S-ar putea să vă placă și
- Unit 1 - Respiration - Reference Material - Shared in GCDocument7 paginiUnit 1 - Respiration - Reference Material - Shared in GCTarunÎncă nu există evaluări
- Transparency 2Document11 paginiTransparency 2nitesh tirkeyÎncă nu există evaluări
- Respiration NotesDocument7 paginiRespiration NotesKrishna SharmaÎncă nu există evaluări
- Breathing and Exchange of GasesDocument17 paginiBreathing and Exchange of GasesArjun ChristopherÎncă nu există evaluări
- Respiratory and Circulatory SystemDocument10 paginiRespiratory and Circulatory Systemainabukhari20Încă nu există evaluări
- Respiratory SystemDocument31 paginiRespiratory SystemMark Jhosua Austria GalinatoÎncă nu există evaluări
- Class 7 RespirationDocument5 paginiClass 7 RespirationGopi SÎncă nu există evaluări
- Study Materials: Vedantu Innovations Pvt. Ltd. Score High With A Personal Teacher, Learn LIVE Online!Document17 paginiStudy Materials: Vedantu Innovations Pvt. Ltd. Score High With A Personal Teacher, Learn LIVE Online!Saraswati PÎncă nu există evaluări
- Notes 1Document12 paginiNotes 1Muhammad TaimoorÎncă nu există evaluări
- PDBreathing and Exchange of Gases Class 11 Notes CBSE Biology Chapter 17FDocument15 paginiPDBreathing and Exchange of Gases Class 11 Notes CBSE Biology Chapter 17Fgandhitirth147Încă nu există evaluări
- Breathing Process PDFDocument3 paginiBreathing Process PDFDianeÎncă nu există evaluări
- ScienceDocument3 paginiScienceVaughn Siegfried FuertezÎncă nu există evaluări
- Respiratory System: (A Written Report)Document16 paginiRespiratory System: (A Written Report)hellofrom theothersideÎncă nu există evaluări
- ApbioprojectDocument5 paginiApbioprojectAshleyÎncă nu există evaluări
- Human Respiratory System Aniket DasDocument11 paginiHuman Respiratory System Aniket DasChep KepÎncă nu există evaluări
- Respiratory System in Human BeingsDocument11 paginiRespiratory System in Human BeingsSarada KasyapÎncă nu există evaluări
- Anatomy and PhysiologyDocument5 paginiAnatomy and PhysiologymalindaÎncă nu există evaluări
- Respiratory SystemDocument10 paginiRespiratory Systemapi-272862164100% (1)
- Gas Exchange Written ReportDocument11 paginiGas Exchange Written ReportEllanny GloriaÎncă nu există evaluări
- ReproductiveDocument5 paginiReproductiveJason Vinluan CarinanÎncă nu există evaluări
- Human Respiratory SystemDocument13 paginiHuman Respiratory SystemKarma DemaÎncă nu există evaluări
- Respiration Is A Chemical Reaction That Happens in All Living CellsDocument3 paginiRespiration Is A Chemical Reaction That Happens in All Living CellsKani KurmanbekovaÎncă nu există evaluări
- Human Biology: Respiratory SystemDocument33 paginiHuman Biology: Respiratory SystemSaikrishna RaoÎncă nu există evaluări
- Research PaperDocument14 paginiResearch PaperAlicia ValverdeÎncă nu există evaluări
- The Respiratory System-11 By:-Dr. Hazim AL-RawiDocument12 paginiThe Respiratory System-11 By:-Dr. Hazim AL-RawiDrAli Al-FendiÎncă nu există evaluări
- Boundless Biology Respiratory SystemDocument7 paginiBoundless Biology Respiratory SystemZackary TsangÎncă nu există evaluări
- Anatomy and PhysiologyDocument11 paginiAnatomy and Physiologyjawn09euclidÎncă nu există evaluări
- Olugbade Physiology AssignmentDocument9 paginiOlugbade Physiology Assignmentolugbaded3Încă nu există evaluări
- Anatomy and Physiology: Biological System Organs Respiration Organism Exchange Oxygen Carbon DioxideDocument3 paginiAnatomy and Physiology: Biological System Organs Respiration Organism Exchange Oxygen Carbon DioxideAngie MandeoyaÎncă nu există evaluări
