S-ar putea să vă placă și
- Gastrointestinal Effects of Nsaids and Cox-2 Specific InhibitorsDocument43 paginiGastrointestinal Effects of Nsaids and Cox-2 Specific InhibitorsPutri WulandariÎncă nu există evaluări
- Management of Ibd - 15 March y MikhailDocument49 paginiManagement of Ibd - 15 March y Mikhailjordanmedics100% (1)
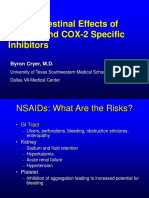
- Risks of Nsaids: Focus On Gi Risks of Over-The-Counter NsaidsDocument40 paginiRisks of Nsaids: Focus On Gi Risks of Over-The-Counter Nsaidspaul_calburean7899Încă nu există evaluări
- Lecture 16 GERDDocument44 paginiLecture 16 GERDSinthuÎncă nu există evaluări
- Raffaele Pezzilli, Lorenzo Fantini, Antonio Maria Morselli-LabateDocument51 paginiRaffaele Pezzilli, Lorenzo Fantini, Antonio Maria Morselli-LabateLeonÎncă nu există evaluări
- G I Toxicity of NSAIDsDocument59 paginiG I Toxicity of NSAIDsPann EiÎncă nu există evaluări
- Nonalcoholic Fatty Liver Disease (NAFLD) : Where Are We Today?Document32 paginiNonalcoholic Fatty Liver Disease (NAFLD) : Where Are We Today?Saad MotawéaÎncă nu există evaluări
- Inflammatory Bowel Disease RK2012Document212 paginiInflammatory Bowel Disease RK2012Nurul Kartika SariÎncă nu există evaluări
- Inflammatory Bowel DiseaseDocument59 paginiInflammatory Bowel DiseaseLala Rahma Qodriyan SofiakmiÎncă nu există evaluări
- NSAID Colon UlcersDocument5 paginiNSAID Colon UlcersFrederic IkkiÎncă nu există evaluări
- Stomach and Duodenum (Forsharing)Document79 paginiStomach and Duodenum (Forsharing)adversal8avrikÎncă nu există evaluări
- Effect of A Preoperative Proton Pump Inhibitor and Gastroesophageal Reflux Disease On Postoperative Nausea and VomitingDocument9 paginiEffect of A Preoperative Proton Pump Inhibitor and Gastroesophageal Reflux Disease On Postoperative Nausea and VomitingINICUOMÎncă nu există evaluări
- 3.a. Peptic Ulcer (DR - Fauzi Yusuf, SP - PD, KGEH)Document18 pagini3.a. Peptic Ulcer (DR - Fauzi Yusuf, SP - PD, KGEH)Irfandy Chairi Sulaiman LubisÎncă nu există evaluări
- GERDDocument47 paginiGERDSutanto TanakaÎncă nu există evaluări
- Summary and Conclusions: Urinary Biomarkers in Experimental DiabetesDocument1 paginăSummary and Conclusions: Urinary Biomarkers in Experimental DiabetesNikesh DoshiÎncă nu există evaluări
- CYP2C9 Polymorphism in Non-Steroidal Anti-Inflammatory Drugs-Induced GastropathyDocument6 paginiCYP2C9 Polymorphism in Non-Steroidal Anti-Inflammatory Drugs-Induced GastropathyFariz NurÎncă nu există evaluări
- CPD Januari 2013Document36 paginiCPD Januari 2013ledyÎncă nu există evaluări
- Gerd - NCCP - Kppik 2011 (Hotel Shangri La)Document28 paginiGerd - NCCP - Kppik 2011 (Hotel Shangri La)Fatmala HaningtyasÎncă nu există evaluări
- Iwamoto Et Al 2014 - DigestiveDocument7 paginiIwamoto Et Al 2014 - Digestivemattlight07Încă nu există evaluări
- Fever Cough and Fungal Infection (FARM)Document20 paginiFever Cough and Fungal Infection (FARM)Balamurugan KGÎncă nu există evaluări
