S-ar putea să vă placă și
- Nursing Diagnosis Impaired Gas ExchangeDocument7 paginiNursing Diagnosis Impaired Gas ExchangeZycon Rodney Ae'zecquel Gachallan50% (2)
- Clinicians To Pediatric Sleep Disorders 2007Document370 paginiClinicians To Pediatric Sleep Disorders 2007Mihaela MuscaluÎncă nu există evaluări
- Anaesthesia in Obese PatientsDocument72 paginiAnaesthesia in Obese PatientsPraveen RamasamyÎncă nu există evaluări
- Apnea Report Reveals Moderate Sleep DisorderDocument2 paginiApnea Report Reveals Moderate Sleep DisordergopuÎncă nu există evaluări
- AASM Scoring Manual Version 2.4 Berry Et Al. 2017Document89 paginiAASM Scoring Manual Version 2.4 Berry Et Al. 2017Jorge Borrani100% (4)
- Myofunctional TherapyDocument19 paginiMyofunctional Therapy許越隆Încă nu există evaluări
- Paediatric Chest RadiologyDocument120 paginiPaediatric Chest Radiologysunielgoel100% (6)
- What is BronchoscopyDocument19 paginiWhat is BronchoscopyMARIANN JEAN ANDREA CULANAG MATALINESÎncă nu există evaluări
- Obesity & Anaesthesia: Co-Ordinator - Dr. Chavi Sethi (MD) Speaker - Dr. Uday Pratap SinghDocument56 paginiObesity & Anaesthesia: Co-Ordinator - Dr. Chavi Sethi (MD) Speaker - Dr. Uday Pratap SinghRafi ramdhanÎncă nu există evaluări
- 4-Anesthesia and Obese PatientsDocument83 pagini4-Anesthesia and Obese PatientsMateen ShukriÎncă nu există evaluări
- Adult Client with Respiratory DisordersDocument101 paginiAdult Client with Respiratory DisordersNicholas TagleÎncă nu există evaluări
- Checklist For Evaluation of Potential Airway & Breathing DisordersDocument7 paginiChecklist For Evaluation of Potential Airway & Breathing DisordersSaran BÎncă nu există evaluări
- Sleep With ButeykoDocument130 paginiSleep With ButeykoDamir100% (2)
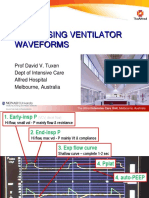
- Ventilator Waveforms DavidTuxen2Document41 paginiVentilator Waveforms DavidTuxen2Syed Shahrul Naz Syed100% (1)
- Nursing Care Plan For Pleural EffusionDocument9 paginiNursing Care Plan For Pleural EffusionJoseph Angelo Fortuna Carmona100% (1)
- Management of COPD: Causes, Symptoms, TreatmentDocument47 paginiManagement of COPD: Causes, Symptoms, TreatmentMegha VadanereÎncă nu există evaluări
- PneumothoraxDocument52 paginiPneumothoraxtrisna satrianaÎncă nu există evaluări
- Pleural Effusion: Presented By:-Gayathri Gopakumar BSC - Nursing 2 YearDocument30 paginiPleural Effusion: Presented By:-Gayathri Gopakumar BSC - Nursing 2 YearGAYATHRI GOPAKUMARÎncă nu există evaluări
- Sleep DisordersDocument19 paginiSleep DisordersKaren MogiÎncă nu există evaluări
- 13.acute Respiratory FailureDocument34 pagini13.acute Respiratory Failurekarim hassan100% (1)
- The Obese Patient. F o RDocument22 paginiThe Obese Patient. F o RsukolratingÎncă nu există evaluări
- Obesity and AnaesthesiaDocument7 paginiObesity and AnaesthesiaRuwan KuruppuÎncă nu există evaluări
- Anesthesia and ObesityDocument39 paginiAnesthesia and ObesityLucille IlaganÎncă nu există evaluări
- Cardiovascular System: Complications of Positive Pressure VentilationDocument5 paginiCardiovascular System: Complications of Positive Pressure VentilationjefrocÎncă nu există evaluări
- ANESTHESIA For OTLARYNGOLOGIC SurgeryDocument64 paginiANESTHESIA For OTLARYNGOLOGIC SurgeryKelvin TuazonÎncă nu există evaluări
- Anaesthesia For Obese Patients: Dr. Thomas Specialist in Anaesthesia, Al Bukariya General HospitalDocument38 paginiAnaesthesia For Obese Patients: Dr. Thomas Specialist in Anaesthesia, Al Bukariya General HospitalAnastesiologi CÎncă nu există evaluări
- Respiratory Distress SyndromeDocument41 paginiRespiratory Distress Syndromef.abrahamÎncă nu există evaluări
- Week 5 Respiratory EmergencyDocument61 paginiWeek 5 Respiratory EmergencyArmand Bong SantiagoÎncă nu există evaluări