- Body SystemDocument15 paginiBody SystemChris Timothy TurdanesÎncă nu există evaluări
- Plant and Animal Organ System and Their FunctionDocument21 paginiPlant and Animal Organ System and Their FunctionJovon GuyoÎncă nu există evaluări
- The Respiratory SystemDocument21 paginiThe Respiratory SystemAditya PrasadÎncă nu există evaluări
- Respiratory SystemDocument54 paginiRespiratory SystemALYZZA JANE BUNAÎncă nu există evaluări
- Gas Exchange System SAT ContentDocument3 paginiGas Exchange System SAT ContentJohn Osborne100% (1)
- Organs in The Respiratory SystemDocument12 paginiOrgans in The Respiratory SystemMaeg John CareeonÎncă nu există evaluări
- Chapter II - Respiratory SystemDocument3 paginiChapter II - Respiratory SystemIndranil SinhaÎncă nu există evaluări
- Respiratory System PreDocument11 paginiRespiratory System PrecontehamosaÎncă nu există evaluări
- Parts and Functions of Respiratory System.Document3 paginiParts and Functions of Respiratory System.Alvin Patrick Colobong AsisÎncă nu există evaluări
- Respiratory System: Respiration (Oxidation of Food in Cells Cellular Respiration Energy Is Produced Along With WaterDocument15 paginiRespiratory System: Respiration (Oxidation of Food in Cells Cellular Respiration Energy Is Produced Along With WaterShuvanjan DahalÎncă nu există evaluări
- Group1 Review of Respiratory SystemDocument41 paginiGroup1 Review of Respiratory Systemjohn obinaÎncă nu există evaluări
- Animal Physiology and Physiological Chemistry Paper Mzo503 Paper Mzo503Document19 paginiAnimal Physiology and Physiological Chemistry Paper Mzo503 Paper Mzo503Abhishek Singh ChandelÎncă nu există evaluări
- The Respiratory SystemDocument28 paginiThe Respiratory SystemJuma SammyÎncă nu există evaluări
- Respiratory SystemDocument3 paginiRespiratory SystemjoimaciascorreaÎncă nu există evaluări
- Unit 7 The Respiratory System: Learning OutcomesDocument9 paginiUnit 7 The Respiratory System: Learning OutcomesDeolita BadiangÎncă nu există evaluări
- Gaseous Exchange: Short Question AnswersDocument5 paginiGaseous Exchange: Short Question AnswersNadeem ArainÎncă nu există evaluări
- Resumen Primera Parte. FisiologíaDocument4 paginiResumen Primera Parte. FisiologíaFatima AzaleansÎncă nu există evaluări
- Respiratory System Anatomy, Assessment & Diagnostic TestsDocument24 paginiRespiratory System Anatomy, Assessment & Diagnostic TestsPrince Rener Velasco PeraÎncă nu există evaluări
- Respiratory System - Anatomy and PhysiologyDocument6 paginiRespiratory System - Anatomy and PhysiologyJay Crishnan Morales CajandingÎncă nu există evaluări
- Parts and Functions of Respiratory SystemDocument18 paginiParts and Functions of Respiratory Systemjosephabram051590Încă nu există evaluări
- Anatomy and Physiology: Upper Respiratory TractDocument3 paginiAnatomy and Physiology: Upper Respiratory TractAltea MartirezÎncă nu există evaluări
- Respiratory System NotesDocument4 paginiRespiratory System NotesFlare FlareonÎncă nu există evaluări
- Gas Exchange in AnimalsDocument20 paginiGas Exchange in AnimalsMaria Theresa HerreroÎncă nu există evaluări
- Anatomy and Physiology Power PointDocument8 paginiAnatomy and Physiology Power PointJoanna Diongson GonzalesÎncă nu există evaluări
- Respiratory System: Anatomy of Respiratory Organs and Their FunctionsDocument6 paginiRespiratory System: Anatomy of Respiratory Organs and Their FunctionsRishabh SharmaÎncă nu există evaluări
