S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- MASLP Syllabus IndiaDocument11 paginiMASLP Syllabus IndiaVedashri14Încă nu există evaluări
- Chapter 16 SummaryDocument3 paginiChapter 16 SummaryMary Dominique RomoÎncă nu există evaluări
- Hearing Loss AafpDocument14 paginiHearing Loss AafpAhdaÎncă nu există evaluări
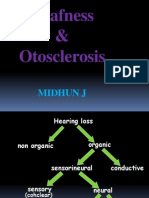
- Deafness & Otosclerosis: Midhun JDocument44 paginiDeafness & Otosclerosis: Midhun JRohit R PillaiÎncă nu există evaluări
- The Importance of Early Intervention of Hearing Impaired ChildrenDocument4 paginiThe Importance of Early Intervention of Hearing Impaired ChildrenAkhsaful ImamÎncă nu există evaluări
- Hearing DisorderDocument64 paginiHearing DisorderЭ.ТөгөлдөрÎncă nu există evaluări
- A. Atresia Surgery On at Least One Ear by Age 3 Years: B. Bone-Anchored Hearing Aid (BAHA) Soft BandDocument37 paginiA. Atresia Surgery On at Least One Ear by Age 3 Years: B. Bone-Anchored Hearing Aid (BAHA) Soft Bandevamirandafitri19Încă nu există evaluări
- Causes of Hearing LossDocument2 paginiCauses of Hearing LossAdjei Fosu KennedyÎncă nu există evaluări
- Hearing Loss - A Clinical ApproachDocument70 paginiHearing Loss - A Clinical ApproachJohnson Jayaraj100% (2)
- MCQS Sensory ImpairmentDocument8 paginiMCQS Sensory ImpairmentHasnain Raza MuhammadiÎncă nu există evaluări
- cmd0111 Oip Vol 15 Issue 1 - 2014 3 p19-28 Karas Interactive PDF d6.0Document12 paginicmd0111 Oip Vol 15 Issue 1 - 2014 3 p19-28 Karas Interactive PDF d6.0CARDENAS BARRETO JUAN PABLOÎncă nu există evaluări
- Discussion Paper On Hearing LossDocument36 paginiDiscussion Paper On Hearing LossAsha ShivaramÎncă nu există evaluări
- (What Do I Do Now - ) Darius Kohan, Selena Heman-Ackah, Sujana Chandrasekhar - Neurotology (2014, Oxford University Press)Document249 pagini(What Do I Do Now - ) Darius Kohan, Selena Heman-Ackah, Sujana Chandrasekhar - Neurotology (2014, Oxford University Press)Anoop Singh100% (1)
- Unit 4 Sensation and Perception Problem Solving Activities Team AssignmentsDocument7 paginiUnit 4 Sensation and Perception Problem Solving Activities Team AssignmentsmuntahaÎncă nu există evaluări
- Haniah RDocument7 paginiHaniah RHaniah DitanongunÎncă nu există evaluări
- Geriatric OtolaryngologyDocument26 paginiGeriatric OtolaryngologySari RakhmawatiÎncă nu există evaluări
- Hearing Aid InformationDocument22 paginiHearing Aid InformationDeepakRodeyÎncă nu există evaluări
- TinnitusDocument60 paginiTinnitusYowendruJunÎncă nu există evaluări
- Sensorineural Hearing LossDocument19 paginiSensorineural Hearing LossBenitaÎncă nu există evaluări
- Noise - AnswerDocument36 paginiNoise - AnswerPankajÎncă nu există evaluări
- Rehabilitacion PlasticidadDocument9 paginiRehabilitacion Plasticidadn_almagroÎncă nu există evaluări
- PresbyacusisDocument15 paginiPresbyacusisP MilanÎncă nu există evaluări
- Ayurvedic Management and Rehabilitation Therapy For Vardhakyajanya BadhiryaDocument4 paginiAyurvedic Management and Rehabilitation Therapy For Vardhakyajanya BadhiryaEditor IJTSRDÎncă nu există evaluări
- Cochlear Vs Retrocochlear LesionsDocument14 paginiCochlear Vs Retrocochlear LesionsDario ReyesÎncă nu există evaluări
- Unit 4Document37 paginiUnit 4PoonguzhaliÎncă nu există evaluări
- HEENT Nursing AssessmentDocument12 paginiHEENT Nursing AssessmentMelissa Aina Mohd Yusof100% (1)
- 3043Document3 pagini3043Lucy Lukova-DemingÎncă nu există evaluări
- AAT Presbyacusis Sudden Deafness Menierre DiseaseDocument47 paginiAAT Presbyacusis Sudden Deafness Menierre DiseaseHananya ManroeÎncă nu există evaluări
- Presbycusi S: By: April Fischer CSD 771 Case StudyDocument26 paginiPresbycusi S: By: April Fischer CSD 771 Case Studyminal madcapÎncă nu există evaluări
- Middle AdulthoodDocument21 paginiMiddle AdulthoodDamielle DacanayÎncă nu există evaluări