- Respiratory Diseases GuideDocument58 paginiRespiratory Diseases GuideSarahÎncă nu există evaluări
- Sleep ApneuDocument22 paginiSleep ApneuAnonymous 8Jlc7aTs90Încă nu există evaluări
- CPPT IN THE ICUDocument39 paginiCPPT IN THE ICUeyob kaseyeÎncă nu există evaluări
- Lung Expansion RevisionDocument89 paginiLung Expansion RevisionPatrick RoqueÎncă nu există evaluări
- CPAP SlidesDocument52 paginiCPAP SlidesAnusha Verghese100% (1)
- Sleep Apnea and Diabetes RelationshipDocument28 paginiSleep Apnea and Diabetes RelationshipSumit PuloriaÎncă nu există evaluări
- Neonatal AnaesthesiaDocument61 paginiNeonatal AnaesthesianeneknoraÎncă nu există evaluări
- Bariatric Surgery Part 2Document89 paginiBariatric Surgery Part 2Hossam atefÎncă nu există evaluări
- Prezentare Caz Clinic Ventilatia Mecanica IntraoperatorieDocument55 paginiPrezentare Caz Clinic Ventilatia Mecanica Intraoperatorieralucaioana89Încă nu există evaluări
- Sleep ApneaDocument23 paginiSleep Apneahams100% (1)
- Obesity 2Document12 paginiObesity 2Siva SankarÎncă nu există evaluări
- Hypoxemia in ICU: Prepared by Hadi JazanDocument41 paginiHypoxemia in ICU: Prepared by Hadi JazanHadi JazanÎncă nu există evaluări
- Airway ManagementDocument30 paginiAirway ManagementFuad TalÎncă nu există evaluări
- Resuscitation in PregnancyDocument24 paginiResuscitation in PregnancyHassan Al SinanÎncă nu există evaluări
- Chest Physiotherapy With Sputum CollectionDocument41 paginiChest Physiotherapy With Sputum CollectionEduardÎncă nu există evaluări
- Women's Pneumonia ReportDocument9 paginiWomen's Pneumonia ReportNohaira SADANGÎncă nu există evaluări
- Asthma v1Document27 paginiAsthma v1Asiya FaizyÎncă nu există evaluări
- Respiratory Disease and AnaesthesiaDocument8 paginiRespiratory Disease and AnaesthesiaReddyÎncă nu există evaluări
- Anesthesia For Esophageal SurgeriesDocument33 paginiAnesthesia For Esophageal SurgeriesKavyasree KatamÎncă nu există evaluări
- Advance Clinical Nursing Presentation - SusanDocument40 paginiAdvance Clinical Nursing Presentation - SusanAbdul Hamid Al FarsiÎncă nu există evaluări
- Sleep Medicine: Devi Farida UtamiDocument105 paginiSleep Medicine: Devi Farida UtamimufiÎncă nu există evaluări
- Pulmonary Vascular Disorders and Respiratory FailureDocument5 paginiPulmonary Vascular Disorders and Respiratory FailureTrishia GuillermoÎncă nu există evaluări
- Respiratory Assessment and Treatments: Presented by ATOP Clinical StaffDocument39 paginiRespiratory Assessment and Treatments: Presented by ATOP Clinical StaffNoralyn AsgariÎncă nu există evaluări
- Chapter 16: Ready For ReviewDocument5 paginiChapter 16: Ready For Reviewsamfarmer333Încă nu există evaluări
- Post Intubation HypotensionDocument37 paginiPost Intubation Hypotensionfifa_0304535100% (1)
- Obstructive Sleep Apnea: SS Visser Lung Unit Pah and UpDocument23 paginiObstructive Sleep Apnea: SS Visser Lung Unit Pah and UpMuhammad NuruddinÎncă nu există evaluări
- COPD Treatment and Dental CareDocument42 paginiCOPD Treatment and Dental CareAnoos rabayarabayaÎncă nu există evaluări
- Osa DR S S FazalDocument92 paginiOsa DR S S FazalAparup SaluiÎncă nu există evaluări
- Pneumothorax: DR G.B.L Samarasekera Consultant Respiratory Physician DGH - GampahaDocument50 paginiPneumothorax: DR G.B.L Samarasekera Consultant Respiratory Physician DGH - GampahappgpcsÎncă nu există evaluări
- Pedia Concepts 2:: From Respiratory Problems To HematologicDocument119 paginiPedia Concepts 2:: From Respiratory Problems To HematologicarudarbmeeÎncă nu există evaluări
- Pedi 2Document25 paginiPedi 2Roba AÎncă nu există evaluări
- Dr. Irbab HawariDocument25 paginiDr. Irbab HawariirbabhmdÎncă nu există evaluări
- Pedi AnesthesiaDocument39 paginiPedi Anesthesiahailemichael chekolÎncă nu există evaluări
