S-ar putea să vă placă și
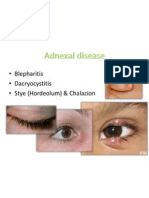
- Tumor Mata: Dr. H. Ibrahim, SPM (K)Document37 paginiTumor Mata: Dr. H. Ibrahim, SPM (K)vivilmÎncă nu există evaluări
- Dr. Mubashir Rehman: Assistant ProfessorDocument112 paginiDr. Mubashir Rehman: Assistant Professorsaqibullah gulÎncă nu există evaluări
- Eyelid PathologyDocument55 paginiEyelid PathologyleahÎncă nu există evaluări
- Diseases of The Eyelids: Mshangila Barnabas MD, M.MedDocument31 paginiDiseases of The Eyelids: Mshangila Barnabas MD, M.MedCharles AnthonyÎncă nu există evaluări
- Eyelid Orbit and ConjunctivaDocument123 paginiEyelid Orbit and ConjunctivaRgdÎncă nu există evaluări
- Eyelids Diseases Lacrimal System DiseasesDocument45 paginiEyelids Diseases Lacrimal System DiseasesMAMA LALAÎncă nu există evaluări
- ChalazionDocument6 paginiChalazionReyhan HarahapÎncă nu există evaluări
- Common Ophthalmic DisordersDocument29 paginiCommon Ophthalmic DisordersSamirÎncă nu există evaluări
- Kelainan Kelopak (Hordeolum, Chalazion, Trichiasis, Blefaritis)Document19 paginiKelainan Kelopak (Hordeolum, Chalazion, Trichiasis, Blefaritis)Wulan NeenÎncă nu există evaluări
- Penyakit Pada MataDocument138 paginiPenyakit Pada Matadevi taqiyyahÎncă nu există evaluări
- Diseases of Eyelid: Prepared by DR - Sourab Kumar DasDocument66 paginiDiseases of Eyelid: Prepared by DR - Sourab Kumar Dasসপ্নে ছোয়া মনÎncă nu există evaluări
- Gangguan Kelopak MataDocument88 paginiGangguan Kelopak MataraiÎncă nu există evaluări
- Revision Mcqs MCQS: Professor Osama ShalabyDocument161 paginiRevision Mcqs MCQS: Professor Osama ShalabyAhmed YounisÎncă nu există evaluări
- Eyelids Eyelids: 7 Semester Dr. Monika Mahat 3 Year Resident Ophthalmology Department LMCTHDocument64 paginiEyelids Eyelids: 7 Semester Dr. Monika Mahat 3 Year Resident Ophthalmology Department LMCTHSubash BasnetÎncă nu există evaluări
- Eye Diagnostic Points - McqsDocument21 paginiEye Diagnostic Points - McqsMuhammad AwaisÎncă nu există evaluări
- EntropionDocument24 paginiEntropionananyaag721Încă nu există evaluări
- Eye Disorders in Children: Alka Sara SajuDocument64 paginiEye Disorders in Children: Alka Sara SajuManisa ParidaÎncă nu există evaluări
- Eyelids AdnexalDocument52 paginiEyelids AdnexalRushdaÎncă nu există evaluări
- Opthalmic Emergencies PresentationDocument85 paginiOpthalmic Emergencies PresentationvictoreffiomÎncă nu există evaluări
- Eye Path12Document45 paginiEye Path12JillKellyÎncă nu există evaluări
- EyelidsDocument96 paginiEyelidsArwa QishtaÎncă nu există evaluări
- Adnexal Diseases, Corneal Abrasion, FBDocument13 paginiAdnexal Diseases, Corneal Abrasion, FBPatt PopÎncă nu există evaluări
- Blepharitis: Dr.T. Kurinchi, MsDocument39 paginiBlepharitis: Dr.T. Kurinchi, MsNailul RosyidaÎncă nu există evaluări
- Mahmood J ShowailDocument47 paginiMahmood J ShowailFauzanFazaAzizÎncă nu există evaluări
- BlepharitisDocument11 paginiBlepharitismohamadÎncă nu există evaluări
- Blepharitis PresentationDocument9 paginiBlepharitis PresentationIt DevelopersÎncă nu există evaluări
- Disease of Lids and Lacrim Al Apparatus: The First Affiliated Hospital of Zhengzhou UniversityDocument46 paginiDisease of Lids and Lacrim Al Apparatus: The First Affiliated Hospital of Zhengzhou Universityapi-19916399Încă nu există evaluări
- 2 EyelidsDocument18 pagini2 Eyelidscawsey mohamedÎncă nu există evaluări
- BlepharitisDocument11 paginiBlepharitismohamadÎncă nu există evaluări
- DT LeukocoriaDocument43 paginiDT LeukocoriadeyshieÎncă nu există evaluări
- Kuliah Mata Merah, Kelainan Struktur Dan Bentuk Mata - DR NaziyaDocument47 paginiKuliah Mata Merah, Kelainan Struktur Dan Bentuk Mata - DR NaziyaFastiati RAÎncă nu există evaluări
