S-ar putea să vă placă și
- Pharm MnemonicsDocument33 paginiPharm MnemonicsThomson George75% (4)
- Cardiovascular Pharmacology - Antihypertensive AgentsCardiovascular Pharmacology - Antihypertensive AgentsDocument14 paginiCardiovascular Pharmacology - Antihypertensive AgentsCardiovascular Pharmacology - Antihypertensive AgentsAndySatrioTipunkÎncă nu există evaluări
- Emergency Room Drugs Nursing ResponsibilitiesDocument20 paginiEmergency Room Drugs Nursing ResponsibilitiestsikiÎncă nu există evaluări
- Central Nervous System: Drug of Choices Notes - Kent Andrei Paelma Bsn-2FDocument22 paginiCentral Nervous System: Drug of Choices Notes - Kent Andrei Paelma Bsn-2FOfficially RandomÎncă nu există evaluări
- SUPER PHARMA TABLE DRUG MOA AND ADVERSE EFFECTSDocument70 paginiSUPER PHARMA TABLE DRUG MOA AND ADVERSE EFFECTSalcojonic100% (2)
- Common Emergency DrugsDocument58 paginiCommon Emergency Drugshatem alsrour84% (19)
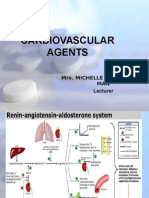
- Cardiovascular Agents: Mrs. Michelle A. Iduria, RN, MAN LecturerDocument131 paginiCardiovascular Agents: Mrs. Michelle A. Iduria, RN, MAN LecturerNiala AlmarioÎncă nu există evaluări
- Prehospital MedicationsDocument123 paginiPrehospital Medicationshilwaalfi100% (1)
- Antiarrhythmic AgentsDocument45 paginiAntiarrhythmic AgentsSoh Kae SiangÎncă nu există evaluări
- Emergency Drugs KathDocument29 paginiEmergency Drugs Kathmajin655Încă nu există evaluări
- Anti - Anginal MedicationDocument41 paginiAnti - Anginal MedicationShine StephenÎncă nu există evaluări
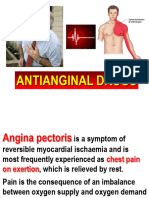
- Angina PectorisDocument4 paginiAngina PectorisAnn CunananÎncă nu există evaluări
- Drugs Used in Myocardial InfarctionDocument53 paginiDrugs Used in Myocardial InfarctionSandeep KannegantiÎncă nu există evaluări
- Angina Pectoris & Anti Anginal DrugsDocument46 paginiAngina Pectoris & Anti Anginal DrugsMohammad AliÎncă nu există evaluări
- FIGO Accreta Prenantal DiagnosisDocument7 paginiFIGO Accreta Prenantal DiagnosisYosef Dwi Cahyadi SalanÎncă nu există evaluări
- Calcium Channel BlockersDocument15 paginiCalcium Channel Blockersfarmasi_hm100% (2)
- Drugs Used in CcuDocument169 paginiDrugs Used in CcuAnusha Verghese100% (3)
- Elektroencephalogram & Proses Kesadaran: Departemen Fisiologi FK USUDocument21 paginiElektroencephalogram & Proses Kesadaran: Departemen Fisiologi FK USUYohanna SinuhajiÎncă nu există evaluări
- Antianginal Drugs Are Used Primarily To Restore The Balance Between The Oxygen SupplyDocument8 paginiAntianginal Drugs Are Used Primarily To Restore The Balance Between The Oxygen SupplyUzma KhanÎncă nu există evaluări
- Antianginal DrugsDocument47 paginiAntianginal Drugsmospala285Încă nu există evaluări
- Anti Angina (Hany)Document51 paginiAnti Angina (Hany)Angga AhadiyatÎncă nu există evaluări
- Antianginal Drugs Antianginal Drugs Are Used Primarily To Restore The Balance Between TheDocument10 paginiAntianginal Drugs Antianginal Drugs Are Used Primarily To Restore The Balance Between TheMIR SARTAJÎncă nu există evaluări
- Angina Pharmacology YeahDocument16 paginiAngina Pharmacology YeahMuhammad AfifuddinÎncă nu există evaluări
- Antiarrhytmic Talk For ResidenDocument90 paginiAntiarrhytmic Talk For ResidenMusa yohanaÎncă nu există evaluări
- Nitrates andDocument61 paginiNitrates andMrunalini DandamudiÎncă nu există evaluări
- Cardiac Medications: 1. Antiplatelet Aggregation Therapy: Antiplatelet Aggregation TherapyDocument14 paginiCardiac Medications: 1. Antiplatelet Aggregation Therapy: Antiplatelet Aggregation TherapyMaria OnofreiÎncă nu există evaluări
