ PDFYalla ChaitanyaÎncă nu există evaluări
- CA-idms Ads Alive User Guide 15.0Document142 paginiCA-idms Ads Alive User Guide 15.0svdonthaÎncă nu există evaluări
- Letter of Intent Date: 18-Feb-2019 Mr. Ravi Mishra,: For Multiplier Brand Solutions PVT LTDDocument2 paginiLetter of Intent Date: 18-Feb-2019 Mr. Ravi Mishra,: For Multiplier Brand Solutions PVT LTDRavi MishraÎncă nu există evaluări
- Tip Sheet March 2017Document2 paginiTip Sheet March 2017hoangvubui4632Încă nu există evaluări
- Content Analysis of Tea BrandsDocument49 paginiContent Analysis of Tea BrandsHumaRiaz100% (1)
- Al Multaqaa Presentation v2Document22 paginiAl Multaqaa Presentation v2Hasaan WaheedÎncă nu există evaluări
- Bank OD Account in Tally 1Document3 paginiBank OD Account in Tally 1yashusahu180Încă nu există evaluări
- Rich Gas and Lean GasDocument7 paginiRich Gas and Lean GasManish GautamÎncă nu există evaluări
- Edug 899 - Grade 2 Forces and Motion Unit - CompletedDocument37 paginiEdug 899 - Grade 2 Forces and Motion Unit - Completedapi-241358660Încă nu există evaluări
- Why Do Kashmiris Need Self-Determination?: UncategorizedDocument16 paginiWhy Do Kashmiris Need Self-Determination?: UncategorizedFarooq SiddiqiÎncă nu există evaluări
- Federal Government Employees Housing FoundationDocument2 paginiFederal Government Employees Housing FoundationMuhammad Shakil JanÎncă nu există evaluări
- Certain Application of Photovo PDFDocument235 paginiCertain Application of Photovo PDFaun_nustÎncă nu există evaluări
- Classical School of Thought: Ms. Salma ShaheenDocument62 paginiClassical School of Thought: Ms. Salma ShaheenQasim Ali100% (1)
- H I Ôn Thi Aptis & Vstep - Tài Liệu - Anna MaiDocument4 paginiH I Ôn Thi Aptis & Vstep - Tài Liệu - Anna Maihanh.mt2022Încă nu există evaluări
- Expansions Meet Health Care Needs: Economists Question Trump Plan FiguresDocument10 paginiExpansions Meet Health Care Needs: Economists Question Trump Plan FiguresThe Daily Tar HeelÎncă nu există evaluări
- DocumentationDocument44 paginiDocumentation19-512 Ratnala AshwiniÎncă nu există evaluări
- One God One People February 2013Document297 paginiOne God One People February 2013Stig DragholmÎncă nu există evaluări
- 1evolution of O and M TheoryDocument27 pagini1evolution of O and M TheoryTracy AdraÎncă nu există evaluări