S-ar putea să vă placă și
- Metabolic Syndrome Risk Factors and ComplicationsDocument46 paginiMetabolic Syndrome Risk Factors and ComplicationsAjeng RetnoÎncă nu există evaluări
- Dyslipidaemias 2019Document30 paginiDyslipidaemias 2019Adinda DianÎncă nu există evaluări
- Ann Soehee - Tctap2021 - SPCDocument43 paginiAnn Soehee - Tctap2021 - SPCSaad KhanÎncă nu există evaluări
- Undangan Rapat PJ UnitDocument1 paginăUndangan Rapat PJ UnitDwi HartatiÎncă nu există evaluări
- Roseday EZ Webinar SlidesDocument35 paginiRoseday EZ Webinar SlidesPragnesh ShahÎncă nu există evaluări
- Lower Is Better - FinalDocument91 paginiLower Is Better - FinalJamsidul Hassan RajibÎncă nu există evaluări
- Statins and Beyond Concurrent Strategies For Prevention of Cardiovascular Disease in Patients WiDocument17 paginiStatins and Beyond Concurrent Strategies For Prevention of Cardiovascular Disease in Patients WiMamad TrihatmowidjoyoÎncă nu există evaluări
- Lower is Better: No Evidence for Treating to Specific lipid TargetsDocument91 paginiLower is Better: No Evidence for Treating to Specific lipid TargetsJamsidul Hassan RajibÎncă nu există evaluări
- Pemberian Insulin KMBDocument36 paginiPemberian Insulin KMBerdhian jatiÎncă nu există evaluări
- Dyslipidemia & Residual RiskDocument26 paginiDyslipidemia & Residual RiskDan LeeÎncă nu există evaluări
- Unmeet Need Is LDL-C Lowering When Regular Statin Wont DoDocument40 paginiUnmeet Need Is LDL-C Lowering When Regular Statin Wont Doyan salvianto100% (1)
- Diabetes Management With Basal InsulinDocument35 paginiDiabetes Management With Basal InsulinSultan MubashirÎncă nu există evaluări
- Lower Is Better - No Evidence For Treating To Spepecific Lipid Targets & Use of StatinsDocument59 paginiLower Is Better - No Evidence For Treating To Spepecific Lipid Targets & Use of StatinsJamsidul Hassan RajibÎncă nu există evaluări
- 2018 RTD Slide - The Place of Newer Generation SUDocument30 pagini2018 RTD Slide - The Place of Newer Generation SUAlka AlkaÎncă nu există evaluări
- Understanding The Needs of The High Productive DyslipidemiaDocument47 paginiUnderstanding The Needs of The High Productive DyslipidemiachchchchkÎncă nu există evaluări
- Dyslipidemia Management in Diabetic PatientsDocument31 paginiDyslipidemia Management in Diabetic PatientsaprinaaaÎncă nu există evaluări
- 10-Year Risk of Fatal CVD Is Based On Risk Factors: Age, Smoking, Sex, Systolic Blood Pressure and Total CholesterolDocument3 pagini10-Year Risk of Fatal CVD Is Based On Risk Factors: Age, Smoking, Sex, Systolic Blood Pressure and Total CholesterolDidik SiswandoroÎncă nu există evaluări
- Recommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (AdaptedDocument8 paginiRecommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (Adaptedعزالدين الطيارÎncă nu există evaluări
- New Recommendations and Revised Concepts in Recent Guidelines On The Management of Dyslipidemias To Prevent Cardiovascular Disease-The 2018 ACC-AHA and 2019 ESC-EAS GuidelinesDocument6 paginiNew Recommendations and Revised Concepts in Recent Guidelines On The Management of Dyslipidemias To Prevent Cardiovascular Disease-The 2018 ACC-AHA and 2019 ESC-EAS GuidelinesJustinaÎncă nu există evaluări
- Dyslipdiemia 2022Document75 paginiDyslipdiemia 2022LeeÎncă nu există evaluări
- Diabetic Complications and Foot CareDocument54 paginiDiabetic Complications and Foot CareNaela AmranÎncă nu există evaluări