- Anesthetic Considerations in Esophageal SurgeriesDocument40 paginiAnesthetic Considerations in Esophageal SurgeriesKavyasree KatamÎncă nu există evaluări
- 19 Respiratory Renal and Hepatic Disease and AnaesthesiaDocument0 pagini19 Respiratory Renal and Hepatic Disease and AnaesthesiajuniorebindaÎncă nu există evaluări
- Procedural AnesthesiaDocument40 paginiProcedural AnesthesiaJovian LutfiÎncă nu există evaluări
- Anaesthetic Management of Obese PatientDocument53 paginiAnaesthetic Management of Obese PatientpriyadikkalaÎncă nu există evaluări
- Acute Respiratory Distress SyndromeDocument26 paginiAcute Respiratory Distress Syndromethea waaniÎncă nu există evaluări
- Consider Abdominal Compartment Syndrome in Patients With Refractory HypotensionDocument26 paginiConsider Abdominal Compartment Syndrome in Patients With Refractory HypotensionHari AdityonugrohoÎncă nu există evaluări
- 2010 Philips Respironics CatalogDocument148 pagini2010 Philips Respironics CatalogAcilegna BÎncă nu există evaluări
- Sleep-Wake DisordersDocument4 paginiSleep-Wake DisordersJohn PagangpangÎncă nu există evaluări
- Modafinil Factsheet (Composite)Document21 paginiModafinil Factsheet (Composite)Danilo ScodellaroÎncă nu există evaluări
- Read The NJT ReportDocument69 paginiRead The NJT ReportNewsdayÎncă nu există evaluări
- Signs and Symptoms of Obstructive Sleep Apnea and Upper Airway Resistance SyndromeDocument7 paginiSigns and Symptoms of Obstructive Sleep Apnea and Upper Airway Resistance SyndromeLuis De jesus SolanoÎncă nu există evaluări
- 1 s2.0 S2213177917304183 MainDocument9 pagini1 s2.0 S2213177917304183 MainAndré DiasÎncă nu există evaluări
- Manual Dream StarDocument92 paginiManual Dream StarDanut Dan100% (1)
- FDA Approved ListDocument25 paginiFDA Approved ListAli UnitedHospitalÎncă nu există evaluări
- Obstructive Sleep Apnea and Orthodontics: An American Association of Orthodontists White PaperDocument17 paginiObstructive Sleep Apnea and Orthodontics: An American Association of Orthodontists White PaperIsa TorresÎncă nu există evaluări
- Obstructive Sleep ApneaDocument49 paginiObstructive Sleep ApnearuthÎncă nu există evaluări
- By: Reashnaa A/P Loganathan Yunisa Meutia Putri Zahra Fitrianti Preseptor: R.M. Haryadi Karyono, DR., SPKJDocument51 paginiBy: Reashnaa A/P Loganathan Yunisa Meutia Putri Zahra Fitrianti Preseptor: R.M. Haryadi Karyono, DR., SPKJmeutiaputripuyÎncă nu există evaluări
- Sleep Disorders in Myopathy 3.10.19Document16 paginiSleep Disorders in Myopathy 3.10.19Nitesh DahiyaÎncă nu există evaluări
- STOP QuestionnaireDocument10 paginiSTOP Questionnaire旭達數位牙科培訓中心Încă nu există evaluări
- PrintDocument65 paginiPrintLý TưởngÎncă nu există evaluări
- Sleep CPGDocument54 paginiSleep CPGbonn maÎncă nu există evaluări
- Ambu Sleepmate Poster PDFDocument1 paginăAmbu Sleepmate Poster PDFMinh Triết LêÎncă nu există evaluări
- OSADocument5 paginiOSAtherese BÎncă nu există evaluări
- 2010 Philips Respironics CatalogDocument146 pagini2010 Philips Respironics CatalogRoynaldo HutabaratÎncă nu există evaluări
- Respironics Dreamstation CpapDocument12 paginiRespironics Dreamstation CpapLowtech23Încă nu există evaluări
- Association Between Breathing Route, Oxygen Desaturation, and Upper Airway MorphologyDocument6 paginiAssociation Between Breathing Route, Oxygen Desaturation, and Upper Airway MorphologyMark Burhenne DDSÎncă nu există evaluări
- Obstructive Sleep Apnea Syndromes: Definitions, Epidemiology, Diagnosis, and VariantsDocument25 paginiObstructive Sleep Apnea Syndromes: Definitions, Epidemiology, Diagnosis, and VariantsnatalieÎncă nu există evaluări
- 10.1007@s11325 012 0746 7Document8 pagini10.1007@s11325 012 0746 7GissellePantojaÎncă nu există evaluări