S-ar putea să vă placă și
- ICU Scoring Systems A Complete Guide - 2020 EditionDe la EverandICU Scoring Systems A Complete Guide - 2020 EditionÎncă nu există evaluări
- Abdominal SurgeryDocument166 paginiAbdominal SurgeryIndera VyasÎncă nu există evaluări
- Primary Trauma Care Manual: Standard Edition 2010 A Manual For Trauma Management in District and Remote LocationsDocument37 paginiPrimary Trauma Care Manual: Standard Edition 2010 A Manual For Trauma Management in District and Remote Locationsdavid wyantoÎncă nu există evaluări
- English in Urgent Care Medicine – Anglictina V Urgentní Medicíne: Textbook – UcebniceDe la EverandEnglish in Urgent Care Medicine – Anglictina V Urgentní Medicíne: Textbook – UcebniceÎncă nu există evaluări
- Operating Room ManagementDocument4 paginiOperating Room ManagementJeremy Lyle JabonilloÎncă nu există evaluări
- Intubations Outside ICUDocument79 paginiIntubations Outside ICUzulham effendyÎncă nu există evaluări
- Initial Assessment and ManagementDocument8 paginiInitial Assessment and ManagementAlvin De LunaÎncă nu există evaluări
- Malaysiantriagescalenewrevised2019!1!221014090642 28d8e1aeDocument18 paginiMalaysiantriagescalenewrevised2019!1!221014090642 28d8e1aenaqibsakila4286Încă nu există evaluări
- Medical CompetenciesDocument22 paginiMedical CompetenciesDewi Putri Lenggo Geni100% (1)
- Student Refresher CourseDocument87 paginiStudent Refresher CourseRaisa S. MariscalÎncă nu există evaluări
- Trauma Thorax: Disusun Oleh: Uray Ria ApriniDocument22 paginiTrauma Thorax: Disusun Oleh: Uray Ria ApriniUray RiaÎncă nu există evaluări
- Nsg241 Study Guide Exam 5Document76 paginiNsg241 Study Guide Exam 5NatalieAndersonÎncă nu există evaluări
- Anaphylaxis With Angioedema: Section I: Scenario DemographicsDocument7 paginiAnaphylaxis With Angioedema: Section I: Scenario DemographicsharasthaÎncă nu există evaluări
- Endometrial Malignancies 1Document41 paginiEndometrial Malignancies 1jerrydanfordfxÎncă nu există evaluări
- Dr. Mirza Koeshardiandi ABC of BurnDocument35 paginiDr. Mirza Koeshardiandi ABC of Burnagus susantoÎncă nu există evaluări
- Trauma OverviewDocument48 paginiTrauma OverviewFrancescoBarbero100% (1)
- 11 Uterine CancerDocument43 pagini11 Uterine Cancerclaire yowsÎncă nu există evaluări
- Hospital Service Quality AsDocument20 paginiHospital Service Quality AsNurulfitrahhafidÎncă nu există evaluări
- Lifting and Moving PatientsDocument20 paginiLifting and Moving PatientsbrentupdegraffÎncă nu există evaluări
- PatientsafetyDocument21 paginiPatientsafetytuÎncă nu există evaluări
- Thoracic Trauma - Navy - PSPD 2021Document45 paginiThoracic Trauma - Navy - PSPD 2021Naavy LaksmonoÎncă nu există evaluări
- Master of Medicine in General SurgeryDocument8 paginiMaster of Medicine in General SurgeryAbdisalaan AbdulahiÎncă nu există evaluări
- Hospital Emergency Response ChecklistDocument26 paginiHospital Emergency Response ChecklistlupibudiÎncă nu există evaluări
- Acute Respiratory Distress: Section I: Scenario DemographicsDocument6 paginiAcute Respiratory Distress: Section I: Scenario DemographicsharasthaÎncă nu există evaluări
- Principles of Post Operative Care..Document21 paginiPrinciples of Post Operative Care..Namra MazharÎncă nu există evaluări
- Rapid Sequence IonDocument36 paginiRapid Sequence IonSyazwani MohamadÎncă nu există evaluări
- Surgical Cricothyrotomy (Assist)Document5 paginiSurgical Cricothyrotomy (Assist)ydtrgnÎncă nu există evaluări
- Basic Electrocardiogram (Ecg) : Mr. Hamza Ratrout Revised By: Dr. Irene RocoDocument28 paginiBasic Electrocardiogram (Ecg) : Mr. Hamza Ratrout Revised By: Dr. Irene Rocoأبوأحمد الحكيمÎncă nu există evaluări
- Lesson Plan Human Reproductive SystemDocument2 paginiLesson Plan Human Reproductive SystemGarnis HakimÎncă nu există evaluări
