S-ar putea să vă placă și
- Testicular Self ExaminationDocument3 paginiTesticular Self ExaminationEmman Ramos100% (1)
- Lab Guide: Musculoskeletal AssessmentDocument6 paginiLab Guide: Musculoskeletal AssessmentDaisy MellaÎncă nu există evaluări
- What Is Epilepsy?Document10 paginiWhat Is Epilepsy?RegineCuasSulibÎncă nu există evaluări
- Pancreatitis: Def Pancreatitis (Inflammation of The Pancreas) Is A Serious Disorder. The Most Basic Classification SystemDocument5 paginiPancreatitis: Def Pancreatitis (Inflammation of The Pancreas) Is A Serious Disorder. The Most Basic Classification SystemSanthu Su100% (2)
- Pulmonary Function TestsDocument2 paginiPulmonary Function TestsSafuan Sudin100% (1)
- Acute Pancreatitis NOTESDocument17 paginiAcute Pancreatitis NOTESsameeha semiÎncă nu există evaluări
- Prepared by Inzar Yasin Ammar LabibDocument47 paginiPrepared by Inzar Yasin Ammar LabibdiaÎncă nu există evaluări
- PERITONITSDocument3 paginiPERITONITSjyoti kundu100% (1)
- Cardiovascular System Diseases Part 2Document9 paginiCardiovascular System Diseases Part 2Prince Rener Velasco PeraÎncă nu există evaluări
- B M W M: IO Edical Aste AnagementDocument23 paginiB M W M: IO Edical Aste AnagementJishnu JohnÎncă nu există evaluări
- Adrenal Crisis FinalDocument10 paginiAdrenal Crisis FinalAmanda Scarlet100% (1)
- Hemodynamic MonitoringDocument4 paginiHemodynamic Monitoringgurneet kourÎncă nu există evaluări
- Thoracotomy: T.Sunil KumarDocument59 paginiThoracotomy: T.Sunil KumarYamini ChowdaryÎncă nu există evaluări
- Friday Problem Statement PresentationDocument7 paginiFriday Problem Statement PresentationyashramawatÎncă nu există evaluări
- Renal TransplantationDocument50 paginiRenal Transplantationregie cuaresmaÎncă nu există evaluări
- Nursing Care of Patients With Cardiac ProblemsDocument125 paginiNursing Care of Patients With Cardiac ProblemsAyeÎncă nu există evaluări
- HT CvaDocument10 paginiHT CvaTopeshwar TpkÎncă nu există evaluări
- Congestive Cardiac FailureDocument20 paginiCongestive Cardiac FailureAnand VaghasiyaÎncă nu există evaluări
- Perforated PeritonitisDocument5 paginiPerforated PeritonitisDeepak singh ratheeÎncă nu există evaluări
- Abdominal ParacentesisDocument5 paginiAbdominal ParacentesisVijith.V.kumar100% (1)
- Exercise Stress TestingDocument18 paginiExercise Stress TestingSereinÎncă nu există evaluări
- Ards PDFDocument2 paginiArds PDFgireeshsachinÎncă nu există evaluări
- Unit 1Document16 paginiUnit 1reeta yadav0% (1)
- Diabetic KetoacidosisDocument4 paginiDiabetic KetoacidosisAbigael Patricia Gutierrez100% (1)
- Rheumatoid ArthritisDocument38 paginiRheumatoid ArthritisOlga GoryachevaÎncă nu există evaluări
- Fluid and Electrolytes Replacement TherapyDocument49 paginiFluid and Electrolytes Replacement TherapyMarife MartinÎncă nu există evaluări
- Thyroid CrisisDocument11 paginiThyroid CrisisKoka KolaÎncă nu există evaluări
- Compartment SyndromeDocument3 paginiCompartment SyndromeTantyo Adi P100% (2)
- Oxygen InhalationDocument4 paginiOxygen InhalationJasdeep KaurÎncă nu există evaluări
- Case Study About: Cardiac Failure and Pulmonary EdemaDocument32 paginiCase Study About: Cardiac Failure and Pulmonary EdemaIan Simon DorojaÎncă nu există evaluări