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreDocument112 paginiOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreabctutorÎncă nu există evaluări
- Pharmacology RevisedDocument59 paginiPharmacology Revisedjohnstockton12100% (1)
- 9 Drugs Affecting Angina PectorisDocument3 pagini9 Drugs Affecting Angina PectoristiaraÎncă nu există evaluări
- Obat-Obat Untuk Angina PectorisDocument31 paginiObat-Obat Untuk Angina PectorisChie ZhumieÎncă nu există evaluări
- Lab 11 AntianginalDocument4 paginiLab 11 AntianginalanaÎncă nu există evaluări
- Arrhythmias!Document49 paginiArrhythmias!mospala285Încă nu există evaluări
- Drugs For IHDDocument36 paginiDrugs For IHDASHUTOSH KHADANGAÎncă nu există evaluări
- Emergency Drugs GuideDocument8 paginiEmergency Drugs GuideShehnaz SheikhÎncă nu există evaluări
- Drugs Used for Treatment Stable Angina PectorisDocument29 paginiDrugs Used for Treatment Stable Angina PectorisAditya Andra PerdanaÎncă nu există evaluări
- Antianginal DrugsDocument38 paginiAntianginal Drugslemmademe204Încă nu există evaluări
- 10-11 Treatment of HypertensionDocument11 pagini10-11 Treatment of HypertensionHanif GandohÎncă nu există evaluări
- Cardiac DrugsDocument21 paginiCardiac DrugsMona MahfouzÎncă nu există evaluări
- Antianginal and Antiischemic DrugsDocument18 paginiAntianginal and Antiischemic DrugsNaveen KumarÎncă nu există evaluări
- Hypotensive AgentsDocument48 paginiHypotensive AgentsFaizan Ahmad AliÎncă nu există evaluări
- Anti-Angina Drugs for Chest Pain ReliefDocument60 paginiAnti-Angina Drugs for Chest Pain ReliefPranish SawantÎncă nu există evaluări
- Cad Sihd 2Document67 paginiCad Sihd 2mohammedghassan53Încă nu există evaluări
- Pharmacological-Management-of-HypertensionDocument35 paginiPharmacological-Management-of-Hypertensiontf.almutairi88Încă nu există evaluări
- Pcol Lab MidtermDocument26 paginiPcol Lab MidtermJoshua AysonÎncă nu există evaluări
- Antinanginal DrugsDocument43 paginiAntinanginal DrugsHUZAIFA YAMAANÎncă nu există evaluări
- RX Only Description: Isordil Titradose™ (Isosorbide Dinitrate) TabletsDocument8 paginiRX Only Description: Isordil Titradose™ (Isosorbide Dinitrate) TabletsazizhaÎncă nu există evaluări
- Last Edation Protocol Adan Ade HospitalDocument17 paginiLast Edation Protocol Adan Ade HospitalAxmed MaxamedÎncă nu există evaluări
- Anti-Anginal Drugs PharmacologyDocument24 paginiAnti-Anginal Drugs PharmacologyDharun RanganathanÎncă nu există evaluări
- Angina Types and TreatmentDocument44 paginiAngina Types and TreatmentsimonjosanÎncă nu există evaluări
- Antiarrhytmic Medications: ND RDDocument2 paginiAntiarrhytmic Medications: ND RDMack FarrellÎncă nu există evaluări
- Module 3.3 - CardioDocument12 paginiModule 3.3 - CardioCatherine Sinen ObinqueÎncă nu există evaluări
- Cardiovascular Drugs GuideDocument6 paginiCardiovascular Drugs GuideElizabella Henrietta TanaquilÎncă nu există evaluări
- Cardiac DrugDocument32 paginiCardiac DrugSalim MinjÎncă nu există evaluări
- Treatment Acute Ischemic StrokeDocument82 paginiTreatment Acute Ischemic StrokeTannov SiregarÎncă nu există evaluări
- Pharmacology Chapter 42 p-3Document19 paginiPharmacology Chapter 42 p-3sho bartÎncă nu există evaluări
- Antiaritmia: Frans D. Suyatna Modified by Sulistia 1010 Departemen Farmakologi & Terapeutik FKUIDocument56 paginiAntiaritmia: Frans D. Suyatna Modified by Sulistia 1010 Departemen Farmakologi & Terapeutik FKUIJoshua ObrienÎncă nu există evaluări
- Drugs For Ischemic Heart DiseaseDocument44 paginiDrugs For Ischemic Heart DiseaseMbah GapinbissiÎncă nu există evaluări
- Anti-Anginal and Antiischemic Drugs: Dr. Pradeepa H D Clinical PharmacologistDocument25 paginiAnti-Anginal and Antiischemic Drugs: Dr. Pradeepa H D Clinical PharmacologistpradeephdÎncă nu există evaluări