- Reinventing Medical Teaching and Learning For The 21st Century - Blended and Flipped Strategies PDFDocument6 paginiReinventing Medical Teaching and Learning For The 21st Century - Blended and Flipped Strategies PDFEnzoÎncă nu există evaluări
- Chapter 16 ITLS - 04-2020Document20 paginiChapter 16 ITLS - 04-2020Ahyar MohÎncă nu există evaluări
- First Aid in The Workplace: Code of PracticeDocument33 paginiFirst Aid in The Workplace: Code of PracticeJD100% (1)
- Basic Emergency CareDocument96 paginiBasic Emergency CareAnukriti MamgainÎncă nu există evaluări
- Sterilization Disinfection 1Document61 paginiSterilization Disinfection 1mynyaÎncă nu există evaluări
- EMS Burn Management PDFDocument30 paginiEMS Burn Management PDFRaymond Sitanaja0% (1)
- Initial Assesment and Management ATLS (Marissa)Document57 paginiInitial Assesment and Management ATLS (Marissa)jfsngdjÎncă nu există evaluări
- 3a - Occupational Safety ME 70 Basic Occupational Safety and HealthDocument91 pagini3a - Occupational Safety ME 70 Basic Occupational Safety and Healths.salise.allendaveÎncă nu există evaluări
- Bls Dewasa PKDJB 2022Document74 paginiBls Dewasa PKDJB 2022Halawatul ImanÎncă nu există evaluări
- Triage in Emergency Department: Triage Waiting Room Team LeaderDocument27 paginiTriage in Emergency Department: Triage Waiting Room Team LeaderJerry AbleÎncă nu există evaluări
- The Newcastle Upon Tyne Hospitals NHS Foundation Trust Count ProcedureDocument42 paginiThe Newcastle Upon Tyne Hospitals NHS Foundation Trust Count ProcedureGina AprianaÎncă nu există evaluări
- Basic Concept of BLS: Muhammad SaleemDocument27 paginiBasic Concept of BLS: Muhammad Saleemms khanÎncă nu există evaluări
- Et IntubateDocument47 paginiEt IntubatectuagentÎncă nu există evaluări
- OxygenationDocument50 paginiOxygenationLulu MushiÎncă nu există evaluări
- Early Assessment of Trauma Patients and ATLSDocument45 paginiEarly Assessment of Trauma Patients and ATLSTILAHUNÎncă nu există evaluări
- Shock On TraumaDocument36 paginiShock On TraumaMeviraf BennyÎncă nu există evaluări
- Early Warning Score & Rapid Response TeamDocument26 paginiEarly Warning Score & Rapid Response TeamAsim IdreesÎncă nu există evaluări
- Advanced Airway Management: Leaugeay Webre, BS, CCEMT-P, Nremt-PDocument35 paginiAdvanced Airway Management: Leaugeay Webre, BS, CCEMT-P, Nremt-Pbasic100% (4)
- Who Patient SafetyDocument14 paginiWho Patient SafetyJuwita Valen RamadhanniaÎncă nu există evaluări
- Chapter 08 ITLS - 04-2020Document36 paginiChapter 08 ITLS - 04-2020Ahyar Moh100% (1)
- 633815699386510632Document123 pagini633815699386510632Muhammad FarisÎncă nu există evaluări
- BATLSDocument70 paginiBATLSVitor Hugo G CorreiaÎncă nu există evaluări
- Emergency ProceduresDocument5 paginiEmergency Proceduresmardemomin100% (1)
- Redbook - ASSESSMENT AND MANAGEMENT OF TRAUMA PDFDocument323 paginiRedbook - ASSESSMENT AND MANAGEMENT OF TRAUMA PDFrizka100% (1)
- Approach For Poly-Trauma PatientDocument63 paginiApproach For Poly-Trauma PatientvadimmadanÎncă nu există evaluări
- prehospital-EMS-COVID-19-recommendations - 4.4Document19 paginiprehospital-EMS-COVID-19-recommendations - 4.4MEONEÎncă nu există evaluări
- Airway ACLSDocument29 paginiAirway ACLSJoshua KosowskyÎncă nu există evaluări
- Principles of Trauma ManagementDocument60 paginiPrinciples of Trauma ManagementDrArish Mahmood100% (1)
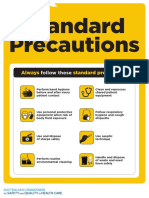
- Approach 4 Standard Precautions Icon PDF 672KBDocument1 paginăApproach 4 Standard Precautions Icon PDF 672KBElaine MacalandaÎncă nu există evaluări
- 10 Patient Safety and Invasive ProceduresDocument4 pagini10 Patient Safety and Invasive Proceduresanojan100% (1)