- Anatomy and Physiology of The Respiratory SystemDocument5 paginiAnatomy and Physiology of The Respiratory SystemxoxosvwÎncă nu există evaluări
- Anatomy and Physiology: PHYSIOLOGY-the Branch of Biology That Deals With The Internal Workings ofDocument4 paginiAnatomy and Physiology: PHYSIOLOGY-the Branch of Biology That Deals With The Internal Workings ofshonievin100% (2)
- Introduction To Respiratory SystemDocument21 paginiIntroduction To Respiratory Systemangel demonyoÎncă nu există evaluări
- Human Respiratory System FunctionsDocument2 paginiHuman Respiratory System Functionsapi-169639475Încă nu există evaluări
- Human Body Book | Introduction to the Respiratory System | Children's Anatomy & Physiology EditionDe la EverandHuman Body Book | Introduction to the Respiratory System | Children's Anatomy & Physiology EditionÎncă nu există evaluări
- Human Respiratory SystemDocument15 paginiHuman Respiratory Systempraneeth satishÎncă nu există evaluări
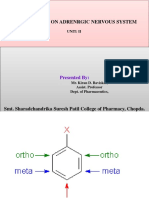
- Drugs Acting On Adrenrgic Nervous System: Presented byDocument63 paginiDrugs Acting On Adrenrgic Nervous System: Presented byKiranÎncă nu există evaluări
- Five Kingdom System-KDBDocument39 paginiFive Kingdom System-KDBKiranÎncă nu există evaluări
- Anticholinergic DrugsDocument14 paginiAnticholinergic DrugsKiranÎncă nu există evaluări
- Antipsychotics: Presented byDocument21 paginiAntipsychotics: Presented byKiranÎncă nu există evaluări
- Cholinergic DrugsDocument29 paginiCholinergic DrugsKiranÎncă nu există evaluări
- Nutrition KDBDocument104 paginiNutrition KDBKiranÎncă nu există evaluări
- Circulation KDBDocument41 paginiCirculation KDBKiranÎncă nu există evaluări
- Theory of Acid Base IndicatorDocument8 paginiTheory of Acid Base IndicatorKiranÎncă nu există evaluări
- Excretion KDBDocument82 paginiExcretion KDBKiranÎncă nu există evaluări
- Redox Titration KDBDocument45 paginiRedox Titration KDBKiranÎncă nu există evaluări
- Gravimetry - KDBDocument37 paginiGravimetry - KDBKiranÎncă nu există evaluări
- Ultrastructure of Bacteria - KDBDocument34 paginiUltrastructure of Bacteria - KDBKiranÎncă nu există evaluări
- Priamary Secondary Standard-KDBDocument12 paginiPriamary Secondary Standard-KDBKiranÎncă nu există evaluări
- Acid Base Titration KDBDocument9 paginiAcid Base Titration KDBKiranÎncă nu există evaluări
- Smt. Sharadchandrika Suresh Patil College of Pharmacy, ChopdaDocument46 paginiSmt. Sharadchandrika Suresh Patil College of Pharmacy, ChopdaKiranÎncă nu există evaluări
- Priamary Secondary Standard-KDBDocument12 paginiPriamary Secondary Standard-KDBKiranÎncă nu există evaluări
- Complexationtitration KDBDocument31 paginiComplexationtitration KDBKiranÎncă nu există evaluări
- Microbiological Assay KDBDocument11 paginiMicrobiological Assay KDBKiran0% (1)
- Validation of Sterilization - KDBDocument15 paginiValidation of Sterilization - KDBKiran100% (1)
- Design of Aseptic Area-KDBDocument21 paginiDesign of Aseptic Area-KDBKiran0% (1)
- Design of Aseptic Area-KDBDocument21 paginiDesign of Aseptic Area-KDBKiran0% (1)
- Design of Aseptic Area-KDBDocument21 paginiDesign of Aseptic Area-KDBKiran0% (1)
- Antiseptic and Disinfectant-KDBDocument43 paginiAntiseptic and Disinfectant-KDBKiran100% (3)
- Antiseptic and Disinfectant-KDBDocument43 paginiAntiseptic and Disinfectant-KDBKiran100% (3)
- (Advait) Pranayama The Vedic Science of BreathDocument76 pagini(Advait) Pranayama The Vedic Science of BreathASHISH K ADIGAÎncă nu există evaluări
- NUR100 Sherpath Oxygenation and PerfusionDocument17 paginiNUR100 Sherpath Oxygenation and Perfusioncaloy2345caloyÎncă nu există evaluări