- Early Detection Kuliah DokterDocument61 paginiEarly Detection Kuliah Doktersuho exoÎncă nu există evaluări
- Pratley New Treatments For Type 2 DiabetesDocument85 paginiPratley New Treatments For Type 2 DiabetesMia DangaÎncă nu există evaluări
- Ontarget Results April 2008 FinalDocument20 paginiOntarget Results April 2008 Finalyona selvia ariesÎncă nu există evaluări
- 2017 DCP 1. Telmisartan Untuk KasusDocument26 pagini2017 DCP 1. Telmisartan Untuk KasusOcto IndradjajaÎncă nu există evaluări
- Cholesterol Guidelines Review 2020Document6 paginiCholesterol Guidelines Review 2020oriannaocantoÎncă nu există evaluări
- Austin AndrologyDocument4 paginiAustin AndrologyAustin Publishing GroupÎncă nu există evaluări
- Intensity of Cholesterol Lowering With Statin in PatientsDocument23 paginiIntensity of Cholesterol Lowering With Statin in Patientsandri ansyahÎncă nu există evaluări
- Guidelines DyslipidDocument49 paginiGuidelines Dyslipidnoveldycb89Încă nu există evaluări
- Causes & Prevention of Coronary Artery DiseaseDocument41 paginiCauses & Prevention of Coronary Artery DiseaseeenagpurcongÎncă nu există evaluări
- Kuliah Dislipidemia Dan ObesitasDocument50 paginiKuliah Dislipidemia Dan ObesitasiikÎncă nu există evaluări
- Diabetes Mellitus: Geriatrics Evaluation & ManagementDocument4 paginiDiabetes Mellitus: Geriatrics Evaluation & ManagementAngeles SlzrÎncă nu există evaluări
- Management of T2DMDocument54 paginiManagement of T2DMdesyÎncă nu există evaluări
- CVD in Diabetes - EADSG 2016Document57 paginiCVD in Diabetes - EADSG 2016OmarÎncă nu există evaluări
- Evolution of Lipid Management GuidelinesDocument63 paginiEvolution of Lipid Management GuidelinesM Azmi HÎncă nu există evaluări
- Rosuvastatin: Role in Cardiovascular High-Risk PatientDocument11 paginiRosuvastatin: Role in Cardiovascular High-Risk Patientnasir uddinÎncă nu există evaluări
- Hypertension & Diabetis MellitusDocument51 paginiHypertension & Diabetis MellitusSuma_Ramesan_5373100% (1)
- Ongoing Therapy and MonitoringDocument1 paginăOngoing Therapy and MonitoringDaveMartoneÎncă nu există evaluări
- Clinical Management of Stable Coronary Artery Disease in Type 2 Diabetes MellitusDocument5 paginiClinical Management of Stable Coronary Artery Disease in Type 2 Diabetes MellitusAnonymous ZUaUz1wwÎncă nu există evaluări
- Insulin Dr. BowoDocument39 paginiInsulin Dr. BowoAri AsriniÎncă nu există evaluări
- Treatment Based On: Pathophysiology of HyperglycemiaDocument38 paginiTreatment Based On: Pathophysiology of HyperglycemiaRoby KieranÎncă nu există evaluări
- Hipertensi Dan Krisis HipertensiDocument26 paginiHipertensi Dan Krisis Hipertensiseptian_tjayaÎncă nu există evaluări
- Current Concepts of Chronic Diabetic Complications: Sarwono WaspadjiDocument49 paginiCurrent Concepts of Chronic Diabetic Complications: Sarwono WaspadjiscribdÎncă nu există evaluări
- Diabetic Foot Care: ReviewDocument7 paginiDiabetic Foot Care: ReviewRavi HardjumadyÎncă nu există evaluări
- Cardiovascular Disorders: Annette HaynesDocument69 paginiCardiovascular Disorders: Annette HaynesBinh Yen Quach TranÎncă nu există evaluări
- Managing Hidden Cardiovascular Risk in Diabetes Mellitus: Agus YuwonoDocument45 paginiManaging Hidden Cardiovascular Risk in Diabetes Mellitus: Agus YuwonoaprinaaaÎncă nu există evaluări