- Crohns DiseaseDocument72 paginiCrohns Diseasea1savedÎncă nu există evaluări
- Case Presentation On Gut ObstructionDocument19 paginiCase Presentation On Gut Obstructionlakshitataneja1998Încă nu există evaluări
- Ge Reflux-MedDocument31 paginiGe Reflux-Medyour babysurgeonÎncă nu există evaluări
- Inflammatory DisturbancesDocument63 paginiInflammatory DisturbancesWang Ming YaÎncă nu există evaluări
- Enteral Nutrition Therapy For The Surgical PatientDocument52 paginiEnteral Nutrition Therapy For The Surgical PatientelenÎncă nu există evaluări
- Art 1 HT3Document3 paginiArt 1 HT3Glenda MaríaÎncă nu există evaluări
- Rheumatology Journal Club Gut Vasculitis: by DR Nur Hidayati Mohd SharifDocument36 paginiRheumatology Journal Club Gut Vasculitis: by DR Nur Hidayati Mohd SharifEida MohdÎncă nu există evaluări
- Gerd (Gastroesophageal Reflux DiseaseDocument43 paginiGerd (Gastroesophageal Reflux DiseaseRoselin Megasari MendrofaÎncă nu există evaluări
- Inflammatory Bowel Disease 5th YearDocument72 paginiInflammatory Bowel Disease 5th YearAi NurfaiziyahÎncă nu există evaluări
- Crohns DiseaseDocument72 paginiCrohns DiseaseFlavia CunhaÎncă nu există evaluări
- Usefulness of Vonoprazan, A Potassium Ion-Competitive Acid Blocker, For Primary Eradication of HelicobacterDocument8 paginiUsefulness of Vonoprazan, A Potassium Ion-Competitive Acid Blocker, For Primary Eradication of HelicobacterUlilta MuktadiraÎncă nu există evaluări
- GERD PathophysiologyDocument35 paginiGERD PathophysiologyKathlea Noble-dc100% (1)
- GERD Med StudentsaaaasdDocument54 paginiGERD Med StudentsaaaasdAlifiyanFithriyanaÎncă nu există evaluări
- Upper Gastrointestinal Bleeding: (UGIB)Document39 paginiUpper Gastrointestinal Bleeding: (UGIB)api-19916399Încă nu există evaluări
- A6. Tukak PeptikDocument31 paginiA6. Tukak PeptikSartika NapitupuluÎncă nu există evaluări
- Dyspepsia + GERDDocument38 paginiDyspepsia + GERDAgung Firmansyah SumantriÎncă nu există evaluări
- Assignment: Applied MedicineDocument10 paginiAssignment: Applied MedicineKhadija BakhtawarÎncă nu există evaluări
- INTRO - Types: Chron'sDocument47 paginiINTRO - Types: Chron'sfadliÎncă nu există evaluări
- Cco Gi CR 2013 SlidesDocument48 paginiCco Gi CR 2013 SlidesArtemSakhnoÎncă nu există evaluări
- Care Plan SBO VomingDocument6 paginiCare Plan SBO Vomingstring44Încă nu există evaluări
- Acute Gastrointestinal Bleeding: Diagnosis and TreatmentDe la EverandAcute Gastrointestinal Bleeding: Diagnosis and TreatmentKaren E. KimÎncă nu există evaluări
- 1430 - Falk - GERD 222Document34 pagini1430 - Falk - GERD 222Tengku Novia Eka PutriÎncă nu există evaluări
- The Safety of COX-2 Inhibitors: John J. Cush, MD Presbyterian Hospital of DallasDocument29 paginiThe Safety of COX-2 Inhibitors: John J. Cush, MD Presbyterian Hospital of DallaskitsilcÎncă nu există evaluări
- CP ON PUD (1) ADocument20 paginiCP ON PUD (1) ADeekshitha DanthuluriÎncă nu există evaluări
