S-ar putea să vă placă și
- CPH SIM Week 1-3Document23 paginiCPH SIM Week 1-3Vine OrtegaÎncă nu există evaluări
- Maternal and Child Health Nursing 1 Saundrs Pink EdDocument149 paginiMaternal and Child Health Nursing 1 Saundrs Pink EdVin SantosÎncă nu există evaluări
- Situation 1 - Mr. Ibarra Is Assigned To The Triage Area and While On Duty, He Assesses The Condition of Mrs. Simon WhoDocument52 paginiSituation 1 - Mr. Ibarra Is Assigned To The Triage Area and While On Duty, He Assesses The Condition of Mrs. Simon Whogerald_ichigoÎncă nu există evaluări
- CHN PRELIM Quiz 1 (2011)Document5 paginiCHN PRELIM Quiz 1 (2011)Amiel Francisco ReyesÎncă nu există evaluări
- Bemonc FlowchartDocument1 paginăBemonc FlowchartReg LagartejaÎncă nu există evaluări
- Care of Clients With Problem in Oxygenation Quiz 3Document5 paginiCare of Clients With Problem in Oxygenation Quiz 3marsan12Încă nu există evaluări
- Community Health NursingDocument5 paginiCommunity Health NursingAmy Canonizado ViniegasÎncă nu există evaluări
- What Is Disaster ManagementDocument1 paginăWhat Is Disaster Managementarvidkumar87060Încă nu există evaluări
- Medical Surgical Nursing:Geniro Urinary Tract Disorder.Document415 paginiMedical Surgical Nursing:Geniro Urinary Tract Disorder.Minlik-alew Dejenie100% (3)
- Port Health - OverviewDocument30 paginiPort Health - OverviewKay BristolÎncă nu există evaluări
- NCM110 Midterm ExamDocument19 paginiNCM110 Midterm ExamJustin John NavarroÎncă nu există evaluări
- University of Perpetual Help System DALTA: College of Radiologic TechnologyDocument2 paginiUniversity of Perpetual Help System DALTA: College of Radiologic TechnologyJynrose Kaye GulpanyÎncă nu există evaluări
- Week Date Topic/s Learning Activities and Strategies AssessmentDocument5 paginiWeek Date Topic/s Learning Activities and Strategies Assessmentkristine bernafaye damokingÎncă nu există evaluări
- Febrile SeizuresDocument18 paginiFebrile Seizureskara_korum100% (1)
- CHN Final TopicsDocument52 paginiCHN Final TopicsMary Ann SacramentoÎncă nu există evaluări
- Ecology: of The Disease or Dynamic of Disease Transmission Chapter TwoDocument42 paginiEcology: of The Disease or Dynamic of Disease Transmission Chapter TwoCabdi WaliÎncă nu există evaluări
- Infectious DiseasesDocument10 paginiInfectious DiseasesAgnes Marie RendonÎncă nu există evaluări
- Questions in HRDP-COPAR LectureDocument2 paginiQuestions in HRDP-COPAR LectureEugene RexÎncă nu există evaluări
- Vital Statistic PHC 2 Joy 1Document19 paginiVital Statistic PHC 2 Joy 1claudetteÎncă nu există evaluări
- Sample QuestionnaireDocument10 paginiSample QuestionnaireJess Fernandez BorgaÎncă nu există evaluări
- Case Presentation 9Document51 paginiCase Presentation 9Evelyn MedinaÎncă nu există evaluări
- NCM 112 EvalDocument16 paginiNCM 112 EvalMartin T ManuelÎncă nu există evaluări
- AMOEBIASISDocument8 paginiAMOEBIASISCheska ت HortelanoÎncă nu există evaluări
- BAJADO, Allyssa Mae D. Microbiology 1Document25 paginiBAJADO, Allyssa Mae D. Microbiology 1Hernandez SakuraÎncă nu există evaluări
- H.E CHAPTER 2 Historical Development and Concepts of Health 1Document35 paginiH.E CHAPTER 2 Historical Development and Concepts of Health 1Gumama AmeiyrhaÎncă nu există evaluări
- RESPIRATORY SYSTEM Nclex Iloilo 4Document27 paginiRESPIRATORY SYSTEM Nclex Iloilo 4Barangay Centro SurÎncă nu există evaluări
- Quiz 9Document189 paginiQuiz 9Joshua PayneÎncă nu există evaluări
- Community Health Nursing ExamsDocument13 paginiCommunity Health Nursing ExamsAhrisJeannine EscuadroÎncă nu există evaluări
- PediaDocument6 paginiPediaエニエルカム オレーバンÎncă nu există evaluări
- Foundations of Community and Public HealthDocument38 paginiFoundations of Community and Public HealthSim QuiambaoÎncă nu există evaluări
