S-ar putea să vă placă și
- TriglyceridesDocument1 paginăTriglyceridesDinesh SreedharanÎncă nu există evaluări
- Total ProteinDocument1 paginăTotal ProteinDinesh SreedharanÎncă nu există evaluări
- GlycoDocument1 paginăGlycoDinesh SreedharanÎncă nu există evaluări
- (Modified Jaffe's Kinetic Method & End Point Method) For The Determination of Creatinine in Serum and Urine (For in Vitro Diagnostic Use Only)Document1 pagină(Modified Jaffe's Kinetic Method & End Point Method) For The Determination of Creatinine in Serum and Urine (For in Vitro Diagnostic Use Only)Dinesh SreedharanÎncă nu există evaluări
- Microalbumin Turbilatex - Liquid CalibratorDocument2 paginiMicroalbumin Turbilatex - Liquid CalibratorDinesh SreedharanÎncă nu există evaluări
- Chloride Mono VialDocument2 paginiChloride Mono VialDinesh SreedharanÎncă nu există evaluări
- RF LatexDocument1 paginăRF LatexDinesh SreedharanÎncă nu există evaluări
- (Mod. IFCC Method) For The Determination of SGPT (ALT) Activity in Serum. (For in Vitro Diagnostic Use Only)Document1 pagină(Mod. IFCC Method) For The Determination of SGPT (ALT) Activity in Serum. (For in Vitro Diagnostic Use Only)Dinesh SreedharanÎncă nu există evaluări
- (Mod. IFCC Method) For The Determination of SGOT (AST) Activity in Serum. (For in Vitro Diagnostic Use Only)Document1 pagină(Mod. IFCC Method) For The Determination of SGOT (AST) Activity in Serum. (For in Vitro Diagnostic Use Only)Dinesh SreedharanÎncă nu există evaluări
- Lipase: Calib. Conc. Check Vial LabelDocument2 paginiLipase: Calib. Conc. Check Vial LabelDinesh SreedharanÎncă nu există evaluări
- Cholesterol & HDL CholesterolDocument1 paginăCholesterol & HDL CholesterolDinesh SreedharanÎncă nu există evaluări
- GlucoseDocument1 paginăGlucoseDinesh SreedharanÎncă nu există evaluări
- BilirubinDocument1 paginăBilirubinDinesh SreedharanÎncă nu există evaluări
- CalciumDocument1 paginăCalciumDinesh SreedharanÎncă nu există evaluări
- Uric Acid KitDocument2 paginiUric Acid KitDinesh SreedharanÎncă nu există evaluări
- Urea Berthelot KitDocument2 paginiUrea Berthelot KitDinesh SreedharanÎncă nu există evaluări
- Urea Kinetic KitDocument2 paginiUrea Kinetic KitDinesh SreedharanÎncă nu există evaluări
- AlbuminDocument1 paginăAlbuminDinesh SreedharanÎncă nu există evaluări
- Tydal S KitDocument2 paginiTydal S KitDinesh SreedharanÎncă nu există evaluări
- Triglycerides (GOP-PAP Method) Test ProcedureDocument3 paginiTriglycerides (GOP-PAP Method) Test ProcedureDinesh SreedharanÎncă nu există evaluări
- SGPTDocument2 paginiSGPTDinesh SreedharanÎncă nu există evaluări
- Total Protein KitDocument2 paginiTotal Protein KitDinesh SreedharanÎncă nu există evaluări
- RF TurbiDocument2 paginiRF TurbiDinesh SreedharanÎncă nu există evaluări
- Tydal Oh KitDocument2 paginiTydal Oh KitDinesh SreedharanÎncă nu există evaluări
- SGOT (AST) Test Kit for Liver & Heart Injury DetectionDocument2 paginiSGOT (AST) Test Kit for Liver & Heart Injury DetectionDinesh Sreedharan0% (1)
- Microalbumin Calibrator Stable for 1 MonthDocument2 paginiMicroalbumin Calibrator Stable for 1 MonthDinesh SreedharanÎncă nu există evaluări
- SODIUMDocument2 paginiSODIUMDinesh SreedharanÎncă nu există evaluări
- RF LatexDocument2 paginiRF LatexDinesh SreedharanÎncă nu există evaluări
- Potassium: 20 Test 1x60mlDocument3 paginiPotassium: 20 Test 1x60mlDinesh SreedharanÎncă nu există evaluări
- Andard (S) and Test (T)Document2 paginiAndard (S) and Test (T)Dinesh SreedharanÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- NIHR Sheffield Clinical Research Facility: Cleaning and Disinfection of The Sample Processing AreaDocument3 paginiNIHR Sheffield Clinical Research Facility: Cleaning and Disinfection of The Sample Processing AreaTanvir SiddikiÎncă nu există evaluări
- Food and Nutrition MCQ CarboDocument6 paginiFood and Nutrition MCQ CarboShivangi Singh0% (2)
- CASE STUDY ON NEWBORN CARE OBSERVATIONDocument8 paginiCASE STUDY ON NEWBORN CARE OBSERVATIONPiyush Dutta100% (1)
