S-ar putea să vă placă și
- Pain PhysiologyDocument51 paginiPain Physiologyvladex77100% (1)
- 1 Pain Sensation Physiology DR Ambreen TauseefDocument73 pagini1 Pain Sensation Physiology DR Ambreen TauseefbilalÎncă nu există evaluări
- Mr. M. Shiva Nandha ReddyDocument71 paginiMr. M. Shiva Nandha Reddyd kumarÎncă nu există evaluări
- PainDocument44 paginiPainCarl Elexer Cuyugan Ano100% (4)
- Types of PainDocument3 paginiTypes of PainSab IbarretaÎncă nu există evaluări
- Anemia: Presented byDocument36 paginiAnemia: Presented byParmvir Singh100% (1)
- A&P - 2. Blood Vessels of The Brain (9p)Document9 paginiA&P - 2. Blood Vessels of The Brain (9p)Gabriel StratulatÎncă nu există evaluări
- Anterior Abdominal Wall and Inguinal CanalDocument35 paginiAnterior Abdominal Wall and Inguinal Canalapi-3698357100% (3)
- Pain Pathways IntroductionDocument7 paginiPain Pathways Introductionganpur01100% (1)
- Amputation: Sites of Amputation: UEDocument6 paginiAmputation: Sites of Amputation: UEChristine PilarÎncă nu există evaluări
- TB SpineDocument15 paginiTB SpineChe AinÎncă nu există evaluări
- Clinical Case PresentationDocument14 paginiClinical Case PresentationJhanviÎncă nu există evaluări
- Median NerveDocument40 paginiMedian Nervehumera100% (2)
- Acute Lung Injury and Ards: Andreas Crede Emergency Medicine RegistrarDocument47 paginiAcute Lung Injury and Ards: Andreas Crede Emergency Medicine RegistrarYohanes FirmansyahÎncă nu există evaluări
- Pain SeminarDocument25 paginiPain SeminarsruthiÎncă nu există evaluări
- Neurology - : Approach To Headache DisordersDocument8 paginiNeurology - : Approach To Headache DisordersKarenÎncă nu există evaluări
- 1 Pain AssessmentDocument13 pagini1 Pain AssessmentQuijano GpokskieÎncă nu există evaluări
- Spinal Cord TumorsDocument23 paginiSpinal Cord TumorsTahleel AltafÎncă nu există evaluări
- Blood Supply Pelvic OrgansDocument39 paginiBlood Supply Pelvic OrgansoliviaÎncă nu există evaluări
- Interferential Therapy 2021Document13 paginiInterferential Therapy 2021Mộng HoàngÎncă nu există evaluări
- Long Term ComplicationsDocument18 paginiLong Term Complicationsapi-3705046Încă nu există evaluări
- Orthopedic Fixation DevicesDocument9 paginiOrthopedic Fixation DevicesJoel Santos100% (1)
- Myasthenia Gravis and Other Neuromuscular Junction DisordersDocument8 paginiMyasthenia Gravis and Other Neuromuscular Junction Disordersidno1008Încă nu există evaluări
- Scapulohumeral PeriarthritisDocument29 paginiScapulohumeral PeriarthritisMárcia PatríciaÎncă nu există evaluări
- Physiology of PainDocument25 paginiPhysiology of PainAsim NawazÎncă nu există evaluări
- VertebraeDocument32 paginiVertebraeAndre saputraÎncă nu există evaluări
- Slides For SeizureDocument15 paginiSlides For SeizureBryan Mae H. Degorio100% (3)
- Spinal Cord: DR Ganesh Khemnar Assistant Professor Dept. of Anatomy BVDUMC, PuneDocument43 paginiSpinal Cord: DR Ganesh Khemnar Assistant Professor Dept. of Anatomy BVDUMC, PunePraneetha NouduriÎncă nu există evaluări
- Neurological AssessmentDocument20 paginiNeurological Assessmentdhanya jayan100% (1)
- Anatomy of GI TractDocument24 paginiAnatomy of GI TractMuhammad Ade RahmanÎncă nu există evaluări
- Tutorial 8 Cardiac ExamDocument14 paginiTutorial 8 Cardiac Examcindy100% (1)
- SPINAL CORD DISORDERS YaredDocument83 paginiSPINAL CORD DISORDERS YaredBethelhem Berhanu50% (2)
- Anes Preoperative-AssessmentDocument6 paginiAnes Preoperative-AssessmentChristine Mendoza100% (1)