- Zollinger EllisonDocument2 paginiZollinger EllisonFrama Intan MiguelÎncă nu există evaluări
- PHC2. The Philippine Health Care Delivery SystemDocument55 paginiPHC2. The Philippine Health Care Delivery SystemHumilyn NgayawonÎncă nu există evaluări
- Asthma Quiz 2Document58 paginiAsthma Quiz 2Swati SharmaÎncă nu există evaluări
- Health Statistics and EpidemiologyDocument44 paginiHealth Statistics and EpidemiologyAhmad BaolayyanÎncă nu există evaluări
- All Questions With AnswersDocument940 paginiAll Questions With AnswersMaria Hernandez Martinez75% (4)
- The Expanded Program On Immunization LectureDocument99 paginiThe Expanded Program On Immunization LectureMichael JoaquinÎncă nu există evaluări
- HANDWASHINGDocument15 paginiHANDWASHINGNis DimagibaÎncă nu există evaluări
- HIV - Acquired Immunodeficiency Syndrome - UnlockedDocument9 paginiHIV - Acquired Immunodeficiency Syndrome - UnlockedThalia FortuneÎncă nu există evaluări
- MCN 2Document7 paginiMCN 2Kat TaasinÎncă nu există evaluări
- Prelim Lecture Exam RationaleDocument107 paginiPrelim Lecture Exam RationaleMartin ClydeÎncă nu există evaluări
- Community Health NursingDocument4 paginiCommunity Health NursingJohn Vincent VasquezÎncă nu există evaluări
- What Is Global Health and Why Is It ImportantDocument7 paginiWhat Is Global Health and Why Is It ImportantSanty ManuelÎncă nu există evaluări
- Philippine HealthcareDocument16 paginiPhilippine HealthcareJacq CalaycayÎncă nu există evaluări
- Primary Health Care: Dr. Ariful Bari ChowdhuryDocument39 paginiPrimary Health Care: Dr. Ariful Bari ChowdhuryTanni ChowdhuryÎncă nu există evaluări
- Overview of Sexually Transmitted DiseasesDocument11 paginiOverview of Sexually Transmitted DiseasesPaulAliboghaÎncă nu există evaluări
- CHN Lecture WCCDocument75 paginiCHN Lecture WCCMeeKo VideñaÎncă nu există evaluări
- Answer and Rationale Communicable Disease NursingDocument17 paginiAnswer and Rationale Communicable Disease NursingCharles Gerard B. BeluanÎncă nu există evaluări
- Downloadfile 2Document8 paginiDownloadfile 2Michael SilvaÎncă nu există evaluări
- Epi 3rd Exam ReviewerDocument93 paginiEpi 3rd Exam ReviewerJillian AsdalaÎncă nu există evaluări
- Individual Case PresentationDocument20 paginiIndividual Case Presentationim. EliasÎncă nu există evaluări
- Idiopathic Thrombocytopenic Purpura (ITP)Document7 paginiIdiopathic Thrombocytopenic Purpura (ITP)Rizqka PertiwiÎncă nu există evaluări
- CD 1Document13 paginiCD 1Don MarcusÎncă nu există evaluări
- Report KAP COVID-19 Among The Community of Shah AlamDocument45 paginiReport KAP COVID-19 Among The Community of Shah AlamAdriana AfiqahÎncă nu există evaluări
- Primay Health CareDocument6 paginiPrimay Health Careمحمد عبدالهادي إسماعيلÎncă nu există evaluări
- Management of Tuberculosis: A guide for clinicians (eBook edition)De la EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Încă nu există evaluări
- Country Cooperation Strategy: IndonesiaDocument20 paginiCountry Cooperation Strategy: Indonesiafauziahputri29Încă nu există evaluări
- Philippine Health Care Delivery System - FinalDocument62 paginiPhilippine Health Care Delivery System - FinalRyan Michael Oducado0% (1)
- 0.1 Chapter 1 - Overview of Public Health Nursing in The PhilippinesDocument11 pagini0.1 Chapter 1 - Overview of Public Health Nursing in The PhilippinesJerreca DasasÎncă nu există evaluări
- 0.1 Chapter 1 - Overview of Public Health Nursing in The PhilippinesDocument11 pagini0.1 Chapter 1 - Overview of Public Health Nursing in The Philippinesaajeno10Încă nu există evaluări
- The Aquino Health AgendaDocument14 paginiThe Aquino Health AgendaIzzah Mei CaballeroÎncă nu există evaluări
