S-ar putea să vă placă și
- Percutaneous Transluminal Coronary AngioplastyDocument22 paginiPercutaneous Transluminal Coronary AngioplastyArya Gaunker100% (1)
- Abg AnalysisDocument9 paginiAbg AnalysisLakshmi RjÎncă nu există evaluări
- Hemodynamic Monitoring 1Document10 paginiHemodynamic Monitoring 1Savita HanamsagarÎncă nu există evaluări
- Sister Nivedita Govt. Nursing College Igmc, ShimlaDocument10 paginiSister Nivedita Govt. Nursing College Igmc, ShimlashivaniÎncă nu există evaluări
- IV Cannulation and Fixation Infusion PumpDocument23 paginiIV Cannulation and Fixation Infusion PumpUday Kumar0% (1)
- Inhalation or Aerosols Therapy1Document21 paginiInhalation or Aerosols Therapy1drnasir31Încă nu există evaluări
- Assignment ON: TOPIC: PTCA (Percutaneous Transluminous Coronary Angioplasty)Document7 paginiAssignment ON: TOPIC: PTCA (Percutaneous Transluminous Coronary Angioplasty)soniya josephÎncă nu există evaluări
- BVCCT-501 Cardiac Catheterization Laboratory BasicsDocument52 paginiBVCCT-501 Cardiac Catheterization Laboratory BasicsManisha khan100% (1)
- Case Study On PacemakersDocument6 paginiCase Study On PacemakersBalamuruganÎncă nu există evaluări
- Bone Marrow AspirationDocument43 paginiBone Marrow AspirationDr. Pawan KumarÎncă nu există evaluări
- 0347burst AbdomenDocument24 pagini0347burst AbdomenSathishKumar100% (1)
- Nasogastric Aspiration: Preparation of ArticlesDocument2 paginiNasogastric Aspiration: Preparation of ArticlesVarun ToshniwalÎncă nu există evaluări
- Centrel Venous CatheterizationDocument77 paginiCentrel Venous CatheterizationAli100% (1)
- Cardiac MonitoringDocument6 paginiCardiac MonitoringAIMÎncă nu există evaluări
- ETT IntubationDocument10 paginiETT IntubationPoova RagavanÎncă nu există evaluări
- Lumbar PunctureDocument18 paginiLumbar PunctureJaspreet KangÎncă nu există evaluări
- Atrial Septal DefectDocument3 paginiAtrial Septal Defectmu_crÎncă nu există evaluări
- Blood Transfusion PDFDocument7 paginiBlood Transfusion PDFBaboolal100% (2)
- Assisting Central Venous Catheter (CVC) Insertion (Procedure1)Document7 paginiAssisting Central Venous Catheter (CVC) Insertion (Procedure1)BsBs A7medÎncă nu există evaluări
- Sub - Medical Surgical Nursing: Assignment On CVP MonitoringDocument11 paginiSub - Medical Surgical Nursing: Assignment On CVP Monitoringkamini ChoudharyÎncă nu există evaluări
- Lumbar Puncture (LP)Document10 paginiLumbar Puncture (LP)Fady Jehad ZabenÎncă nu există evaluări
- Angiography: Presented By: Mulituba, Nairah DDocument9 paginiAngiography: Presented By: Mulituba, Nairah DAkazukin AineÎncă nu există evaluări
- Allen's TestDocument8 paginiAllen's TestJustineMaeMadroñalÎncă nu există evaluări
- Defibrillation TypedDocument8 paginiDefibrillation TypedValarmathiÎncă nu există evaluări
- Bone Marrow AspirationDocument2 paginiBone Marrow AspirationJClaudz PilapilÎncă nu există evaluări
- ANGIOGRAPHYDocument8 paginiANGIOGRAPHYAkazukin AineÎncă nu există evaluări
- Heart Block: BY DR - AriyalakshmiDocument26 paginiHeart Block: BY DR - AriyalakshmiDiksha chaudharyÎncă nu există evaluări
- On Emergency DrugsDocument25 paginiOn Emergency DrugsBikram Chhetry100% (1)
- Chest TraumaDocument79 paginiChest TraumaAnusha VergheseÎncă nu există evaluări
- Monitoring of Critically Ill PatientDocument11 paginiMonitoring of Critically Ill PatientAnusikta PandaÎncă nu există evaluări
- Bone Marrow AspirationDocument6 paginiBone Marrow AspirationSai PardhuÎncă nu există evaluări
- Dialyzer Reprocessing Flow ChartDocument1 paginăDialyzer Reprocessing Flow ChartGrafe ChuaÎncă nu există evaluări