- Top Trials in Gastroenterology & HepatologyDe la EverandTop Trials in Gastroenterology & HepatologyEvaluare: 4.5 din 5 stele4.5/5 (7)
- Evidence-Based Nursing: Submitted By: de Guzman, Tammy S. de Leon, Jenalyn C. BSN113Document6 paginiEvidence-Based Nursing: Submitted By: de Guzman, Tammy S. de Leon, Jenalyn C. BSN113tammy_deguzman5223Încă nu există evaluări
- Cancer Gastrico AvancesDocument48 paginiCancer Gastrico AvancesSeal MachucaÎncă nu există evaluări
- Gastrointestinal Hemorrhage in The ICU: Doctor Chad Pulmonary & Critical Care MedicineDocument49 paginiGastrointestinal Hemorrhage in The ICU: Doctor Chad Pulmonary & Critical Care MedicinechadchimaÎncă nu există evaluări
- 03 PsoriasisDocument28 pagini03 PsoriasisGlen Lester ChiongÎncă nu există evaluări
- Exmd 509 Mcgill Stomach 2016Document36 paginiExmd 509 Mcgill Stomach 2016Sora OhÎncă nu există evaluări
- Pain Talk VipondDocument39 paginiPain Talk VipondHelmi IsmunandarÎncă nu există evaluări
- Case Presentation: Clostridium DifficileDocument35 paginiCase Presentation: Clostridium DifficileDnse LucidoÎncă nu există evaluări
- Molitch - Hot Topics Cushings Disease and AcromegalyDocument69 paginiMolitch - Hot Topics Cushings Disease and AcromegalyMaryOÎncă nu există evaluări
- Empirical Treatment With PPI in Acid Related DiseaseDocument41 paginiEmpirical Treatment With PPI in Acid Related DiseaseAyu Yunita Jaury HRÎncă nu există evaluări
- Nejmcp 2114026Document10 paginiNejmcp 2114026Engin AltınkayaÎncă nu există evaluări
- Acute Pancreatitis: Some Important Issues RevisitedDocument109 paginiAcute Pancreatitis: Some Important Issues RevisitedjlaguilarÎncă nu există evaluări
- 0830 - Ravi Esoph-Sm BWLDocument49 pagini0830 - Ravi Esoph-Sm BWLAlejandro Kanito Alvarez SÎncă nu există evaluări
- Barb Melo SkyDocument17 paginiBarb Melo SkyAfiqah So JasmiÎncă nu există evaluări
- Top Trials in Gastroenterology & Hepatology, 2nd EditionDe la EverandTop Trials in Gastroenterology & Hepatology, 2nd EditionÎncă nu există evaluări
- Kulkarni2018 PDFDocument7 paginiKulkarni2018 PDFtooba uroojÎncă nu există evaluări
- Pediatrics Shelf TopicsDocument5 paginiPediatrics Shelf TopicsSam Zeez100% (2)
- Risk of Social Media For Teens in An Urban SettingDocument4 paginiRisk of Social Media For Teens in An Urban Settingdiana nistoranÎncă nu există evaluări
- M3 Service ManualDocument115 paginiM3 Service ManualEmerson Gutiérrez CarrilloÎncă nu există evaluări
- Oxford Specialist Handbooks Addiction Medicine 2009 PDFDocument492 paginiOxford Specialist Handbooks Addiction Medicine 2009 PDFMahmoud Hassan100% (1)
- Pseudomonas Aeruginosa, 2013Document12 paginiPseudomonas Aeruginosa, 2013katiushikasÎncă nu există evaluări
- Respiratory Distress SyndromeDocument3 paginiRespiratory Distress SyndromeJamaica Louise Quetua MacalinoÎncă nu există evaluări
- Sciatic AdviceDocument3 paginiSciatic AdviceJohn Fightakis100% (2)
- Features: Viasys Bird VIP VentilatorDocument2 paginiFeatures: Viasys Bird VIP VentilatorNana MohamedÎncă nu există evaluări
