S-ar putea să vă placă și
- Hernia: Inguinal - Surgical Anatomy, Presentation, Treatment, ComplicationsDocument43 paginiHernia: Inguinal - Surgical Anatomy, Presentation, Treatment, ComplicationsFobin VargheseÎncă nu există evaluări
- Food Poisoning-Elim Gluten-Elim The Effects of Gluten (Lectins) Eliminate Cause of High HCLDocument10 paginiFood Poisoning-Elim Gluten-Elim The Effects of Gluten (Lectins) Eliminate Cause of High HCLNavin Ramroop100% (2)
- 3-Inguinal Canal PDFDocument58 pagini3-Inguinal Canal PDFN A0% (1)
- Abdomen - IntroductionDocument63 paginiAbdomen - IntroductionPriyanka SharmaÎncă nu există evaluări
- UW Notes - 9 - Gastero-Intestinal ArrangedDocument61 paginiUW Notes - 9 - Gastero-Intestinal ArrangedMohammed SadoonÎncă nu există evaluări
- Colorectal MalignancyDocument108 paginiColorectal MalignancySatishht SatishÎncă nu există evaluări
- Nursing Care Plan - ConstipationDocument2 paginiNursing Care Plan - Constipationderic87% (71)
- Anterior Abdominal Wall Lecture - Nov2015Document75 paginiAnterior Abdominal Wall Lecture - Nov2015Nithin0% (1)
- Abdominal WallDocument75 paginiAbdominal WallJojo RyelciusÎncă nu există evaluări
- 2019 Hernia Kuliah FKDocument50 pagini2019 Hernia Kuliah FKKhairani NurhamidahÎncă nu există evaluări
- (HANDOUT) Phar 112 Lab - Fecalysis and Fecal Occult Blood TestDocument2 pagini(HANDOUT) Phar 112 Lab - Fecalysis and Fecal Occult Blood TestHan SoloÎncă nu există evaluări
- Nursing Care Plan Hirschsprung's Disease (Congenital A Ganglionic Mega Colon)Document2 paginiNursing Care Plan Hirschsprung's Disease (Congenital A Ganglionic Mega Colon)deric87% (30)
- Colostomy ClassDocument24 paginiColostomy Classshahulkp100% (1)
- 03 Anal & Perianal DisordersDocument56 pagini03 Anal & Perianal DisordersHafizah HoshniÎncă nu există evaluări
- Chapter 34 - Assessment of Digestive and Gastrointestinal FunctionDocument3 paginiChapter 34 - Assessment of Digestive and Gastrointestinal FunctionMichael Boado100% (1)
- Nursing Diagnosis For Intestinal ObstructionDocument2 paginiNursing Diagnosis For Intestinal ObstructionYoga Mesi58% (19)
- Dissection Abd WallDocument59 paginiDissection Abd WallTom TsouÎncă nu există evaluări
- Anatomy of PeritoneumDocument61 paginiAnatomy of PeritoneumFirdaus SeptiawanÎncă nu există evaluări
- Enema Administration ChecklistDocument4 paginiEnema Administration ChecklistChelleyOllitro100% (1)
- Large Intestine PIMSR-Dr - Gosai 2022Document40 paginiLarge Intestine PIMSR-Dr - Gosai 2022Dr.B.B.GosaiÎncă nu există evaluări
- Anal CanalDocument59 paginiAnal CanalLulu ShukkoorÎncă nu există evaluări
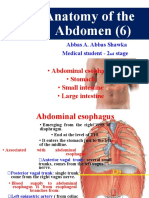
- Anatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineDocument34 paginiAnatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineBilal YimamÎncă nu există evaluări
- Abdominal CavityDocument78 paginiAbdominal Cavitytanishapatel1005Încă nu există evaluări
- A No RectalDocument34 paginiA No RectalSyarafina AzmanÎncă nu există evaluări
- GIT Cont 071628Document51 paginiGIT Cont 071628Olatomide OlaniranÎncă nu există evaluări
- General AnatomyDocument46 paginiGeneral AnatomyIhab IsmailÎncă nu există evaluări
- Peritoneum, Peritoneal Cavity, and Diaphragm 11-6-15-1Document67 paginiPeritoneum, Peritoneal Cavity, and Diaphragm 11-6-15-1Deny ShajiniÎncă nu există evaluări
- Hernia FTDDocument71 paginiHernia FTDEmmanuel Papa AcquahÎncă nu există evaluări
- Urinary Bladder, Rectum and Anal CanalDocument34 paginiUrinary Bladder, Rectum and Anal CanalIbe ClementÎncă nu există evaluări