- Preparation For EndosDocument17 paginiPreparation For EndoscsngiuÎncă nu există evaluări
- Cardio Pulmonary ResuscitationDocument13 paginiCardio Pulmonary Resuscitationaparna100% (1)
- Needle Cricothyroidotomy 2 - Hatem AlsrourDocument32 paginiNeedle Cricothyroidotomy 2 - Hatem Alsrourhatem alsrour100% (2)
- Cardiac MonitoringDocument5 paginiCardiac MonitoringAmit Kl100% (1)
- Central Venous Pressure Monitoring ManualDocument6 paginiCentral Venous Pressure Monitoring ManualCristina L. JaysonÎncă nu există evaluări
- Disorders of AortaDocument25 paginiDisorders of Aortavani reddyÎncă nu există evaluări
- SP42 Thoracentesis (Adult)Document7 paginiSP42 Thoracentesis (Adult)Adam HuzaibyÎncă nu există evaluări
- Lesson Plan BMA&BDocument14 paginiLesson Plan BMA&BLoma Waghmare (Jadhav)Încă nu există evaluări
- Cardio Vascular Assessment: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingDocument46 paginiCardio Vascular Assessment: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingmeghanaÎncă nu există evaluări
- Aetiology Heart Diasease in Children May Be Congenital or AcquiredDocument23 paginiAetiology Heart Diasease in Children May Be Congenital or AcquiredkasondaÎncă nu există evaluări
- Medical-Surgical EmergenciesDocument78 paginiMedical-Surgical EmergenciesGopala Hari100% (8)
- Equipment EditedDocument6 paginiEquipment EditedCHRISTINE JOY. MOLINAÎncă nu există evaluări
- Seminar On PacemakerDocument14 paginiSeminar On Pacemakerjyothi50% (4)
- Advanced Cardiac ProcedureDocument9 paginiAdvanced Cardiac ProcedureSachin DwivediÎncă nu există evaluări
- OT Equipments: Hold The Highest Standard With Best Pieces of EquipmentsDocument71 paginiOT Equipments: Hold The Highest Standard With Best Pieces of Equipmentsradhika333100% (1)
- VentilatorDocument9 paginiVentilatorSheeba StephenÎncă nu există evaluări
- Institute of Nursing and Allied Health SciencesDocument2 paginiInstitute of Nursing and Allied Health Sciencesshadow gonzalezÎncă nu există evaluări
- Pulse Oximetry IDocument4 paginiPulse Oximetry IFriends Forever100% (1)
- Purbanchal University Shree Medical and Technical College Bharatpur 10, ChitwanDocument10 paginiPurbanchal University Shree Medical and Technical College Bharatpur 10, Chitwansushma shresthaÎncă nu există evaluări
- Bone Marrow Aspiration and BiopsyDocument2 paginiBone Marrow Aspiration and Biopsyprince10120% (1)
- ThoracentesisDocument4 paginiThoracentesisCyntia Theresia Lumintang100% (1)
- Care of Chest Tube Drainage & Nursing Manangement SHDocument82 paginiCare of Chest Tube Drainage & Nursing Manangement SHJoanna RemollinoÎncă nu există evaluări
- Procedural Checklist For Care of TracheostomyDocument2 paginiProcedural Checklist For Care of TracheostomyAbegail TabuniagÎncă nu există evaluări
- PericarditisDocument45 paginiPericarditisBrenda WardshoneÎncă nu există evaluări
- Mitral Stenosis: Dr. Mohammed Asrafur Rahman MBBS, Bcs (H), MD Resident (Internal Medicine) (P-A) Chattogram Medical CollegeDocument16 paginiMitral Stenosis: Dr. Mohammed Asrafur Rahman MBBS, Bcs (H), MD Resident (Internal Medicine) (P-A) Chattogram Medical CollegeAsrafur RahmanÎncă nu există evaluări
- Arterial LineDocument2 paginiArterial LineRaghav Goyal100% (1)
- Lumbar PunctureDocument27 paginiLumbar PunctureWitneyGrace100% (1)
- PericardiocintesisDocument20 paginiPericardiocintesisKarelau KarniaÎncă nu există evaluări
- Dolor CVNADocument15 paginiDolor CVNAStephania MendozaÎncă nu există evaluări
- Paper Lips1Document11 paginiPaper Lips1dominiqueÎncă nu există evaluări
