S-ar putea să vă placă și
- Practical Gastroenterology and Hepatology Board Review ToolkitDe la EverandPractical Gastroenterology and Hepatology Board Review ToolkitKenneth R. DeVaultÎncă nu există evaluări
- The Parkinson's Effect: R&R (Recommendations and Reasons)De la EverandThe Parkinson's Effect: R&R (Recommendations and Reasons)Încă nu există evaluări
- Urinary Incontinence: By: Ayu SorayaDocument23 paginiUrinary Incontinence: By: Ayu Sorayaandry setiawanÎncă nu există evaluări
- Acute Kidney Injury: KDIGO 2012 Clinical Practice GuidelineDocument40 paginiAcute Kidney Injury: KDIGO 2012 Clinical Practice GuidelineAbedDabajaÎncă nu există evaluări
- Urinary IncontinenceDocument34 paginiUrinary IncontinenceHerb Ezaldein100% (2)
- The Effect of Aromatherapy On Fatigue and Anxiety.62 PDFDocument8 paginiThe Effect of Aromatherapy On Fatigue and Anxiety.62 PDFImelda WidiyatamaÎncă nu există evaluări
- Urinary Retention 2Document3 paginiUrinary Retention 2Agli AdhityaÎncă nu există evaluări
- Urinary IncontinenceDocument112 paginiUrinary IncontinencePrabhakar KumarÎncă nu există evaluări
- HematuriaDocument51 paginiHematuriaRam ManoharÎncă nu există evaluări
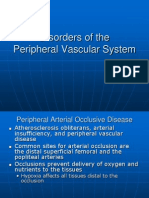
- Disorders of The Peripheral Vascular SystemDocument17 paginiDisorders of The Peripheral Vascular SystemDardarConstantinoÎncă nu există evaluări
- JNC 8Document40 paginiJNC 8Nadira Wulandari100% (1)
- Urologic Emergencies: Hakan Koyuncu MD Associate Professor Yeditepe University Medical Faculty Department of UrologyDocument62 paginiUrologic Emergencies: Hakan Koyuncu MD Associate Professor Yeditepe University Medical Faculty Department of UrologycoassrunÎncă nu există evaluări
- Obstructive Uropathy & Urinary Tract CalculiDocument55 paginiObstructive Uropathy & Urinary Tract CalculiNorFarah Fatin AnuarÎncă nu există evaluări
- Ks Module 12Document29 paginiKs Module 12jerinthomasrajanÎncă nu există evaluări
- Final GIT Case PresentationDocument53 paginiFinal GIT Case PresentationRovan100% (1)
- Frailty in The Elderly - Compressed PDFDocument74 paginiFrailty in The Elderly - Compressed PDFNaing LlynÎncă nu există evaluări
- Nephrology: Omar K MRCP IrelandDocument54 paginiNephrology: Omar K MRCP IrelandManmeet SÎncă nu există evaluări
- Acid Peptic DisordersDocument67 paginiAcid Peptic DisordersTheop AyodeleÎncă nu există evaluări
- Subacute Combined Degeneration of Spinal CordDocument4 paginiSubacute Combined Degeneration of Spinal CordPriyanka MathurÎncă nu există evaluări
- Treatment of CP With Chinese Scalp Acupuncture 17 June HaoDocument6 paginiTreatment of CP With Chinese Scalp Acupuncture 17 June HaoSebastiano Serra100% (1)
- DR Aida Lombok 3 Mei 2017 - HisfarsiDocument39 paginiDR Aida Lombok 3 Mei 2017 - HisfarsiBasri BaslamÎncă nu există evaluări
- Acute Glomerulonep Hritis: By: Edelrose D. Lapitan BSN Iii-CDocument29 paginiAcute Glomerulonep Hritis: By: Edelrose D. Lapitan BSN Iii-CEdelrose Lapitan100% (1)
- UGIHDocument59 paginiUGIHEkkawit IamthonginÎncă nu există evaluări
- Urinary Tract DisorderDocument63 paginiUrinary Tract DisorderShivaranjan KsÎncă nu există evaluări
- Organophosphorus Poisoning PDFDocument5 paginiOrganophosphorus Poisoning PDFEliuth Zamora100% (1)
- Physio Reviewer Renal To Acid BaseDocument11 paginiPhysio Reviewer Renal To Acid BaseNicole ChanÎncă nu există evaluări
- Nephrology - Proteinuria - SOAP Note - Manish Suneja PDFDocument4 paginiNephrology - Proteinuria - SOAP Note - Manish Suneja PDFΝίκος ΣυρίγοςÎncă nu există evaluări
- Hyporeninemic HypoaldosteronismDocument12 paginiHyporeninemic HypoaldosteronismCésar Augusto Sánchez SolisÎncă nu există evaluări
- UROLITHIASISDocument25 paginiUROLITHIASISPaulo ManlangitÎncă nu există evaluări
- Acute Kidney Injury (AKI)Document68 paginiAcute Kidney Injury (AKI)Alex beharuÎncă nu există evaluări