- University of Cambridge International Examinations General Certificate of Education Ordinary LevelDocument16 paginiUniversity of Cambridge International Examinations General Certificate of Education Ordinary Levelmstudy123456Încă nu există evaluări
- The Telluric BreathingDocument7 paginiThe Telluric BreathingRebeccaLangford100% (1)
- Huna BreathingDocument14 paginiHuna BreathingHendrawan Huang100% (10)
- Respiratory SystemDocument19 paginiRespiratory SystemayuÎncă nu există evaluări
- SwimmingDocument19 paginiSwimmingCheaÎncă nu există evaluări
- NCP Impaired Gas Exhange Related To Alveolar Wall Destruction EMPHYSEMADocument5 paginiNCP Impaired Gas Exhange Related To Alveolar Wall Destruction EMPHYSEMAMa. Elaine Carla Tating50% (2)
- Lung Volumes and CapacitiesDocument15 paginiLung Volumes and CapacitiesAnn Michelle Tarrobago100% (1)
- Asthma BrochureDocument2 paginiAsthma BrochureRex Arisugawa100% (3)
- Battista, Lamperti - The Techniques of Bel Canto - Feherebb LapDocument48 paginiBattista, Lamperti - The Techniques of Bel Canto - Feherebb Lapnapfenyem97% (31)
- MCQ Medical Electronics Question BankDocument47 paginiMCQ Medical Electronics Question BankBALAJI VENKATRAMAN100% (1)
- BLS For TeacherrDocument166 paginiBLS For TeacherrGavinKarl Mianabanatao100% (1)
- Eyezercise Free E-Book: 10 Supplemental Eye ExercisesDocument15 paginiEyezercise Free E-Book: 10 Supplemental Eye ExercisesheavykickerÎncă nu există evaluări
- Ventilator: CCV-700B User'S ManualDocument25 paginiVentilator: CCV-700B User'S ManualBashir MtwaklÎncă nu există evaluări
- Spirometry ReportDocument11 paginiSpirometry ReportTharshini_Indr_6713100% (1)
- The DORN - Self Help ExerciseDocument11 paginiThe DORN - Self Help Exerciseyansol100% (1)
- English February TeeVo 2024Document84 paginiEnglish February TeeVo 2024scrapicocov8100% (1)
- Principles of Mechanical Ventilation: RET 2284 Classification of Ventilators How A Breath Is DeliveredDocument51 paginiPrinciples of Mechanical Ventilation: RET 2284 Classification of Ventilators How A Breath Is DeliveredArnaldo SantizoÎncă nu există evaluări
- Kriyayoga TecniquesDocument102 paginiKriyayoga TecniquesAmit SharmaÎncă nu există evaluări
- Circulation and RespirationDocument39 paginiCirculation and RespirationeriÎncă nu există evaluări
- Bagh College of Arts and Modern Sciences: 1 GST Test ObjectiveDocument2 paginiBagh College of Arts and Modern Sciences: 1 GST Test ObjectiveAbdul Waheed KhawajaÎncă nu există evaluări
- 8BreathingExercises Calmhappyhealthy PDFDocument10 pagini8BreathingExercises Calmhappyhealthy PDFlunn100% (1)
- 6.0 Biology Lab ManualDocument49 pagini6.0 Biology Lab ManualJacob SmithÎncă nu există evaluări
- Power Breathing Breathe Your Way To Inner Power (2008)Document264 paginiPower Breathing Breathe Your Way To Inner Power (2008)Pk100% (2)
- Philips Respironics V680 VentilatorDocument4 paginiPhilips Respironics V680 VentilatorZuley Hurtado HernandezÎncă nu există evaluări
- CARESCAPE R860 Ventilator Quick Guide JB77395XXzDocument16 paginiCARESCAPE R860 Ventilator Quick Guide JB77395XXzlusun dhakalÎncă nu există evaluări
- Human Organ Systems and Bio-Designs - 2: at Myintuition4865Document8 paginiHuman Organ Systems and Bio-Designs - 2: at Myintuition48651NC21IS038 POLATHALA MOUNIKAÎncă nu există evaluări
- Pranic Healing PrinciplesDocument10 paginiPranic Healing Principlesapi-26172340Încă nu există evaluări
- MCQ RespiratoryDocument6 paginiMCQ Respiratorynurulhudaabdulmuiez100% (2)