- List of Accredited AgenciesDocument3 paginiList of Accredited AgenciescajaroÎncă nu există evaluări
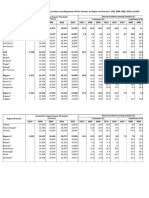
- Table 1. Annual Per Capita Poverty Threshold, Poverty Incidence and Magnitude of Poor Families, by Region and Province - 2006, 2009, 2012 and 2015Document12 paginiTable 1. Annual Per Capita Poverty Threshold, Poverty Incidence and Magnitude of Poor Families, by Region and Province - 2006, 2009, 2012 and 2015Cris Angelo Natanuan VispoÎncă nu există evaluări
- K Channel Takes A LEEP: July 10 at ABS-CBN Studio 8Document7 paginiK Channel Takes A LEEP: July 10 at ABS-CBN Studio 8Dennis OnidaÎncă nu există evaluări
- Appendices: "Be Trained To Be The Best, Be Linked To Success"Document27 paginiAppendices: "Be Trained To Be The Best, Be Linked To Success"Riza Mae AlceÎncă nu există evaluări
- PNP Police Entrance Exam Reviewer v2 PDFDocument100 paginiPNP Police Entrance Exam Reviewer v2 PDFARIEL VILLANUEVA33% (3)
- Midas HotelDocument3 paginiMidas HotelDorielyns SaratanÎncă nu există evaluări
- Class 1992 DirectoryDocument16 paginiClass 1992 DirectoryVincs KongÎncă nu există evaluări
- Calida Vigilant1Document4 paginiCalida Vigilant1Nami BuanÎncă nu există evaluări
- Executive Order No. 125Document8 paginiExecutive Order No. 125Jo Segismundo-JiaoÎncă nu există evaluări
- The Katipunan's CryDocument6 paginiThe Katipunan's CryCharmy SalvatoreÎncă nu există evaluări
- Manila Water 2010 Sustainability ReportDocument60 paginiManila Water 2010 Sustainability ReportArlina Liongson100% (1)
- Cars For Sale - 2018 PS BankDocument7 paginiCars For Sale - 2018 PS BankdayneblazeÎncă nu există evaluări
- Vista Land: Vista City ProjectDocument3 paginiVista Land: Vista City ProjectBusinessWorld100% (1)
- Araling Panlipunan 2Document26 paginiAraling Panlipunan 2Ja TapangÎncă nu există evaluări
- Excel Example Offered by Coursebank SP201Document40 paginiExcel Example Offered by Coursebank SP201Ivan Jon FerriolÎncă nu există evaluări
- LornasilveriocvDocument4 paginiLornasilveriocvgeorgeorwell9329Încă nu există evaluări
- Asia Envirocon Company ProfileDocument15 paginiAsia Envirocon Company ProfileDie Gedanken sind FreiÎncă nu există evaluări
- List of City and Municipality Nicknames in The PhilippinesDocument19 paginiList of City and Municipality Nicknames in The PhilippinesGerlen JuanÎncă nu există evaluări
- Philippines RegionsDocument7 paginiPhilippines Regionsmiho motoÎncă nu există evaluări
- ProspectDocument16 paginiProspectchristian benedict Lomibao100% (1)
- Soil Bearing Capacity Reference For Metro Manila, PhilippinesDocument7 paginiSoil Bearing Capacity Reference For Metro Manila, PhilippinesRox CardonaÎncă nu există evaluări
- List of Designated Travel AgenciesDocument2 paginiList of Designated Travel AgenciesRappler100% (3)
- Radio MemoriesDocument344 paginiRadio MemoriesPcnhs Sal100% (2)
- Position Paper (Cry of Balintawak) (Readings in Phil. History)Document2 paginiPosition Paper (Cry of Balintawak) (Readings in Phil. History)JeahannÎncă nu există evaluări
- BusinessDocument230 paginiBusinessRobert SonguitanÎncă nu există evaluări
- IRR of R. A. 7924Document13 paginiIRR of R. A. 7924Orville CipresÎncă nu există evaluări
- Urban Barangays in The PhilippinesDocument17 paginiUrban Barangays in The PhilippinesRico EdureseÎncă nu există evaluări
- Certification For No IpsDocument40 paginiCertification For No IpsTchr VhinzÎncă nu există evaluări
- Clup Volume 2-Land Use PlanDocument8 paginiClup Volume 2-Land Use PlanArch. Jan Echiverri0% (1)
- List of Authorized Online Remote Gaming PlatformsDocument1 paginăList of Authorized Online Remote Gaming PlatformsJusticeLezahÎncă nu există evaluări