- AnginaDocument16 paginiAnginaMc_Lopez_1761Încă nu există evaluări
- Antihypertensive AgentsDocument52 paginiAntihypertensive Agentssameena ramzanÎncă nu există evaluări
- Antianginal Student222Document69 paginiAntianginal Student222MoonAIRÎncă nu există evaluări
- Antiadrenergic 180630054321Document19 paginiAntiadrenergic 180630054321Dinam Gyatso AadHenmooÎncă nu există evaluări
- Ischemic Heart DiseaseDocument31 paginiIschemic Heart DiseaseRohit SahÎncă nu există evaluări
- Diskusi Topik Anestesi GamaDocument65 paginiDiskusi Topik Anestesi Gamakusumagama28Încă nu există evaluări
- FI-Medicinal Chemistry 3Document40 paginiFI-Medicinal Chemistry 3Meri Apri YaniÎncă nu există evaluări
- Vasodilators and Drugs Used in The Treatment of Angina PectorisDocument52 paginiVasodilators and Drugs Used in The Treatment of Angina PectorisAbdiweli AbubakarÎncă nu există evaluări
- Amiodarone - A Closer LookDocument14 paginiAmiodarone - A Closer Lookmr.kenny.chengÎncă nu există evaluări
- Relief of Pain, Inflammation and Rheumatic ConditionsDocument16 paginiRelief of Pain, Inflammation and Rheumatic Conditionsdemolay03Încă nu există evaluări
- Common Emergency DrugsDocument61 paginiCommon Emergency DrugsFebee Gee100% (1)
- K1 - B2 - EBM TherapyDocument54 paginiK1 - B2 - EBM TherapyZikri Putra Lan LubisÎncă nu există evaluări
- K1 - B2 - EBM TherapyDocument54 paginiK1 - B2 - EBM TherapyZikri Putra Lan LubisÎncă nu există evaluări
- MEDICAL NUTRITION THERAPY FOR RENAL DISEASEDocument39 paginiMEDICAL NUTRITION THERAPY FOR RENAL DISEASESteven FongÎncă nu există evaluări
- Rts2-K52-Nutrition and Respiratory ProblemDocument43 paginiRts2-K52-Nutrition and Respiratory ProblemYohanna SinuhajiÎncă nu există evaluări
- GUS2-K7-2016 Pharmacology of Drugs ForDocument99 paginiGUS2-K7-2016 Pharmacology of Drugs ForYohanna SinuhajiÎncă nu există evaluări
- CVS2-K38-Acute Coronary SyndromeDocument35 paginiCVS2-K38-Acute Coronary SyndromeYohanna SinuhajiÎncă nu există evaluări
- Understanding Common Causes of Scrotal SwellingsDocument35 paginiUnderstanding Common Causes of Scrotal SwellingsYohanna SinuhajiÎncă nu există evaluări
- Crp5 k3 Prog PceDocument33 paginiCrp5 k3 Prog PceAde IndrawanÎncă nu există evaluări
- MEDICAL NUTRITION THERAPY FOR RENAL DISEASEDocument39 paginiMEDICAL NUTRITION THERAPY FOR RENAL DISEASESteven FongÎncă nu există evaluări
- K1 - B2 - EBM TherapyDocument54 paginiK1 - B2 - EBM TherapyZikri Putra Lan LubisÎncă nu există evaluări
- Crp5 k3 Prog PceDocument33 paginiCrp5 k3 Prog PceAde IndrawanÎncă nu există evaluări
- ID Pengaruh Terapi Oksigenasi Nasal Prong T PDFDocument7 paginiID Pengaruh Terapi Oksigenasi Nasal Prong T PDFhasbi aniÎncă nu există evaluări
- RTS1 K4 BronchiolitisDocument24 paginiRTS1 K4 BronchiolitisYohanna SinuhajiÎncă nu există evaluări
- Rts2-K52-Nutrition and Respiratory ProblemDocument43 paginiRts2-K52-Nutrition and Respiratory ProblemYohanna SinuhajiÎncă nu există evaluări
- RTS1-K13-Anatomy of LungsDocument22 paginiRTS1-K13-Anatomy of LungsYohanna SinuhajiÎncă nu există evaluări
- Farmakologi Antiaritmia (RZH)Document20 paginiFarmakologi Antiaritmia (RZH)Yohanna SinuhajiÎncă nu există evaluări
- ID Pengaruh Terapi Oksigenasi Nasal Prong T PDFDocument7 paginiID Pengaruh Terapi Oksigenasi Nasal Prong T PDFhasbi aniÎncă nu există evaluări
- The Pathophysiology of Hypertension: Abdul Majid/ Eka Roina MDocument51 paginiThe Pathophysiology of Hypertension: Abdul Majid/ Eka Roina MYohanna SinuhajiÎncă nu există evaluări
- K5 - EBM HarmDocument22 paginiK5 - EBM HarmYohanna SinuhajiÎncă nu există evaluări