- Icu-Ccu Inservice Training For Nurses (Recertification)Document41 paginiIcu-Ccu Inservice Training For Nurses (Recertification)anagh cuphuÎncă nu există evaluări
- Urological Emergencies: DR Ahmed BekeerDocument31 paginiUrological Emergencies: DR Ahmed BekeerAh BakaÎncă nu există evaluări
- Renal Ultrasound: Diana Pancu, MDDocument76 paginiRenal Ultrasound: Diana Pancu, MDYoungFanjiens100% (1)
- Principle of Fluid & Electrolyte Management in ADocument47 paginiPrinciple of Fluid & Electrolyte Management in AAbdulazeez Abdulmalik100% (1)
- Lower Urinary Tract Symptoms (LUTS)Document26 paginiLower Urinary Tract Symptoms (LUTS)Ayi Abdul BasithÎncă nu există evaluări
- 8.the Meanings of MenopauseDocument275 pagini8.the Meanings of MenopauseMuhammad Syamil RozlanÎncă nu există evaluări
- AtaxiaDocument10 paginiAtaxiaosakaÎncă nu există evaluări
- Lung Transplant PathwayDocument39 paginiLung Transplant PathwayMohana Preethi MÎncă nu există evaluări
- Peptic Ulcer DiseaseDocument18 paginiPeptic Ulcer DiseasechetankumarbhumireddyÎncă nu există evaluări
- Neurogenic Bladder: When Nerve Damage Causes Bladder ProblemsDocument3 paginiNeurogenic Bladder: When Nerve Damage Causes Bladder ProblemsmarselamgeÎncă nu există evaluări
- Hyponatremia in Children 03.19.2010Document23 paginiHyponatremia in Children 03.19.2010Emily EresumaÎncă nu există evaluări
- Nonalcoholic Fatty Liver Disease (NAFLD) : Where Are We Today?Document32 paginiNonalcoholic Fatty Liver Disease (NAFLD) : Where Are We Today?Saad MotawéaÎncă nu există evaluări
- Treatment of Pulmonary Embolism Anticoagulation Thrombolytic Therapy and Complications of Therapy 2011 Critical Care ClinicsDocument15 paginiTreatment of Pulmonary Embolism Anticoagulation Thrombolytic Therapy and Complications of Therapy 2011 Critical Care ClinicsGabriel Alberto Tamayo SolÎncă nu există evaluări
- DM PhysioDocument24 paginiDM Physiodwi astutiÎncă nu există evaluări
- Kidney Stones Pathophysiology, Diagnosis and ManagementDocument13 paginiKidney Stones Pathophysiology, Diagnosis and ManagementNani AlituÎncă nu există evaluări
- Acute Tubular NecrosisDocument33 paginiAcute Tubular Necrosisanita meihuaÎncă nu există evaluări
- Irritable Bowel Syndrome (IBS)Document7 paginiIrritable Bowel Syndrome (IBS)Hisyam DinGanuÎncă nu există evaluări
- 990812 EUS教學 (4) 重點式急診泌尿系統超音波之應用Document77 pagini990812 EUS教學 (4) 重點式急診泌尿系統超音波之應用juice119100% (2)
- Introduction To Intervertebral Disc Anatomy, Pivd (Lumbar) and Its ManagementDocument104 paginiIntroduction To Intervertebral Disc Anatomy, Pivd (Lumbar) and Its ManagementVivek SaxenaÎncă nu există evaluări
- Acute Urinary RetentionDocument26 paginiAcute Urinary Retentionlukmankyubi100% (1)
- Renal Transplant: 1) Steps Involved in Kidney TransplantationDocument4 paginiRenal Transplant: 1) Steps Involved in Kidney TransplantationNadia SalwaniÎncă nu există evaluări
- Acute Kidney InjuryDocument21 paginiAcute Kidney InjuryAtif Gazali100% (1)
- Management of IncontinenceDocument91 paginiManagement of IncontinenceVahid Msmi100% (1)
- Compilation Conditions + FormulasDocument2 paginiCompilation Conditions + Formulaspeter911x0% (1)
- Acute Renal FailureDocument6 paginiAcute Renal Failurearif kurnia timurÎncă nu există evaluări
- Cvs PracticalDocument63 paginiCvs PracticalSreedeep TejaÎncă nu există evaluări
- Rheumatic Heart Disease: Emmanuel Edafe Consultant Interventional Cardiologist, NduDocument36 paginiRheumatic Heart Disease: Emmanuel Edafe Consultant Interventional Cardiologist, NduPrincewill SeiyefaÎncă nu există evaluări
- Cushing DiseaseDocument24 paginiCushing DiseaseSuci AlimaÎncă nu există evaluări
- Fluids Electrolytes and Acid Base ImbalancesDocument8 paginiFluids Electrolytes and Acid Base ImbalancesSamantha Bernardo UndaÎncă nu există evaluări