- Brachial Plexus InjuriesDocument64 paginiBrachial Plexus Injuriesprashanth naikÎncă nu există evaluări
- Obstetric PalsyDocument4 paginiObstetric PalsyDelphy VargheseÎncă nu există evaluări
- MedicalDocument29 paginiMedicalZia Ur RehmanÎncă nu există evaluări
- Caudal BlockDocument6 paginiCaudal BlockAshish PandeyÎncă nu există evaluări
- NeuroblastomaDocument33 paginiNeuroblastomahariÎncă nu există evaluări
- Spinal Cord InjuryDocument49 paginiSpinal Cord InjuryIis Rica MustikaÎncă nu există evaluări
- Theories of Pain MechanismDocument16 paginiTheories of Pain MechanismGithaiga KimaniÎncă nu există evaluări
- MicturitionDocument7 paginiMicturitionOsama MohamedÎncă nu există evaluări
- Cerebral Venous Thrombosis PDFDocument7 paginiCerebral Venous Thrombosis PDFd dÎncă nu există evaluări
- UnconsciousnessDocument16 paginiUnconsciousnessAkhilesh BabuÎncă nu există evaluări
- Pain PathwayDocument17 paginiPain PathwaySalsabila Al-BasheerÎncă nu există evaluări
- For Controlled Cough Technique: RatingDocument3 paginiFor Controlled Cough Technique: RatingJojo JustoÎncă nu există evaluări
- Pain PathwayDocument70 paginiPain PathwayDr Mirunalini SundaravadiveluÎncă nu există evaluări
- Bone Marrow and Stem Cell TranspplantDocument28 paginiBone Marrow and Stem Cell TranspplantVILLEJO JHOVIALENÎncă nu există evaluări
- Cerumen Impaction FinalDocument8 paginiCerumen Impaction FinalRose Ann Del MundoÎncă nu există evaluări
- Bartholin's Cyst/AbscessDocument6 paginiBartholin's Cyst/AbscessJane NathaniaÎncă nu există evaluări
- Vertebral Arteries, and Their Divisions. Arteries Fuse To Form The Basilar ArteryDocument6 paginiVertebral Arteries, and Their Divisions. Arteries Fuse To Form The Basilar Arterymurali_bharadwazÎncă nu există evaluări
- Congenital Dysplasia of Hip (CDH) Developmental Dysplasia of The Hip (DDH)Document50 paginiCongenital Dysplasia of Hip (CDH) Developmental Dysplasia of The Hip (DDH)NarishaAmeliaÎncă nu există evaluări
- Cerebral Venous ThrombosisDocument15 paginiCerebral Venous ThrombosisValentina RobuÎncă nu există evaluări
- Warning Signs of Various DiseasesDocument44 paginiWarning Signs of Various DiseasesamsabavanÎncă nu există evaluări
- Hand and WristDocument5 paginiHand and WristcpÎncă nu există evaluări
- Obstetric Emergencies PDFDocument15 paginiObstetric Emergencies PDFEdi BackyÎncă nu există evaluări
- EMG-NCV Tests Biofeedback: Dr. Vaishali (PT), Sr. Lecturer, AIMS, AhmedabadDocument119 paginiEMG-NCV Tests Biofeedback: Dr. Vaishali (PT), Sr. Lecturer, AIMS, AhmedabadSakshi Gadhvi100% (1)
- DR - Lajja Bhagat MPT (Cardiopulmonary)Document49 paginiDR - Lajja Bhagat MPT (Cardiopulmonary)Lajja Bhagat Shah100% (1)
- Nervous System - Somatosensory Pathways Fall 2021Document32 paginiNervous System - Somatosensory Pathways Fall 2021ElenaÎncă nu există evaluări
- Pain PhysiologyDocument40 paginiPain PhysiologyAnmol Jain100% (1)
- Neurobiology of Pain: C R MishraDocument47 paginiNeurobiology of Pain: C R MishraKing Bradley100% (2)
- Anna Billion - Kundalini - Secrets of The Ancient YogisDocument226 paginiAnna Billion - Kundalini - Secrets of The Ancient Yogisomran97100% (8)
- How The Way You Move Can Change The Way You Think and Feel: HealthDocument9 paginiHow The Way You Move Can Change The Way You Think and Feel: HealthThiago TinocoÎncă nu există evaluări
- Overview: Functions of The CerebellumDocument17 paginiOverview: Functions of The CerebellumMohd Fitri ShahruddinÎncă nu există evaluări
