S-ar putea să vă placă și
- LASER IN CONSERVATIVE DENTISTRY -NHDocument39 paginiLASER IN CONSERVATIVE DENTISTRY -NHAiluul AlmaaÎncă nu există evaluări
- Key ActivitiesDocument1 paginăKey ActivitiesAiluul AlmaaÎncă nu există evaluări
- Catatan Kuliah SubmandibularDocument2 paginiCatatan Kuliah SubmandibularAiluul AlmaaÎncă nu există evaluări
- Junk File Aploa ScribeDocument1 paginăJunk File Aploa ScribeAiluul AlmaaÎncă nu există evaluări
- Egg RollDocument3 paginiEgg RollAiluul AlmaaÎncă nu există evaluări
- Berman Fa atDocument1 paginăBerman Fa atAiluul AlmaaÎncă nu există evaluări
- Rainbow CakeDocument3 paginiRainbow CakeAiluul AlmaaÎncă nu există evaluări
- Junk File Aploa ScribeDocument1 paginăJunk File Aploa ScribeAiluul AlmaaÎncă nu există evaluări
- Nama: Ailuul Almaa Adiwangsa NIM: 22010217120010Document2 paginiNama: Ailuul Almaa Adiwangsa NIM: 22010217120010Ailuul AlmaaÎncă nu există evaluări
- 14 PDFDocument1.474 pagini14 PDFAiluul Almaa100% (2)
- Crossbite Posterior Perb-WPS OfficeDocument1 paginăCrossbite Posterior Perb-WPS OfficeAiluul AlmaaÎncă nu există evaluări
- Dampak Pemakaian GT Mahkota Terhadap Kesehatan Jaringan GingivaDocument1 paginăDampak Pemakaian GT Mahkota Terhadap Kesehatan Jaringan GingivaAiluul AlmaaÎncă nu există evaluări
- Delayed Tooth Eruption Pa Tho Genesis, Diagnosis and Treatment.Document14 paginiDelayed Tooth Eruption Pa Tho Genesis, Diagnosis and Treatment.DrFarhana AfzalÎncă nu există evaluări
- EarlyDocument1 paginăEarlyAiluul AlmaaÎncă nu există evaluări
- The Relation Between Salivary Siga Level and Caries Incidence in Down Syndrome ChildrenDocument5 paginiThe Relation Between Salivary Siga Level and Caries Incidence in Down Syndrome ChildrenAiluul AlmaaÎncă nu există evaluări
- Pathogenesis of Dental Fluorosis: Biochemical and Cellular MechanismsDocument15 paginiPathogenesis of Dental Fluorosis: Biochemical and Cellular MechanismsAiluul AlmaaÎncă nu există evaluări
- Resin Modified WPS OfficeDocument2 paginiResin Modified WPS OfficeAiluul AlmaaÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Key Words: Pathological Dissociation, Detachment, Compartmentalization, ClassificationDocument8 paginiKey Words: Pathological Dissociation, Detachment, Compartmentalization, ClassificationSilviaNathaliaÎncă nu există evaluări
- KeynoteAdvanced Unit1 Readingp15Document3 paginiKeynoteAdvanced Unit1 Readingp15Anh-5A-18 Vũ Ngọc ThảoÎncă nu există evaluări
- Diabettes Mellitus and Cognitive ImpairmentsDocument12 paginiDiabettes Mellitus and Cognitive ImpairmentsPutri YunandaÎncă nu există evaluări
- KINESIOLOGY CHAPTER 2 MOVEMENTSDocument36 paginiKINESIOLOGY CHAPTER 2 MOVEMENTSZuhaib AhmedÎncă nu există evaluări
- Soft Skills Guiding NotesDocument34 paginiSoft Skills Guiding NotesRajick MusiqÎncă nu există evaluări
- Types of ListeningDocument2 paginiTypes of ListeningCrisalyn SicatÎncă nu există evaluări
- Brain Structure and FunctionDocument4 paginiBrain Structure and FunctionTenri FaniÎncă nu există evaluări
- Pattern Recognition in Neural Networks: T. Muthya Mounika, V.V. Vishnu PrabhakarDocument3 paginiPattern Recognition in Neural Networks: T. Muthya Mounika, V.V. Vishnu Prabhakarmaneesh sÎncă nu există evaluări
- Whitney Mclaughlin 2019 Ncca PresentationDocument21 paginiWhitney Mclaughlin 2019 Ncca Presentationapi-298976119Încă nu există evaluări