- Conjunctiva Anatomy and PhysiologyDocument106 paginiConjunctiva Anatomy and Physiologysaddam0% (1)
- Opthalmology PhotosDocument54 paginiOpthalmology Photosshekharkhadka2057Încă nu există evaluări
- 8 Lacrimal Drainage System Diseases by James PMDocument63 pagini8 Lacrimal Drainage System Diseases by James PMCharles AntonyÎncă nu există evaluări
- Preceptor: Dr. Rahmat Syuhada SP.M (K) : BlefaritisDocument23 paginiPreceptor: Dr. Rahmat Syuhada SP.M (K) : BlefaritisAndre BinsarÎncă nu există evaluări
- Secondary Angle Closure GlaucomaDocument35 paginiSecondary Angle Closure GlaucomaAndriati NadhilaÎncă nu există evaluări
- Glaucoma: Defitaria Permatasari I11109005Document46 paginiGlaucoma: Defitaria Permatasari I11109005yusufharkianÎncă nu există evaluări
- Ophthalmology - Diseases of The EyelidsDocument9 paginiOphthalmology - Diseases of The EyelidsjbtcmdtjjvÎncă nu există evaluări
- Penyakit Palpebra Dan AdneksaDocument39 paginiPenyakit Palpebra Dan AdneksaayucicuÎncă nu există evaluări
- Disease of Orbit, LacrimalDocument73 paginiDisease of Orbit, LacrimalMarshet GeteÎncă nu există evaluări
- Presentation Topic: Corneal DegenerationDocument16 paginiPresentation Topic: Corneal DegenerationArooba MalikÎncă nu există evaluări
- Kuliah Blok Mata: Halida Wibawaty Infection Immunology Subdivision Department of Ophthalmology RSUD DR Moewardi SurakartaDocument51 paginiKuliah Blok Mata: Halida Wibawaty Infection Immunology Subdivision Department of Ophthalmology RSUD DR Moewardi SurakartaMuhammad Nur SidiqÎncă nu există evaluări
- Dry Eye SyndromeDocument69 paginiDry Eye Syndromeendalew mulugetaÎncă nu există evaluări
- Ophthalmology QuizDocument45 paginiOphthalmology QuizLana LocoÎncă nu există evaluări
- Ocular ExaminationDocument55 paginiOcular Examinationsath3028Încă nu există evaluări
- Corneal DiseasesDocument32 paginiCorneal Diseasesnighat khanÎncă nu există evaluări
- Presentation 2Document57 paginiPresentation 2medhanit anjuloÎncă nu există evaluări
- Chp6 Ocular Surface DiseasesDocument31 paginiChp6 Ocular Surface DiseasesarifdikmanÎncă nu există evaluări
- Dakriosistits Akut, Dakriosistits Kronis, DakrioadenitisDocument37 paginiDakriosistits Akut, Dakriosistits Kronis, DakrioadenitisyuliasmindeÎncă nu există evaluări
- Phatology The Eyelids, Lacrimal GlandsDocument62 paginiPhatology The Eyelids, Lacrimal GlandsGermanyÎncă nu există evaluări
- Dry EyeDocument36 paginiDry EyeJ NATASHA MARIAÎncă nu există evaluări
- Ocular Manifestations in TB, Leprosy and SyphilisDocument62 paginiOcular Manifestations in TB, Leprosy and SyphilisAnumeha JindalÎncă nu există evaluări
- Common Diseases in Eye Lid & Its AnatomyDocument41 paginiCommon Diseases in Eye Lid & Its AnatomyTahmidur RahmanÎncă nu există evaluări
- Glaucoma: Seminar OnDocument43 paginiGlaucoma: Seminar OnSanjay GarasiyaÎncă nu există evaluări
- Palpebra Dan Jaringan Orbita FixDocument77 paginiPalpebra Dan Jaringan Orbita FixRiezqi Aditya Putra BakriÎncă nu există evaluări
- Eye Adnexa Diseases: Catedra OftalmologieDocument39 paginiEye Adnexa Diseases: Catedra OftalmologieDanielaÎncă nu există evaluări
- DT LeukocoriaDocument44 paginiDT LeukocoriahamzahÎncă nu există evaluări
- Ophthalmology: Almendrala-Molina, Jorja Post Graduate InternDocument65 paginiOphthalmology: Almendrala-Molina, Jorja Post Graduate InternJajaAlmendralaÎncă nu există evaluări
- Corneal DiseasesDocument55 paginiCorneal DiseasesShally GuptaÎncă nu există evaluări
- Clinical Ophthalmology for UndergraduatesDe la EverandClinical Ophthalmology for UndergraduatesEvaluare: 4 din 5 stele4/5 (5)