- Management of Blood Cholesterol 2019Document2 paginiManagement of Blood Cholesterol 2019Luis Alberto Alvarez AnkassÎncă nu există evaluări
- 2019 ESC Guidelines On Diabetes, Pre-Diabetes, and Cardiovascular DiseasesDocument19 pagini2019 ESC Guidelines On Diabetes, Pre-Diabetes, and Cardiovascular DiseasesBertha MansurÎncă nu există evaluări
- A Review of Efficacy RosuvastatinDocument11 paginiA Review of Efficacy RosuvastatindunhowhÎncă nu există evaluări
- Acute Metabolic Emergencies in Diabetes: DKA, HHS and EDKADocument30 paginiAcute Metabolic Emergencies in Diabetes: DKA, HHS and EDKAGian CarloÎncă nu există evaluări
- Final Atcofliflozin Binder DiabetesDocument23 paginiFinal Atcofliflozin Binder DiabetesEslamÎncă nu există evaluări
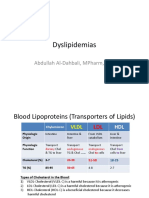
- Dyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDDocument15 paginiDyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDعزالدين الطيارÎncă nu există evaluări
- 2013 Cholesterol Guidelines at A Glance: - Robert Barnes, M3Document15 pagini2013 Cholesterol Guidelines at A Glance: - Robert Barnes, M3CoolrobertizÎncă nu există evaluări
- Chapter 8 Dyslipidemia: Understanding Cholesterol Levels and RisksDocument10 paginiChapter 8 Dyslipidemia: Understanding Cholesterol Levels and RisksFriska tampuboLonÎncă nu există evaluări
- Non-Communicable Diseases - Lifestyle Related Diseases: Wilma N. Beralde, RM, RN, ManDocument53 paginiNon-Communicable Diseases - Lifestyle Related Diseases: Wilma N. Beralde, RM, RN, ManNaddy RetxedÎncă nu există evaluări
- Chronic Complications of Diabetes MellitusDocument40 paginiChronic Complications of Diabetes MellitusironÎncă nu există evaluări
- Primary and Secondary CV Prevention - Iman EvanDocument104 paginiPrimary and Secondary CV Prevention - Iman EvanFikriYTÎncă nu există evaluări
- Kelompok 1Document14 paginiKelompok 1Aurent WidjanarkoÎncă nu există evaluări
- Metformin, Diabetes, Update of The Evidence BaseDocument14 paginiMetformin, Diabetes, Update of The Evidence BaseRonal PerinoÎncă nu există evaluări
- The Efects of a Plant-Based Diet on Diabetes MellitusDe la EverandThe Efects of a Plant-Based Diet on Diabetes MellitusÎncă nu există evaluări
- Draft JADWAL KULIAH - 2022-2023 - Edited 8agustus2022-1Document101 paginiDraft JADWAL KULIAH - 2022-2023 - Edited 8agustus2022-1indro hariantoÎncă nu există evaluări
- MonkeypoxDocument36 paginiMonkeypoxindro hariantoÎncă nu există evaluări
- MonkeypoxDocument36 paginiMonkeypoxindro hariantoÎncă nu există evaluări
- Glycemic IndexDocument1 paginăGlycemic Indexindro hariantoÎncă nu există evaluări
- Problem Solving in LogyDocument293 paginiProblem Solving in Logyveravero100% (2)
- Diare Ubaya 2Document38 paginiDiare Ubaya 2indro hariantoÎncă nu există evaluări
- Lampiran 1. Data PenelitianDocument6 paginiLampiran 1. Data Penelitianindro hariantoÎncă nu există evaluări
- Glycemic IndexDocument1 paginăGlycemic Indexindro hariantoÎncă nu există evaluări
- Nilai GulaDocument1 paginăNilai Gulaindro hariantoÎncă nu există evaluări
- Fournier's Gangrene Clinical Review Outlines Risk Factors and ManagementDocument10 paginiFournier's Gangrene Clinical Review Outlines Risk Factors and Managementindro hariantoÎncă nu există evaluări
- Glycemic IndexDocument1 paginăGlycemic Indexindro hariantoÎncă nu există evaluări
- CRIM 3 Midterm Exam Answer KeyDocument2 paginiCRIM 3 Midterm Exam Answer KeyKenneth AlatanÎncă nu există evaluări