- Bloom Action Verbs PDFDocument1 paginăBloom Action Verbs PDFvino78100% (2)
- Master's in Biomedical Sciences ChecklistDocument3 paginiMaster's in Biomedical Sciences ChecklistMarcelo SantosÎncă nu există evaluări
- Selection: Suzaine Polancos Zaira Mae RafalDocument6 paginiSelection: Suzaine Polancos Zaira Mae RafalMarlene AgcaoiliÎncă nu există evaluări
- Brown PDFDocument20 paginiBrown PDFccareemail100% (1)
- Guidance Approach For The Encouraging Classroom 6th Edition Dan Gartrell Test BankDocument3 paginiGuidance Approach For The Encouraging Classroom 6th Edition Dan Gartrell Test Banka878027987Încă nu există evaluări
- MicroTAS 2012 PresentationDocument19 paginiMicroTAS 2012 PresentationJan KrajniakÎncă nu există evaluări
- Reflection 2 - Blake Academy and The Green Arrow - Scott NannenDocument2 paginiReflection 2 - Blake Academy and The Green Arrow - Scott Nannenapi-366876366Încă nu există evaluări
- Scared YouthDocument2 paginiScared Youthnarcis2009Încă nu există evaluări
- Stop CrammingDocument6 paginiStop CrammingCharmaine AlipayoÎncă nu există evaluări
- Person Centered TherapyDocument16 paginiPerson Centered TherapyAldrinBalitaÎncă nu există evaluări
- Far Journeys Robert Monroe PDF en EspaolDocument2 paginiFar Journeys Robert Monroe PDF en EspaolAndrew100% (1)
- (NLP For Education) Richard Bandler - Kate Benson - Teaching Excellence - The Definitive Guide To NLP For Teaching and Learning-New Thinking Publications (2018) PDFDocument433 pagini(NLP For Education) Richard Bandler - Kate Benson - Teaching Excellence - The Definitive Guide To NLP For Teaching and Learning-New Thinking Publications (2018) PDFmuveszszi100% (20)
- Psilocybin For Depression and Anxiety Associated With Life-Threatening IllnessesDocument2 paginiPsilocybin For Depression and Anxiety Associated With Life-Threatening IllnessesJosé Carlos Solís SuárezÎncă nu există evaluări
- Stafford y Colom (2013) - Purpose and of Psychoeducation Inpatients With Bipolar Disorder in A Bipolar ClinicsettingDocument9 paginiStafford y Colom (2013) - Purpose and of Psychoeducation Inpatients With Bipolar Disorder in A Bipolar ClinicsettingAbrahán OrellanaÎncă nu există evaluări
- Leadership Roles and Management Functions in Nursing Theory and Application Marquis 7th Edition Test BankDocument6 paginiLeadership Roles and Management Functions in Nursing Theory and Application Marquis 7th Edition Test BankAmanda Wise100% (31)
- Soal Penyisihan KMNR 10 Kelas 1-2Document12 paginiSoal Penyisihan KMNR 10 Kelas 1-2Hari Kurniawan0% (1)
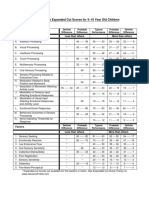
- Sensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenDocument1 paginăSensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenAyra MagpiliÎncă nu există evaluări
- CT I MRI Tumora MozgaDocument126 paginiCT I MRI Tumora MozgaElvir MalicevicÎncă nu există evaluări
- Dahraan Mental Hospital Marka Mental Health CareDocument8 paginiDahraan Mental Hospital Marka Mental Health CareJossephÎncă nu există evaluări
- The Intelligence Trap - David RobsonDocument312 paginiThe Intelligence Trap - David RobsonmichealangeloÎncă nu există evaluări
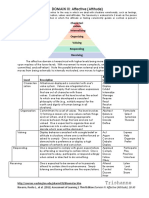
- Trishanne: DOMAIN III: Affective (Attitude)Document2 paginiTrishanne: DOMAIN III: Affective (Attitude)ᜆ᜔ᜇᜒᜐ᜔ᜑ᜔ ᜀᜈ᜔Încă nu există evaluări