- Non Hodgkin's Lymphoma: Rakesh BiswasDocument16 paginiNon Hodgkin's Lymphoma: Rakesh BiswasDayledaniel SorvetoÎncă nu există evaluări
- Systemic Lupus ErythematosusDocument25 paginiSystemic Lupus ErythematosusdaliaÎncă nu există evaluări
- Commentary: Dr. Brian BudgellDocument6 paginiCommentary: Dr. Brian Budgellsolstar1008Încă nu există evaluări
- Book Review of Practical Counselling and Helping Skills - Chapter 16Document3 paginiBook Review of Practical Counselling and Helping Skills - Chapter 16woanling leeÎncă nu există evaluări
- Freud Eros and ThanatosDocument5 paginiFreud Eros and Thanatossicoastrologo_5Încă nu există evaluări
- E Posters PDFDocument349 paginiE Posters PDFpriyadikkalaÎncă nu există evaluări
- Brochure Gelofusine Ef PDFDocument4 paginiBrochure Gelofusine Ef PDFJeshwinder KaurÎncă nu există evaluări
- Primitive ReflexesDocument6 paginiPrimitive ReflexesMarikit2012100% (1)
- Little HansDocument3 paginiLittle HansJC4REAL86Încă nu există evaluări
- SujokDocument57 paginiSujokVitor Fernandes de Souza100% (1)
- Converging Disciplines at The Crossroads of Cancer Care BrochureDocument2 paginiConverging Disciplines at The Crossroads of Cancer Care BrochuremusictherapistsÎncă nu există evaluări
- Tissue Adaptation To Physical Stress: A Proposed "Physical Stress Theory" To Guide Physical Therapist Practice, Education, and ResearchDocument21 paginiTissue Adaptation To Physical Stress: A Proposed "Physical Stress Theory" To Guide Physical Therapist Practice, Education, and ResearchGavin Cao100% (1)
- Broncho, Second YearDocument68 paginiBroncho, Second YearHampson MalekanoÎncă nu există evaluări
- Oral HabitsDocument78 paginiOral HabitsMrunali MaskeÎncă nu există evaluări
- Removable Orthodontic Appliances (ROA) 2Document83 paginiRemovable Orthodontic Appliances (ROA) 2cynjesÎncă nu există evaluări
- Trunk Kinematics in Hemiplegic Gait and Effect of Walking AidsDocument6 paginiTrunk Kinematics in Hemiplegic Gait and Effect of Walking Aidsbarros6Încă nu există evaluări
- Abg Specimen Collection Test RequisitionDocument7 paginiAbg Specimen Collection Test RequisitionVangie OriginesÎncă nu există evaluări
- Presentasi OcdDocument10 paginiPresentasi OcdRizal L MuzakiÎncă nu există evaluări
- How Do You Handle StressDocument15 paginiHow Do You Handle StressLing HockÎncă nu există evaluări
- Anesthesia & Analgesia For Labor & DeliveryDocument30 paginiAnesthesia & Analgesia For Labor & DeliveryPalwasha MalikÎncă nu există evaluări
- Nursing Care Plan (CVA)Document2 paginiNursing Care Plan (CVA)Mel Rodolfo50% (2)
- Are You A Mentor, A Helper or A Rescuer?: SciencedirectDocument9 paginiAre You A Mentor, A Helper or A Rescuer?: SciencedirectSpam PubsÎncă nu există evaluări
- Self-Concealment and Attitudes Toward Counseling in University StudentsDocument7 paginiSelf-Concealment and Attitudes Toward Counseling in University StudentsMaryÎncă nu există evaluări
- Good Radio Pharmacy Practice - OriginalDocument34 paginiGood Radio Pharmacy Practice - OriginalTusvedran PillaiÎncă nu există evaluări
- BC Lioton SKDocument71 paginiBC Lioton SKAlejandra Cale Radowitz0% (1)
- Cobbett 2016Document9 paginiCobbett 2016angieÎncă nu există evaluări
- Hasler 2004 Prochaska Eating DisordersDocument7 paginiHasler 2004 Prochaska Eating Disordersandra_coralia9112Încă nu există evaluări
- Mood Disorders - Lecture NotesDocument24 paginiMood Disorders - Lecture NotesPeter Forster100% (9)
- October Offers Jafra IndiaDocument7 paginiOctober Offers Jafra IndiaNehaÎncă nu există evaluări
- Sri Lakshmi Medical Centre and Hospital: 18/121 MTP Road, Thudiyalur, Coimbatore - 641 034Document49 paginiSri Lakshmi Medical Centre and Hospital: 18/121 MTP Road, Thudiyalur, Coimbatore - 641 034dhir.ankur100% (1)