- Course Exercise - ACLS Precourse Self-Assessment and Precourse WorkDocument3 paginiCourse Exercise - ACLS Precourse Self-Assessment and Precourse WorksameerocksÎncă nu există evaluări
- BLS-First Aid (FTP-OJT) - 1Document43 paginiBLS-First Aid (FTP-OJT) - 1TMRU TCPSÎncă nu există evaluări
- Jurnal Trauma KepalaDocument4 paginiJurnal Trauma KepalaIlham Nur KasgoroÎncă nu există evaluări
- Stop The Bleed BookletDocument16 paginiStop The Bleed Bookletmoises ninaÎncă nu există evaluări
- Head InjuryDocument13 paginiHead InjuryMay NitayakulÎncă nu există evaluări
- 2021 Cape Town Atls Course ScheduleDocument2 pagini2021 Cape Town Atls Course Schedulermullah23Încă nu există evaluări
- Chest Injuries, What The Sport Therapist Should Know - Article.Document4 paginiChest Injuries, What The Sport Therapist Should Know - Article.salmankhan09215Încă nu există evaluări
- 3BLS Adult Skill Testing Checklist 2020Document1 pagină3BLS Adult Skill Testing Checklist 2020Bloody DoctorÎncă nu există evaluări
- Journal of Clinical Orthopaedics and TraumaDocument8 paginiJournal of Clinical Orthopaedics and TraumaandiÎncă nu există evaluări
- GREY BOOK August 2022 75th EditionDocument155 paginiGREY BOOK August 2022 75th EditionMohamed AbdelmoniemÎncă nu există evaluări
- Causes of Death in BurnsDocument9 paginiCauses of Death in Burnsniraj_sdÎncă nu există evaluări
- Copy of Q3-PPT-HEALTH 9 (Dressing and Bandages)Document36 paginiCopy of Q3-PPT-HEALTH 9 (Dressing and Bandages)ADRIAN ELISEOÎncă nu există evaluări
- 2020 ECC GuidelinesDocument32 pagini2020 ECC GuidelinesKevin Michael Reyes Roque100% (1)
- Chapter 27 Chest InjuriesDocument70 paginiChapter 27 Chest Injuriesventus virÎncă nu există evaluări
- First AidDocument10 paginiFirst AidRachita PatangiÎncă nu există evaluări
- Auckland HEMS Checklist Reference 2014Document29 paginiAuckland HEMS Checklist Reference 2014Jorge JoÎncă nu există evaluări
- Standard Operating Procedure: R04: Sequence of Actions When Using An Automated External Defibrillator (AED)Document5 paginiStandard Operating Procedure: R04: Sequence of Actions When Using An Automated External Defibrillator (AED)AnggriawanCaesarNurfattahÎncă nu există evaluări
- Pediatric Basic Life SupportDocument30 paginiPediatric Basic Life Supportkariuki90406978Încă nu există evaluări
- Forensic Aspects of Complications Resulting From Cardiopulmonary ResuscitationDocument6 paginiForensic Aspects of Complications Resulting From Cardiopulmonary ResuscitationMadul15Încă nu există evaluări
- Glasgow Coma Scale GCSDocument4 paginiGlasgow Coma Scale GCScardiacanesthesiaÎncă nu există evaluări
- Sports and Activity First Aid PDFDocument2 paginiSports and Activity First Aid PDFVITALÎncă nu există evaluări
- NSTP Script KishaDocument2 paginiNSTP Script KishaKisha Nicole R. EnanoriaÎncă nu există evaluări
- Assessment-Task-1 SolutionDocument29 paginiAssessment-Task-1 SolutionMirajur Rahman 1722007Încă nu există evaluări
- Shock: Bethelhem BerhanuDocument33 paginiShock: Bethelhem BerhanuAbdelrahman M. AlnweiriÎncă nu există evaluări
- How To Use An AED - Automatic External DefibrillatorDocument4 paginiHow To Use An AED - Automatic External DefibrillatorMiguel BarreirosÎncă nu există evaluări
- Advanced Cardiovascular Life Support (ACLS)Document2 paginiAdvanced Cardiovascular Life Support (ACLS)Vijay MgÎncă nu există evaluări
- JADWAL ATLS Semarang 10-12 Agustus 2018 (1654) Utk PesertaDocument5 paginiJADWAL ATLS Semarang 10-12 Agustus 2018 (1654) Utk PesertafebriÎncă nu există evaluări
- Incorrect - Right Answer: True: CorrectDocument10 paginiIncorrect - Right Answer: True: CorrectAhmed - Sawalha100% (2)
- The Stay Alive GuideDocument82 paginiThe Stay Alive GuideTaylor PiersonÎncă nu există evaluări
- First Aid: List of ContentsDocument42 paginiFirst Aid: List of ContentsNasser HashimÎncă nu există evaluări