- GI - Anatomy To DiagnosticsDocument39 paginiGI - Anatomy To DiagnosticsIvan FernandezÎncă nu există evaluări
- Administration of Inotropes Evidence Based Nursing PolicyDocument8 paginiAdministration of Inotropes Evidence Based Nursing PolicyRonald ThakorÎncă nu există evaluări
- Effectiveness of Structured Teaching Programme On Knowledge Regarding Acid Peptic Disease and Its Prevention Among The Industrial WorkersDocument6 paginiEffectiveness of Structured Teaching Programme On Knowledge Regarding Acid Peptic Disease and Its Prevention Among The Industrial WorkersIJAR JOURNALÎncă nu există evaluări
- Colostomy CareDocument4 paginiColostomy CareRhenzes HaraÎncă nu există evaluări
- Thrombolytic TherapyDocument37 paginiThrombolytic TherapySani sunilÎncă nu există evaluări
- Burns MGNT and CalculationDocument7 paginiBurns MGNT and CalculationPoova RagavanÎncă nu există evaluări
- Angiography: Presented By: Mulituba, Nairah DDocument9 paginiAngiography: Presented By: Mulituba, Nairah DAkazukin AineÎncă nu există evaluări
- Cardiovascular System Diseases Part 1Document22 paginiCardiovascular System Diseases Part 1Prince Rener Velasco PeraÎncă nu există evaluări
- Heart FailureDocument43 paginiHeart FailuresimonjosanÎncă nu există evaluări
- Burns DressingDocument4 paginiBurns DressingBalaMuruganÎncă nu există evaluări
- Peripheral Artery Disease: Nikhil Vaishnav M.Sc. (Nursing)Document70 paginiPeripheral Artery Disease: Nikhil Vaishnav M.Sc. (Nursing)Dimpal ChoudharyÎncă nu există evaluări
- Pericarditis NCLEX Review: Serous Fluid Is Between The Parietal and Visceral LayerDocument2 paginiPericarditis NCLEX Review: Serous Fluid Is Between The Parietal and Visceral LayerlhenÎncă nu există evaluări
- Lung AbscessDocument46 paginiLung AbscessJeevitha VanithaÎncă nu există evaluări
- Riaz Gul AHN Unit 1Document106 paginiRiaz Gul AHN Unit 1Riaz Gul RindÎncă nu există evaluări
- 1 Pain AssessmentDocument13 pagini1 Pain AssessmentQuijano GpokskieÎncă nu există evaluări
- COPDDocument30 paginiCOPDAmila SirisingheÎncă nu există evaluări
- Approach To Patient With Burn (S) : No Blisters Swollen and Blistered Whitish or Charred (Black)Document6 paginiApproach To Patient With Burn (S) : No Blisters Swollen and Blistered Whitish or Charred (Black)Suthar Keval CÎncă nu există evaluări
- Practicle Exam NSG EducationDocument11 paginiPracticle Exam NSG Educationshobharani durgamÎncă nu există evaluări
- Pancreatitis: Dr. Ahmad Aqel RN, PHD The University of Jordan 2015Document27 paginiPancreatitis: Dr. Ahmad Aqel RN, PHD The University of Jordan 2015Anonymous 5HzElnmÎncă nu există evaluări
- Chronic Kidney DiseaseDocument7 paginiChronic Kidney DiseaseLardel Balbiran LafortezaÎncă nu există evaluări
- Adrenal CrisisDocument6 paginiAdrenal CrisisSteven SetioÎncă nu există evaluări
- ETT IntubationDocument10 paginiETT IntubationPoova RagavanÎncă nu există evaluări
- Psychiatric EmergenciesDocument25 paginiPsychiatric EmergenciesAnnapurna DangetiÎncă nu există evaluări
- KeratitisDocument5 paginiKeratitisBagas AndriyonoÎncă nu există evaluări
- Research Proposal Outline (PHD)Document3 paginiResearch Proposal Outline (PHD)nadia azriÎncă nu există evaluări