- Gastrointestinal Diseases and Disorders Sourcebook, Fifth EditionDe la EverandGastrointestinal Diseases and Disorders Sourcebook, Fifth EditionÎncă nu există evaluări
- Frequency Response For Control System Analysis - GATE Study Material in PDFDocument7 paginiFrequency Response For Control System Analysis - GATE Study Material in PDFNarendra AgrawalÎncă nu există evaluări
- Elastomeric Impression MaterialsDocument6 paginiElastomeric Impression MaterialsMarlene CasayuranÎncă nu există evaluări
- Mitsubishi FanDocument2 paginiMitsubishi FanKyaw ZawÎncă nu există evaluări
- 0 BA Design ENDocument12 pagini0 BA Design ENFilho AiltonÎncă nu există evaluări
- IPM GuidelinesDocument6 paginiIPM GuidelinesHittesh SolankiÎncă nu există evaluări
- DIFFERENTIATING PERFORMANCE TASK FOR DIVERSE LEARNERS (Script)Document2 paginiDIFFERENTIATING PERFORMANCE TASK FOR DIVERSE LEARNERS (Script)Laurice Carmel AgsoyÎncă nu există evaluări
- Grade 9 WorkbookDocument44 paginiGrade 9 WorkbookMaria Russeneth Joy NaloÎncă nu există evaluări
- Object-Oriented Design Patterns in The Kernel, Part 2 (LWN - Net)Document15 paginiObject-Oriented Design Patterns in The Kernel, Part 2 (LWN - Net)Rishabh MalikÎncă nu există evaluări
- Tree PruningDocument15 paginiTree Pruningrita44Încă nu există evaluări
- War at Sea Clarifications Aug 10Document4 paginiWar at Sea Clarifications Aug 10jdageeÎncă nu există evaluări
- TrellisDocument1 paginăTrellisCayenne LightenÎncă nu există evaluări
- Aquaculture - Set BDocument13 paginiAquaculture - Set BJenny VillamorÎncă nu există evaluări
- T-Tess Six Educator StandardsDocument1 paginăT-Tess Six Educator Standardsapi-351054075100% (1)
- LRAD Datasheet 2000XDocument2 paginiLRAD Datasheet 2000XOkkar MaungÎncă nu există evaluări
- IG Deck Seal PumpDocument3 paginiIG Deck Seal PumpSergei KurpishÎncă nu există evaluări
- 2a Unani Medicine in India - An OverviewDocument123 pagini2a Unani Medicine in India - An OverviewGautam NatrajanÎncă nu există evaluări
- Electric Motor Cycle and ScooterDocument9 paginiElectric Motor Cycle and ScooterA A.DevanandhÎncă nu există evaluări
- BRAND AWARENESS Proposal DocumentDocument11 paginiBRAND AWARENESS Proposal DocumentBuchi MadukaÎncă nu există evaluări
- Chapter Three: Tools For Exploring The World: Physical, Perceptual, and Motor DevelopmentDocument43 paginiChapter Three: Tools For Exploring The World: Physical, Perceptual, and Motor DevelopmentHsieh Yun JuÎncă nu există evaluări
- Advent Wreath Lesson PlanDocument2 paginiAdvent Wreath Lesson Planapi-359764398100% (1)
- Student Exploration: Digestive System: Food Inio Simple Nutrien/oDocument9 paginiStudent Exploration: Digestive System: Food Inio Simple Nutrien/oAshantiÎncă nu există evaluări
- Morse Potential CurveDocument9 paginiMorse Potential Curvejagabandhu_patraÎncă nu există evaluări
- Final Prmy Gr4 Math Ph1 HWSHDocument55 paginiFinal Prmy Gr4 Math Ph1 HWSHKarthik KumarÎncă nu există evaluări
- Laboratorio 1Document6 paginiLaboratorio 1Marlon DiazÎncă nu există evaluări
- FSM Syllabus20071228 1Document3 paginiFSM Syllabus20071228 1Institute of Fengshui BaziÎncă nu există evaluări
- #Angles Are in Degrees: EGR2313 HW SOLUTIONS (2021)Document4 pagini#Angles Are in Degrees: EGR2313 HW SOLUTIONS (2021)SolomonÎncă nu există evaluări
- Course Projects PDFDocument1 paginăCourse Projects PDFsanjog kshetriÎncă nu există evaluări
- Unit 1 and 2Document4 paginiUnit 1 and 2Aim Rubia100% (1)
- Hydrogeological Survey and Eia Tor - Karuri BoreholeDocument3 paginiHydrogeological Survey and Eia Tor - Karuri BoreholeMutonga Kitheko100% (1)
- A Junk Project - An Income Generating ProjectDocument2 paginiA Junk Project - An Income Generating ProjectHercules Verdeflor ValenzuelaÎncă nu există evaluări