- GBS Vagus NerveDocument15 paginiGBS Vagus Nerveprintulmiorlau100% (3)
- Mounjaro UspiDocument19 paginiMounjaro UspiayaznptiÎncă nu există evaluări
- Ac EPTDocument29 paginiAc EPTNisa Nisa100% (2)
- TB Chapter17Document19 paginiTB Chapter17Avery Wiese100% (2)
- Lou Gehrigs Disease PresentationDocument15 paginiLou Gehrigs Disease PresentationAdi ParamarthaÎncă nu există evaluări
- Nutrition AssessmentDocument22 paginiNutrition AssessmentMelissakklÎncă nu există evaluări
- Biological Aspect of Aging: Eligrace F. Fabian, RNDocument39 paginiBiological Aspect of Aging: Eligrace F. Fabian, RNsweetsai05Încă nu există evaluări
- Sepsis and Septic ShockDocument36 paginiSepsis and Septic ShockCarlos Emerson Rodriguez MalaverÎncă nu există evaluări
- Handout PolioDocument24 paginiHandout Poliobryan leguiabÎncă nu există evaluări
- @anesthesia Books 2019 CRQs in Anaesthesia Constructed Response PDFDocument552 pagini@anesthesia Books 2019 CRQs in Anaesthesia Constructed Response PDFAbed AlawnehÎncă nu există evaluări
- 12Document31 pagini12chieflittlehorseÎncă nu există evaluări
- SclerademaDocument5 paginiSclerademaMichael SponslerÎncă nu există evaluări
- Usmle Hy Images: By: MeduploaderDocument62 paginiUsmle Hy Images: By: Meduploaderdamodarpatil100% (18)
- Numbness: Tyas Mayangputri Hadiana - 10100118204Document7 paginiNumbness: Tyas Mayangputri Hadiana - 10100118204refimaya arlitaÎncă nu există evaluări
- Physical Examination TemplateDocument6 paginiPhysical Examination TemplateJeremy Owen G. GoÎncă nu există evaluări
- Clinical Psychology Summary 1 SearchDocument33 paginiClinical Psychology Summary 1 SearchDaniel IliescuÎncă nu există evaluări
- Cleric Spell List D&D 5th EditionDocument9 paginiCleric Spell List D&D 5th EditionLeandros Mavrokefalos100% (2)
- RickettsiaDocument3 paginiRickettsiaFeroz MamunÎncă nu există evaluări
- Berlant - Slow Death (Sovereignty, Obesity, Lateral Agency)Document28 paginiBerlant - Slow Death (Sovereignty, Obesity, Lateral Agency)Anna FlynnÎncă nu există evaluări
- PN Comprehensive Practice A Anad B Questions and Answers VerifiedDocument8 paginiPN Comprehensive Practice A Anad B Questions and Answers Verifiedianshirow834Încă nu există evaluări
- Nursing Health Assessment Exam 2Document45 paginiNursing Health Assessment Exam 2Jennifer Jaworsky100% (3)
- (3F) Pediatrics - Pediatric HistoryDocument9 pagini(3F) Pediatrics - Pediatric HistoryNomar Nonato100% (2)
- June 2009Document37 paginiJune 2009Onichan KhunÎncă nu există evaluări
- Bad Trip Due To Anticholinergic Effect of CannabisDocument2 paginiBad Trip Due To Anticholinergic Effect of CannabisRobert DinuÎncă nu există evaluări
- The Adrenal Thyroid Revolution Supplement Guide: SOS RX: Daily Dose SupplementsDocument8 paginiThe Adrenal Thyroid Revolution Supplement Guide: SOS RX: Daily Dose SupplementsPetra JobovaÎncă nu există evaluări
- EweDocument246 paginiEweOluwo88% (32)
- Community Health Nursing (Learning Feedback Diary (LFD #25)Document3 paginiCommunity Health Nursing (Learning Feedback Diary (LFD #25)Angelica Malacay RevilÎncă nu există evaluări
- Doctor Charting Guidelines for HPI, Exams and ManagementDocument2 paginiDoctor Charting Guidelines for HPI, Exams and ManagementMacy Valenciano MacatuggalÎncă nu există evaluări
- Medical and Allied Health ProfessionDocument30 paginiMedical and Allied Health ProfessionAnalyn QueroÎncă nu există evaluări