- Status of DNB Seats - Bulletin - StatewiseSpecialitywise - WU26022009Document142 paginiStatus of DNB Seats - Bulletin - StatewiseSpecialitywise - WU26022009raghavagummadiÎncă nu există evaluări
- NEWS2 Chart 4 - Clinical Response To NEWS Trigger Thresholds - 0Document1 paginăNEWS2 Chart 4 - Clinical Response To NEWS Trigger Thresholds - 0echa okta anggrainiÎncă nu există evaluări
- Daftar Buku Perpustakaan: Tanggal Judul Buku Pengarang Kode Buku Keterangan (Edisi, Tahun, Penerbit)Document21 paginiDaftar Buku Perpustakaan: Tanggal Judul Buku Pengarang Kode Buku Keterangan (Edisi, Tahun, Penerbit)SuyotoAhmadÎncă nu există evaluări
- Rose Torres RN, MSN - CVDocument5 paginiRose Torres RN, MSN - CVrosetorresÎncă nu există evaluări
- Pelvic Trauma: DR Indro Wibowo SejatiDocument42 paginiPelvic Trauma: DR Indro Wibowo SejatiIndro WibowoÎncă nu există evaluări
- Dr. Ali Khamis - CVDocument2 paginiDr. Ali Khamis - CVAli KhamisÎncă nu există evaluări
- 10.2.3.30-Functional Systems Kurtzke FormDocument3 pagini10.2.3.30-Functional Systems Kurtzke FormGem Nicole P. AbrasaldoÎncă nu există evaluări
- Disaster Triage Forgotten Lessons in Pandemic Covid-19 Management - Dr. Yogi Prabowo, SpOT (K)Document23 paginiDisaster Triage Forgotten Lessons in Pandemic Covid-19 Management - Dr. Yogi Prabowo, SpOT (K)Clara EverlastÎncă nu există evaluări
- Distinctions Dental 2008Document64 paginiDistinctions Dental 2008Ellery July100% (3)
- ScienceDocument1 paginăScienceni putu.comsurya dianaÎncă nu există evaluări
- 1.basics of Anesthesiology. Anesthesia Machine and Equipments.Document41 pagini1.basics of Anesthesiology. Anesthesia Machine and Equipments.karim hassanÎncă nu există evaluări
- Network HospitalsDocument92 paginiNetwork Hospitalsvengatraj880% (1)
- 1 - Scene Size-UpDocument24 pagini1 - Scene Size-UpIman KadeÎncă nu există evaluări
- Resume: Nivetha RavichandranDocument3 paginiResume: Nivetha Ravichandran777Încă nu există evaluări
- The Role of Pharmacists in Minimizing Medication Errors in The Neonatal Intensive Care Unit: A Systematic ReviewDocument10 paginiThe Role of Pharmacists in Minimizing Medication Errors in The Neonatal Intensive Care Unit: A Systematic ReviewIJAR JOURNALÎncă nu există evaluări
- AcneDocument38 paginiAcneSavanna ChambersÎncă nu există evaluări
- Ifth DitionDocument25 paginiIfth DitionAlfie Omega0% (1)
- Auditory Function Screening Devices - NewbornDocument25 paginiAuditory Function Screening Devices - NewbornAdriana FerreiraÎncă nu există evaluări
- Who TRS 919Document228 paginiWho TRS 919Muhammad HabibiÎncă nu există evaluări
- Recent Advances in Surgery12 JP Medical Publishers 5a18b8551723ddf2aa406b59Document11 paginiRecent Advances in Surgery12 JP Medical Publishers 5a18b8551723ddf2aa406b59Swarnadeep ManiÎncă nu există evaluări
- Medical Findings and Child Sexual AbuseDocument26 paginiMedical Findings and Child Sexual AbuseEdgar Aleman CruzÎncă nu există evaluări