- Hernia SanaDocument57 paginiHernia SanaBurhanuddin BhindarwalaÎncă nu există evaluări
- External & Internal Generative Organs OrgansDocument78 paginiExternal & Internal Generative Organs OrgansdeevoncÎncă nu există evaluări
- Dinding Abdomen PSIKDocument79 paginiDinding Abdomen PSIKSondang DamanikÎncă nu există evaluări
- 1 Abdominal VisceraDocument45 pagini1 Abdominal VisceraMero HamedÎncă nu există evaluări
- ANAT 221 - PeritoneumDocument22 paginiANAT 221 - PeritoneumWisdom IkechukwuÎncă nu există evaluări
- Ana SGD 15Document67 paginiAna SGD 15Bea ManzanoÎncă nu există evaluări
- Anat 221-Large IntestineDocument21 paginiAnat 221-Large IntestineWisdom IkechukwuÎncă nu există evaluări
- Inguinal Hernias: Trix M. Asuncion M.D. General SurgeryDocument55 paginiInguinal Hernias: Trix M. Asuncion M.D. General Surgeryjitendra magarÎncă nu există evaluări
- Anatomy of Lower Gastrointestinal TractDocument26 paginiAnatomy of Lower Gastrointestinal TractOmar Ali AyoubkhanÎncă nu există evaluări
- Anatomy of The EsophagusDocument14 paginiAnatomy of The EsophagusroselynroukayaÎncă nu există evaluări
- Anatomy of GIT For PCII Students..Document106 paginiAnatomy of GIT For PCII Students..AMANUEL HABTEWOLDÎncă nu există evaluări
- Sahitya Snigdha (Hernia Module)Document159 paginiSahitya Snigdha (Hernia Module)h9pkyd9dg9Încă nu există evaluări
- Large IntestineDocument29 paginiLarge IntestineOlaifa victorÎncă nu există evaluări
- 7) Anatomy of OMENTUMDocument22 pagini7) Anatomy of OMENTUMGoodone OneÎncă nu există evaluări
- The Large IntestineDocument34 paginiThe Large IntestineSastiy MutiadesieÎncă nu există evaluări
- Abdominal AnatomyDocument17 paginiAbdominal AnatomyAbdu NaviÎncă nu există evaluări
- Inguinal Canal: DR - Lubna NazliDocument28 paginiInguinal Canal: DR - Lubna NazliAhmed AminÎncă nu există evaluări
- Surgical Anatomy of PeritoneumDocument63 paginiSurgical Anatomy of PeritoneumSuvarna RajÎncă nu există evaluări
- StomachDocument29 paginiStomachSupriti Verma Bhatnagar100% (1)
- RectumDocument43 paginiRectummidhunramesh007100% (4)
- Maternal Anatomy External and Internal Generative OrgansDocument84 paginiMaternal Anatomy External and Internal Generative OrgansChristine HoÎncă nu există evaluări
- Duodenum and PancreaslectureDocument35 paginiDuodenum and PancreaslectureChigozie GeraldÎncă nu există evaluări
- Anatomy of The AbdomenDocument107 paginiAnatomy of The AbdomenmichaelhossianÎncă nu există evaluări
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreDocument28 paginiOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreabctutorÎncă nu există evaluări
- Abdominal SymptomsDocument21 paginiAbdominal SymptomsKiara GovenderÎncă nu există evaluări
- Abdomen - Esophagus To ColonDocument42 paginiAbdomen - Esophagus To ColonBibek GajmerÎncă nu există evaluări
- Anatomy of The Abdomen: Samara University Biomedical Sciences DepartmentDocument142 paginiAnatomy of The Abdomen: Samara University Biomedical Sciences Departmentfentaw melkieÎncă nu există evaluări
- Hernia Scrotalis FIxDocument56 paginiHernia Scrotalis FIxivaniÎncă nu există evaluări
- Abdomen AnatomyDocument9 paginiAbdomen AnatomyPhan Hoàng SơnÎncă nu există evaluări
- Colon, Caecum & Appendix 2017Document67 paginiColon, Caecum & Appendix 2017yasrul izad0% (1)
- GasterDocument179 paginiGasterAraka Patriota100% (1)
- Anatomi Gaster Dan DuodenumDocument179 paginiAnatomi Gaster Dan DuodenumHaraka NabdaÎncă nu există evaluări