- Father-Child Play: A Systematic Review of Its Frequency, T Characteristics and Potential Impact On Children's DevelopmentDocument17 paginiFather-Child Play: A Systematic Review of Its Frequency, T Characteristics and Potential Impact On Children's DevelopmentNiyyah HusseinÎncă nu există evaluări
- Healthy Eating:What Does It Mean To Adolescents?: Esearch RticleDocument10 paginiHealthy Eating:What Does It Mean To Adolescents?: Esearch RticlealifiaÎncă nu există evaluări
- Housekeeping Procedures: Why Should We Pay Attention To Housekeeping at Work?Document4 paginiHousekeeping Procedures: Why Should We Pay Attention To Housekeeping at Work?Selva KumarÎncă nu există evaluări
- Bài Tập Trắc Nghiệm Anh 10- Chương Trình Thí ĐiểmDocument143 paginiBài Tập Trắc Nghiệm Anh 10- Chương Trình Thí ĐiểmPhong ĐâyÎncă nu există evaluări
- Template For Synthesis TallyDocument5 paginiTemplate For Synthesis TallyFloesine De JesusÎncă nu există evaluări
- Depression Among Allied Health StudentsDocument6 paginiDepression Among Allied Health StudentsMatelyn OargaÎncă nu există evaluări
- Stress Management OutlineDocument7 paginiStress Management OutlineJericko Allen Resus100% (1)
- Metacognitive Therapy Hjemdal 2013Document13 paginiMetacognitive Therapy Hjemdal 2013rnuevo2Încă nu există evaluări
- Hubungan Pemberian Obat Terhadap HB, Zat Besi ProteinDocument10 paginiHubungan Pemberian Obat Terhadap HB, Zat Besi ProteinFanny Aulia PratamaÎncă nu există evaluări
- London Sperm Bank FAQsDocument4 paginiLondon Sperm Bank FAQsdickenschuiÎncă nu există evaluări
- Lifestyle Diseases Affecting The Nursing Faculty at Tarlac State University During Covid 19 PandemicDocument19 paginiLifestyle Diseases Affecting The Nursing Faculty at Tarlac State University During Covid 19 PandemicDeinielle Magdangal RomeroÎncă nu există evaluări
- Parkinson's DiseaseDocument3 paginiParkinson's DiseaseRachelle Ann E. De FelixÎncă nu există evaluări
- The Lung Meridian Acu-PointsDocument1 paginăThe Lung Meridian Acu-PointsVicaas VSÎncă nu există evaluări
- 2021 09 02 Motorsport Uk Yearbook 2021Document472 pagini2021 09 02 Motorsport Uk Yearbook 2021Marcello AssunçãoÎncă nu există evaluări
- Martinplus Silo Solutions: Storage Vessel Cleaning Service and ProductsDocument8 paginiMartinplus Silo Solutions: Storage Vessel Cleaning Service and ProductstacosanchezbrayanÎncă nu există evaluări
- Addiction and The BrainDocument53 paginiAddiction and The BrainNational Press Foundation100% (1)
- Introduction To Congestive Heart Failure Diagnosis, Classifications & ManagementDocument50 paginiIntroduction To Congestive Heart Failure Diagnosis, Classifications & Managementmadimadi11Încă nu există evaluări
- LecturePlan AE201 23ECH-102Document5 paginiLecturePlan AE201 23ECH-102Specsy GuyÎncă nu există evaluări
- Examination of Consumption Habits of Fast Food Patrons in SingaporeDocument41 paginiExamination of Consumption Habits of Fast Food Patrons in SingaporeAngeline Leong100% (1)
- BASF Animal Nutrition Balangut Brochure PoultryDocument2 paginiBASF Animal Nutrition Balangut Brochure PoultryVmp VmpÎncă nu există evaluări
- Revision 123 For The Mid - Term - E8Document4 paginiRevision 123 For The Mid - Term - E8hnaoabÎncă nu există evaluări
- Knowledge, Attitude and Practice On Hypertension Among Antihypertensive Medication UsersDocument7 paginiKnowledge, Attitude and Practice On Hypertension Among Antihypertensive Medication UsersMuhammad DeddyÎncă nu există evaluări
- 11 EnglishDocument12 pagini11 EnglishIndrajitÎncă nu există evaluări
- Sneha KalpanaDocument15 paginiSneha KalpanaP V N R PrasadÎncă nu există evaluări
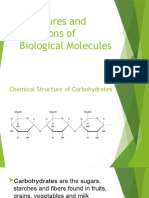
- Carbohydrates Structure Functions Biological MoleculesDocument26 paginiCarbohydrates Structure Functions Biological Moleculesbuena carillaÎncă nu există evaluări
- History of Public HealthDocument23 paginiHistory of Public HealthБакытÎncă nu există evaluări
- NCP On Preterm LaborDocument2 paginiNCP On Preterm Laborinah krizia lagueÎncă nu există evaluări