- Demonstration On ParacentesisDocument10 paginiDemonstration On ParacentesisDeepika PrajapatiÎncă nu există evaluări
- CardioversionDocument48 paginiCardioversionDeeksha RajputÎncă nu există evaluări
- Case Stydy Angina PectorisDocument46 paginiCase Stydy Angina PectorissharenÎncă nu există evaluări
- Burns PDFDocument4 paginiBurns PDFRifqi UlilÎncă nu există evaluări
- A Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsDe la EverandA Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsÎncă nu există evaluări
- Health Talk PlanDocument10 paginiHealth Talk PlanManisha Shakya80% (5)
- Health Talk PlanDocument10 paginiHealth Talk PlanManisha Shakya80% (5)
- Bedside Teaching On Mechanical Ventilation: Submitted ToDocument8 paginiBedside Teaching On Mechanical Ventilation: Submitted ToManisha Shakya50% (2)
- Understanding Liver BiopsyDocument4 paginiUnderstanding Liver BiopsyManisha ShakyaÎncă nu există evaluări
- Assignment ON Diabetic Diet: Submitted To: Ms. Sarita NadiyaDocument8 paginiAssignment ON Diabetic Diet: Submitted To: Ms. Sarita NadiyaManisha Shakya100% (2)
- Intestinal Obstruction and HerniasDocument53 paginiIntestinal Obstruction and HerniasManisha ShakyaÎncă nu există evaluări
- Pamphlet Liver BiopsyDocument8 paginiPamphlet Liver BiopsyManisha ShakyaÎncă nu există evaluări
- Drug Presentation: Manisha M.Sc. Nursing 1 Year Con IlbsDocument57 paginiDrug Presentation: Manisha M.Sc. Nursing 1 Year Con IlbsManisha ShakyaÎncă nu există evaluări
- Drug PresentationDocument32 paginiDrug PresentationManisha ShakyaÎncă nu există evaluări
- Mnlkaxi QH: Manisha M.Sc. NursingDocument57 paginiMnlkaxi QH: Manisha M.Sc. NursingManisha ShakyaÎncă nu există evaluări
- Rapid Fire RoundDocument2 paginiRapid Fire RoundManisha ShakyaÎncă nu există evaluări
- Mnlkaxi QH: Manisha M.Sc. NursingDocument57 paginiMnlkaxi QH: Manisha M.Sc. NursingManisha ShakyaÎncă nu există evaluări
- AssignmentDocument5 paginiAssignmentManisha ShakyaÎncă nu există evaluări
- Pamphlet Liver BiopsyDocument8 paginiPamphlet Liver BiopsyManisha ShakyaÎncă nu există evaluări
- Dass42 TestDocument2 paginiDass42 TestkimmlisaÎncă nu există evaluări
- Biliary TreeDocument20 paginiBiliary TreeManisha Shakya100% (1)
- Bed Side Teaching Whipple'S Procedure: Submitted To-Sarita Nadiya Madam Submitted By-Ms - ManishaDocument8 paginiBed Side Teaching Whipple'S Procedure: Submitted To-Sarita Nadiya Madam Submitted By-Ms - ManishaManisha ShakyaÎncă nu există evaluări
- Fluid Electrolyte Balances and ImbalanceDocument157 paginiFluid Electrolyte Balances and ImbalanceManisha Shakya0% (1)
- Experiment 2 HORSEPOWER EFFICIENCY GEAR RATIO AND SPEED RATIODocument10 paginiExperiment 2 HORSEPOWER EFFICIENCY GEAR RATIO AND SPEED RATIOJake Polo SantiagoÎncă nu există evaluări
- Vq40de Service ManualDocument257 paginiVq40de Service Manualjaumegus100% (4)
- Reference GuideDocument88 paginiReference GuideAnonymous Qm0zbNk100% (1)
- SPFL Monitoring ToolDocument3 paginiSPFL Monitoring ToolAnalyn EnriquezÎncă nu există evaluări
- Bill of Quantities 16FI0009Document1 paginăBill of Quantities 16FI0009AJothamChristianÎncă nu există evaluări