- Farmakologi Antihiperlipidemia (RZH)Document24 paginiFarmakologi Antihiperlipidemia (RZH)Yohanna SinuhajiÎncă nu există evaluări
- CVS K39 Antiphospholipid Prof. HarimanDocument38 paginiCVS K39 Antiphospholipid Prof. HarimanYohanna SinuhajiÎncă nu există evaluări
- Infeksi Jamur pada Paru: Penyebab, Gejala, Diagnosis dan PengobatanDocument141 paginiInfeksi Jamur pada Paru: Penyebab, Gejala, Diagnosis dan PengobatanZikri Putra Lan LubisÎncă nu există evaluări
- PpipDocument32 paginiPpipYohanna SinuhajiÎncă nu există evaluări
- Eng PDFDocument92 paginiEng PDFPedro AtuanÎncă nu există evaluări
- Journal Reading ParuDocument53 paginiJournal Reading ParuDaniel IvanÎncă nu există evaluări
- CVS K38 Cardiac Enzymes Prof. HarimanDocument43 paginiCVS K38 Cardiac Enzymes Prof. HarimanYohanna SinuhajiÎncă nu există evaluări
- Laboratory Hemostatic DisordersDocument41 paginiLaboratory Hemostatic DisordersYohanna SinuhajiÎncă nu există evaluări
- Cardicor 2.5mg Tablets: (Bisoprolol Hemifumarate)Document4 paginiCardicor 2.5mg Tablets: (Bisoprolol Hemifumarate)Chris HartoyoÎncă nu există evaluări
- Anti HypertensivesDocument23 paginiAnti HypertensivesLeena AlateeqÎncă nu există evaluări
- Pharmacological and Parenteral Therapies RationalesDocument10 paginiPharmacological and Parenteral Therapies Rationalesrhymes2u83% (6)
- Cardio DrugsDocument58 paginiCardio DrugsMARIA ROWENA VIA J. LUCENAÎncă nu există evaluări
- Calcium Channel Blockers (CCBS)Document3 paginiCalcium Channel Blockers (CCBS)Yohanes SutrisnoÎncă nu există evaluări
- Drug Study: Tabije, Arvie Jayselle P. Marbella, IvyDocument15 paginiDrug Study: Tabije, Arvie Jayselle P. Marbella, IvyJaysellePuguonTabijeÎncă nu există evaluări
- NSAID Mechanism COX InhibitionDocument23 paginiNSAID Mechanism COX InhibitionWissam DadiÎncă nu există evaluări
- Verapamil PDFDocument13 paginiVerapamil PDFddandan_2Încă nu există evaluări
- Practice Test QuestionsDocument19 paginiPractice Test QuestionsEman ArmadoÎncă nu există evaluări
- VerapamilDocument2 paginiVerapamilMyla Reyes San MiguelÎncă nu există evaluări
- Anti-Anginal and Anti-Ischemic DrugsDocument18 paginiAnti-Anginal and Anti-Ischemic DrugsSrisriÎncă nu există evaluări
- Chapter 5 Drug StudyDocument16 paginiChapter 5 Drug StudyRegee Rose LacsonÎncă nu există evaluări
- 8B - Antianginal DrugsDocument70 pagini8B - Antianginal Drugslalitrajindolia100% (1)
- PHARMACOTHERAPEUTICS MCQSDocument17 paginiPHARMACOTHERAPEUTICS MCQSWwe 2Încă nu există evaluări
- Calcium Channel Blockers inDocument15 paginiCalcium Channel Blockers inAnonymous NeRC5JYiSÎncă nu există evaluări
- New Microsoft Word DocumentDocument79 paginiNew Microsoft Word DocumentalexpharmÎncă nu există evaluări
- Cardioversion of Atrial Fibrillation and Atrial Flutter Revisited: Current Evidence and Practical Guidance For A Common ProcedureDocument13 paginiCardioversion of Atrial Fibrillation and Atrial Flutter Revisited: Current Evidence and Practical Guidance For A Common ProcedureGian CarloÎncă nu există evaluări
- Anti-Anginal Drugs ExplainedDocument19 paginiAnti-Anginal Drugs ExplainedAnusha ZubairÎncă nu există evaluări
- Acls Prep Packet 2019aDocument86 paginiAcls Prep Packet 2019aSanti ParambangÎncă nu există evaluări
- Calcium Channel BlockersDocument3 paginiCalcium Channel BlockersrajeshmangalÎncă nu există evaluări
- Response of Cluster Headache To Kudzu (Complete)Document15 paginiResponse of Cluster Headache To Kudzu (Complete)Andy RotsaertÎncă nu există evaluări
- Antianginal Agents - PharmacologyDocument3 paginiAntianginal Agents - PharmacologyChona FontanillaÎncă nu există evaluări