- Male Catheterization (Indwelling)Document43 paginiMale Catheterization (Indwelling)Dan Floyd FernandezÎncă nu există evaluări
- Digestive SystemDocument10 paginiDigestive SystemLindsay AnquiloÎncă nu există evaluări
- DR Sourabh Patwardhan's Phaco Handbook Ed 1-2Document106 paginiDR Sourabh Patwardhan's Phaco Handbook Ed 1-2Nounzia Boucherit BoubekriÎncă nu există evaluări
- AIIMS Nursing Officer Question Paper With Key 2019-1Document35 paginiAIIMS Nursing Officer Question Paper With Key 2019-1shubham vermaÎncă nu există evaluări
- Data Sarana PrasaranaDocument18 paginiData Sarana PrasaranaFlora Indah FajarwattyÎncă nu există evaluări
- Terminologi Kedokteran Patologi KlinikDocument12 paginiTerminologi Kedokteran Patologi KlinikchristobawelleÎncă nu există evaluări
- Total Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Post-OperativeDocument2 paginiTotal Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Post-OperativeMiar QuestÎncă nu există evaluări
- Meta 4 - de Jong DM - 2022Document13 paginiMeta 4 - de Jong DM - 2022matheus.verasÎncă nu există evaluări
- Retinoblastoma and Management - A Post-Graduate Pocket Book Manjandavida FPDocument18 paginiRetinoblastoma and Management - A Post-Graduate Pocket Book Manjandavida FPSyeda F AmbreenÎncă nu există evaluări
- Esthetic Depigmentation of Anterior Gingiva: A Case: Indian Dental JournalDocument3 paginiEsthetic Depigmentation of Anterior Gingiva: A Case: Indian Dental JournalSaatvik AtriÎncă nu există evaluări
- 45 Min FibulaDocument3 pagini45 Min FibulaTor ChiuÎncă nu există evaluări
- Signs and Symptoms Of: How Does Your Kidneys Do?Document2 paginiSigns and Symptoms Of: How Does Your Kidneys Do?Afia TawiahÎncă nu există evaluări
- Impression HonigumDocument4 paginiImpression Honigumandrian_10Încă nu există evaluări
- Radiology Dissertation TopicsDocument4 paginiRadiology Dissertation TopicsWriteMyPaperForCheapCanada100% (1)
- Sesap16 Volume 1Document459 paginiSesap16 Volume 1Kamil Hanna0% (1)
- Operative Exam Questions DR Hatem Sahar 2012-2013Document2 paginiOperative Exam Questions DR Hatem Sahar 2012-2013Abdallah GamalÎncă nu există evaluări
- 133-Article Text-648-3-10-20190525 PDFDocument6 pagini133-Article Text-648-3-10-20190525 PDFyantiÎncă nu există evaluări
- Mitsuo Ochi, Konsei Shino, Kazunori Yasuda, Masahiro Kurosaka (Eds.) - ACL Injury and Its Treatment-Springer Japan (2016) PDFDocument546 paginiMitsuo Ochi, Konsei Shino, Kazunori Yasuda, Masahiro Kurosaka (Eds.) - ACL Injury and Its Treatment-Springer Japan (2016) PDFdrbaneÎncă nu există evaluări
- Cardiac Catheterization and Coronary AngiographyDocument5 paginiCardiac Catheterization and Coronary Angiographyedem100% (1)
- Nurs 603 Assignment 2Document6 paginiNurs 603 Assignment 2api-429205355Încă nu există evaluări
- Cardiac Surgery Basic KnowledgeDocument28 paginiCardiac Surgery Basic KnowledgeGinwong100% (1)
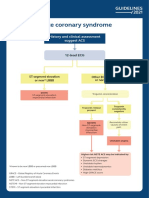
- Acute Coronary Syndrome: History and Clinical Assessment Suggest ACSDocument12 paginiAcute Coronary Syndrome: History and Clinical Assessment Suggest ACSginongÎncă nu există evaluări
- CraniotomyDocument10 paginiCraniotomyUzma KhanÎncă nu există evaluări
- Extensor Tendon InjuriesDocument35 paginiExtensor Tendon InjuriesPk Nutsuklo100% (1)
- Anatomy Lower LimbDocument4 paginiAnatomy Lower Limbch yaqoobÎncă nu există evaluări
- MCQ 123Document13 paginiMCQ 123Satya Asatya67% (3)
- Indravati PCPNDT 2 MoDocument6 paginiIndravati PCPNDT 2 MoDr Sachin Chitnis M O UPHC AiroliÎncă nu există evaluări
- Procedure Guide For Bag Technique Part 3Document2 paginiProcedure Guide For Bag Technique Part 3CrishaGarraÎncă nu există evaluări