- Financial Institutions Markets and ServicesDocument2 paginiFinancial Institutions Markets and ServicesPavneet Kaur Bhatia100% (1)
- 02 CT311 Site WorksDocument26 pagini02 CT311 Site Worksshaweeeng 101Încă nu există evaluări
- JEE Mains Paper 1 (12 Apr 2019 Shift 2) EnglishDocument131 paginiJEE Mains Paper 1 (12 Apr 2019 Shift 2) EnglishRudraksha KushwahaÎncă nu există evaluări
- Optical Transport Network SwitchingDocument16 paginiOptical Transport Network SwitchingNdambuki DicksonÎncă nu există evaluări
- Answer: C: Exam Name: Exam Type: Exam Code: Total QuestionsDocument26 paginiAnswer: C: Exam Name: Exam Type: Exam Code: Total QuestionsMohammed S.GoudaÎncă nu există evaluări
- ABBindustrialdrives Modules en RevBDocument2 paginiABBindustrialdrives Modules en RevBMaitry ShahÎncă nu există evaluări
- 2.ed - Eng6 - q1 - Mod3 - Make Connections Between Information Viewed and Personal ExpiriencesDocument32 pagini2.ed - Eng6 - q1 - Mod3 - Make Connections Between Information Viewed and Personal ExpiriencesToni Marie Atienza Besa100% (3)
- Bichelle HarrisonDocument2 paginiBichelle HarrisonShahbaz KhanÎncă nu există evaluări
- Thermal Physics Lecture 1Document53 paginiThermal Physics Lecture 1Swee Boon OngÎncă nu există evaluări
- Final - Anarchy One-Sheet Sell SheetDocument2 paginiFinal - Anarchy One-Sheet Sell SheetMaddanie WijayaÎncă nu există evaluări
- Outlook of PonDocument12 paginiOutlook of Ponty nguyenÎncă nu există evaluări
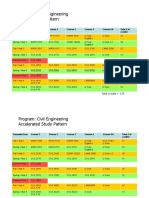
- HKUST 4Y Curriculum Diagram CIVLDocument4 paginiHKUST 4Y Curriculum Diagram CIVLfrevÎncă nu există evaluări
- Advanced Herd Health Management, Sanitation and HygieneDocument28 paginiAdvanced Herd Health Management, Sanitation and Hygienejane entunaÎncă nu există evaluări
- Review of LiteratureDocument3 paginiReview of LiteratureAbhimanyu Narayan RaiÎncă nu există evaluări
- Coke Drum Repair Welch Aquilex WSI DCU Calgary 2009Document37 paginiCoke Drum Repair Welch Aquilex WSI DCU Calgary 2009Oscar DorantesÎncă nu există evaluări
- EP07 Measuring Coefficient of Viscosity of Castor OilDocument2 paginiEP07 Measuring Coefficient of Viscosity of Castor OilKw ChanÎncă nu există evaluări
- Transactions List: Marilena Constantin RO75BRDE445SV93146784450 RON Marilena ConstantinDocument12 paginiTransactions List: Marilena Constantin RO75BRDE445SV93146784450 RON Marilena ConstantinConstantin MarilenaÎncă nu există evaluări
- Ty Baf TaxationDocument4 paginiTy Baf TaxationAkki GalaÎncă nu există evaluări
- Written Report SampleDocument16 paginiWritten Report Sampleallanposo3Încă nu există evaluări
- FluteDocument13 paginiFlutefisher3910% (1)
- Study and Interpretation of The ScoreDocument10 paginiStudy and Interpretation of The ScoreDwightPile-GrayÎncă nu există evaluări
- Work Sample 2 - Eoc and CrucibleDocument35 paginiWork Sample 2 - Eoc and Crucibleapi-259791703Încă nu există evaluări
- Economics Exam Technique GuideDocument21 paginiEconomics Exam Technique Guidemalcewan100% (5)
- FINAL VERSION On Assessment Tool For CDCs LCs Sept. 23 2015Document45 paginiFINAL VERSION On Assessment Tool For CDCs LCs Sept. 23 2015Edmar Cielo SarmientoÎncă nu există evaluări
- JIMMA Electrical&ComputerEngDocument219 paginiJIMMA Electrical&ComputerEngTewodros71% (7)