- Pertemuan 2 ElearningDocument6 paginiPertemuan 2 ElearningFather & SonÎncă nu există evaluări
- Gerser, 2005Document10 paginiGerser, 2005Elisabet GobelliÎncă nu există evaluări
- K 1 2 Formatio Reticularis & Sistem LimbikDocument39 paginiK 1 2 Formatio Reticularis & Sistem LimbikfelixÎncă nu există evaluări
- Autopsy of Baby WyllowDocument10 paginiAutopsy of Baby WyllowKOLD News 13100% (1)
- Grade 5 RevisionDocument3 paginiGrade 5 RevisionshamshadÎncă nu există evaluări
- Vesela Mih Thesis SMDocument102 paginiVesela Mih Thesis SMJohnÎncă nu există evaluări
- The Use of Machine Learning and Neural Networks in The Digital Economy and International Digital IntegrationDocument6 paginiThe Use of Machine Learning and Neural Networks in The Digital Economy and International Digital IntegrationOpen Access JournalÎncă nu există evaluări
- How Science Learned Rev 10-09Document26 paginiHow Science Learned Rev 10-09Victor PopaÎncă nu există evaluări
- Dokumen - Tips - Meeting 1 NounsDocument5 paginiDokumen - Tips - Meeting 1 NounsMila WdyntÎncă nu există evaluări
- College of Arts and SciencesDocument33 paginiCollege of Arts and SciencesTrizha NeraÎncă nu există evaluări
- Review of Clinical EEGDocument200 paginiReview of Clinical EEGtuanamg66100% (10)
- Nitrous OxideDocument43 paginiNitrous OxideSatpreet SinghÎncă nu există evaluări
- Thank You For EverythingDocument238 paginiThank You For EverythingKeith Nuena100% (3)
- Individualized Teaching - Full ReportDocument26 paginiIndividualized Teaching - Full ReportDarpan VyasÎncă nu există evaluări
- 1to7.2.2020 Discussion QUESTIONS PDFDocument63 pagini1to7.2.2020 Discussion QUESTIONS PDFJulyhathul KuraishiÎncă nu există evaluări
- Human Brain EssayDocument6 paginiHuman Brain Essayafhbgdmbt100% (2)
- The Encyclopedia of NootropicsDocument231 paginiThe Encyclopedia of NootropicsBorakÎncă nu există evaluări
- Q. What Is Recognition-By - Components Model? How Is It Different From Feature - Matching Model?Document3 paginiQ. What Is Recognition-By - Components Model? How Is It Different From Feature - Matching Model?Ushasi PalÎncă nu există evaluări
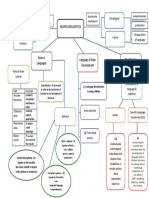
- Neurolingusitics: Brain & Languages Language & Brain Development The Modular MindDocument1 paginăNeurolingusitics: Brain & Languages Language & Brain Development The Modular MindhamizahÎncă nu există evaluări
- MidBrain ActivationDocument29 paginiMidBrain ActivationSandeep Kumar Sai100% (3)
- Department of Education: 2nd Quarter Trends Networks and Critical Thinking Skills in The 21 Century-12Document7 paginiDepartment of Education: 2nd Quarter Trends Networks and Critical Thinking Skills in The 21 Century-12Garry QuezonÎncă nu există evaluări
- Reflectiveessay BrainDocument5 paginiReflectiveessay Brainapi-305353379Încă nu există evaluări
- Musicality and The Intrinsic Motive Pulse: Evidence From Human Psychobiology and Infant CommunicationDocument61 paginiMusicality and The Intrinsic Motive Pulse: Evidence From Human Psychobiology and Infant CommunicationEdwin Yahir GalvisÎncă nu există evaluări
- You Can Grow Your IntelligenceDocument4 paginiYou Can Grow Your IntelligenceLauren FlynnÎncă nu există evaluări
- The Idea of The Brain Matthew CobbDocument2 paginiThe Idea of The Brain Matthew CobblaurakaiohÎncă nu există evaluări
- U3L1 Student GuideDocument3 paginiU3L1 Student GuideJosieÎncă nu există evaluări
- WMM EvaluationDocument3 paginiWMM EvaluationWilliamÎncă nu există evaluări