S-ar putea să vă placă și
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Gyproc Regular Ceiling Plasterboard: Technical & Safety DatasheetDocument6 paginiGyproc Regular Ceiling Plasterboard: Technical & Safety DatasheetAbdelmuneimÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Jurnal 1Document8 paginiJurnal 1Dela Amelia Nur SalehaÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- MSDS Easy UPS Battery Pack - PB EN SDS v1-5 APCDocument16 paginiMSDS Easy UPS Battery Pack - PB EN SDS v1-5 APCtino mediamudaÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Anesthesiology ManualDocument131 paginiAnesthesiology ManualHarlyn Magsino100% (1)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
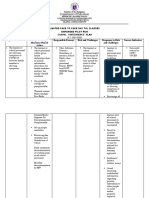
- Department of Education: School Contingency PlanDocument8 paginiDepartment of Education: School Contingency PlanNIMFA SEPARAÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Kuliayada CaafimaadkaDocument50 paginiKuliayada CaafimaadkaKhalid Abdiaziz AbdulleÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Secondhand Smoke ConsumerDocument11 paginiSecondhand Smoke ConsumerДанила НеделкуÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Material Safety Data Sheet: TM TMDocument6 paginiMaterial Safety Data Sheet: TM TMAris WicaksonoÎncă nu există evaluări
- Respiratory System - Charts and Graphs 2023Document16 paginiRespiratory System - Charts and Graphs 2023MamathaÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- 1 Material Safety Data Sheet: Alchol-Ether Mixture MSDSDocument6 pagini1 Material Safety Data Sheet: Alchol-Ether Mixture MSDSA.N. MÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Modul ASTHMA Ardine-VitaDocument34 paginiModul ASTHMA Ardine-VitayuliaevitasariÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Chapter 7 CPRDocument6 paginiChapter 7 CPRboltuÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Nurse'S Notes Name: - Cleopatra Andude - Age/Sex/CS: - 36/F/M - Ward/Room: - Obward-123 - ATTENDING PHYSICIAN - Dr. Danilo DizonDocument3 paginiNurse'S Notes Name: - Cleopatra Andude - Age/Sex/CS: - 36/F/M - Ward/Room: - Obward-123 - ATTENDING PHYSICIAN - Dr. Danilo DizonRenea Joy ArruejoÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- 13 Areas of AssessmentDocument39 pagini13 Areas of AssessmentKate CortinaÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Scenario Presentation Newborn in Need of PPV and IntubationDocument3 paginiScenario Presentation Newborn in Need of PPV and IntubationMaria PârghieÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Material Safety Data Sheet: Section 1 - Chemical Product / Company InformationDocument5 paginiMaterial Safety Data Sheet: Section 1 - Chemical Product / Company InformationMarcy Viviana Chiquillo MarquezÎncă nu există evaluări
- Trikloretilen MSDSDocument8 paginiTrikloretilen MSDSserhat simsekÎncă nu există evaluări
- MSDS-H1D572C-WB Primer White OutdoorDocument3 paginiMSDS-H1D572C-WB Primer White Outdooragung satriaÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- ACLS Exam Version ADocument11 paginiACLS Exam Version AAhmed - Sawalha97% (29)
- Pulmonary Nodules and Masses After Lung and Heart-Lung TransplantationDocument7 paginiPulmonary Nodules and Masses After Lung and Heart-Lung TransplantationManisha UppalÎncă nu există evaluări
- Pengadaan Bahan Habis Pakai Medis Di Rumah Sakit Universitas Brawijaya Periode Bulan Januari - Maret 2017Document13 paginiPengadaan Bahan Habis Pakai Medis Di Rumah Sakit Universitas Brawijaya Periode Bulan Januari - Maret 2017Melin Agnesha0% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Child CPR: Skills Testing ChecklistDocument3 paginiChild CPR: Skills Testing ChecklistTravis TravoltaÎncă nu există evaluări
- Call For The Other Side of Justice By: Halima B. AbdulmaguidDocument1 paginăCall For The Other Side of Justice By: Halima B. AbdulmaguidRy FernandezÎncă nu există evaluări
- Evaluation of Dyspneic PatientDocument15 paginiEvaluation of Dyspneic Patientcamila perillaÎncă nu există evaluări
- Physiology MCQS: Week 12Document3 paginiPhysiology MCQS: Week 12AzizÎncă nu există evaluări
- Artikel KKN 15 - A.rizal Dwiki RivaldhyDocument17 paginiArtikel KKN 15 - A.rizal Dwiki RivaldhyArizal RivaldhyÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- TG101 DOSELimitDocument2 paginiTG101 DOSELimitZhicong Huang100% (1)
- Case Study About Cystic Fibrosis GeneDocument40 paginiCase Study About Cystic Fibrosis GeneEvora, Sichem D.Încă nu există evaluări
- HEMP-005 Excavation Manual & Mechanical Rev.2Document9 paginiHEMP-005 Excavation Manual & Mechanical Rev.2saravana.bÎncă nu există evaluări
- AWFA+First+Aid+E-Manual+Vs5.3 Aug+2019Document88 paginiAWFA+First+Aid+E-Manual+Vs5.3 Aug+2019Tomas BravoÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)