- HERNIADocument70 paginiHERNIAmwro789000Încă nu există evaluări
- Abdominal-Cavity TransDocument23 paginiAbdominal-Cavity TransMigz BolivarÎncă nu există evaluări
- Surgical-ANATOMY OF Anterior Abdominal WallDocument83 paginiSurgical-ANATOMY OF Anterior Abdominal WallSyed Irfan ArifÎncă nu există evaluări
- Repaso 5 ANATOMY JEJUNUM LJ ILEUM L0 COLONDocument4 paginiRepaso 5 ANATOMY JEJUNUM LJ ILEUM L0 COLONAngelitza AlmodóvarÎncă nu există evaluări
- Acd 13 PDFDocument62 paginiAcd 13 PDFIgor AnsoffÎncă nu există evaluări
- HerniaDocument106 paginiHerniaDr-Mohammad Ali-Fayiz Al TamimiÎncă nu există evaluări
- A Homeopathic Approach To Inflammatory Bowel Disease (Crohn's and Colitis)Document7 paginiA Homeopathic Approach To Inflammatory Bowel Disease (Crohn's and Colitis)Saad MasoodÎncă nu există evaluări
- Drug Used in ConstipationDocument14 paginiDrug Used in ConstipationSuraj VermaÎncă nu există evaluări
- Acupuncture Points Parents Can Use To Help KidsDocument1 paginăAcupuncture Points Parents Can Use To Help KidsBishara WilsonÎncă nu există evaluări
- Fleet Enema Instructions 2020 04 14Document1 paginăFleet Enema Instructions 2020 04 14CalebAHardinÎncă nu există evaluări
- GI-GU Exam 4 Fall 2020Document1 paginăGI-GU Exam 4 Fall 2020AnnissaLarnardÎncă nu există evaluări
- Vonoprazan 10 MG DailyDocument5 paginiVonoprazan 10 MG DailySanjay NavaleÎncă nu există evaluări
- Askep HisprungDocument25 paginiAskep HisprungRika AmaliyaÎncă nu există evaluări
- Ileus MeconiumDocument27 paginiIleus MeconiumDebby TamaraÎncă nu există evaluări
- Case Presentation BashaDocument24 paginiCase Presentation Bashakhaderbasha2020Încă nu există evaluări
- Cattell ManeuverDocument1 paginăCattell ManeuvermahmoudÎncă nu există evaluări
- Welcome To TampcolDocument5 paginiWelcome To TampcolmurugangdÎncă nu există evaluări
- Coffee-Bean SignDocument1 paginăCoffee-Bean Signjudin_oÎncă nu există evaluări
- No Jenis Keterangan 1. Air Under The Diaphragm: Nama: Adilah Zatil Kurnia Rahma AfifahDocument6 paginiNo Jenis Keterangan 1. Air Under The Diaphragm: Nama: Adilah Zatil Kurnia Rahma AfifahMona Indah PutrianiÎncă nu există evaluări
- Teaching Plan For DiarrheaDocument2 paginiTeaching Plan For DiarrheaSheila Nones50% (6)
- Pig Anatomy PosterDocument1 paginăPig Anatomy PosterBrandon Alexis Calderón AvellanedaÎncă nu există evaluări
- Bowel Function AnatomyDocument3 paginiBowel Function AnatomyseksÎncă nu există evaluări
- Novilyn C. Pataray BSN - Ii: Assessment Diagnosi S Pathophysiolog Y Planning Intervention Rationale EvaluationDocument2 paginiNovilyn C. Pataray BSN - Ii: Assessment Diagnosi S Pathophysiolog Y Planning Intervention Rationale EvaluationCharina AubreyÎncă nu există evaluări
- Digestive System 3 HistologyDocument29 paginiDigestive System 3 HistologyshmirtbÎncă nu există evaluări
- 02 DyspepsiaDocument42 pagini02 Dyspepsiaacatrinei_daniela_2Încă nu există evaluări
- My Small and Large Intestines: © Teacher Created Resources, Inc. #211 My BodyDocument3 paginiMy Small and Large Intestines: © Teacher Created Resources, Inc. #211 My Bodyalana reneÎncă nu există evaluări
- Dr. Octaviana Dewi Ayu Puspita: Hari/ Tanggal Nama Pasien JK Umur Diagnosis KeteranganDocument4 paginiDr. Octaviana Dewi Ayu Puspita: Hari/ Tanggal Nama Pasien JK Umur Diagnosis KeteranganDaniel HoseaÎncă nu există evaluări
- ILA - Hirschsprungs DiseaseDocument48 paginiILA - Hirschsprungs DiseaseSoleh Ramly100% (1)