S-ar putea să vă placă și
- Care of WoundsDocument6 paginiCare of WoundsKimpoy Tu-osÎncă nu există evaluări
- Drugs Acting On The Respiratory SystemDocument13 paginiDrugs Acting On The Respiratory SystemAlloiBialbaÎncă nu există evaluări
- ) Administering Nasogastric Tube or Orogastric Tube FeedingDocument6 pagini) Administering Nasogastric Tube or Orogastric Tube FeedingJohn Pearl FernandezÎncă nu există evaluări
- Fundamentals of Nursing: OxygenationDocument56 paginiFundamentals of Nursing: OxygenationFEVIE ANNE BANATAOÎncă nu există evaluări
- Kardex, Drug Study and CheckDocument12 paginiKardex, Drug Study and CheckJemina Rafanan RacadioÎncă nu există evaluări
- Nasal PolypsDocument20 paginiNasal PolypsPauleenÎncă nu există evaluări
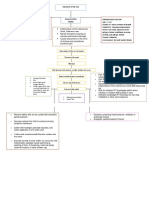
- Schematic Diagram BA HAP HRDocument2 paginiSchematic Diagram BA HAP HRMika MinsalanÎncă nu există evaluări
- Physical Assessment (Ippa)Document14 paginiPhysical Assessment (Ippa)Barbara HsuÎncă nu există evaluări
- Bowel SoundsDocument1 paginăBowel Soundsmh125fizanÎncă nu există evaluări
- RBS and FBSDocument5 paginiRBS and FBSAllenne Rose Labja Vale100% (1)
- ABDOMINAL ObjectiveDocument9 paginiABDOMINAL ObjectiveXing-Jin RomeroÎncă nu există evaluări
- Clinical Guidelines (Nursing) - Indwelling Urinary Catheter - Insertion and Ongoing CareDocument8 paginiClinical Guidelines (Nursing) - Indwelling Urinary Catheter - Insertion and Ongoing CareLeeÎncă nu există evaluări
- Chronic Obstructive Pulmonary Disease: Presented byDocument25 paginiChronic Obstructive Pulmonary Disease: Presented byChinni 12599Încă nu există evaluări
- Tracheostomy SlidesDocument24 paginiTracheostomy SlidesMohammed AdamÎncă nu există evaluări
- Sample QuestionnaireDocument10 paginiSample QuestionnaireJess Fernandez BorgaÎncă nu există evaluări
- Tranexamic AcidDocument18 paginiTranexamic AcidFatima Love Ariate-ArcasetasÎncă nu există evaluări
- Anatomy and Physiology of NeonatesDocument17 paginiAnatomy and Physiology of NeonatesYu ShiÎncă nu există evaluări
- Legaspi - Preparing Medication From A Vial ChecklistDocument4 paginiLegaspi - Preparing Medication From A Vial ChecklistJason LumayaÎncă nu există evaluări
- Assessing Respiration: Fundamentals of Nursing Practice, RleDocument2 paginiAssessing Respiration: Fundamentals of Nursing Practice, RleMONIQUE GONZALES0% (1)
- Module V ActDocument3 paginiModule V ActQueencess hayoÎncă nu există evaluări
- Nebulization 1Document3 paginiNebulization 1Shane Aileen AngelesÎncă nu există evaluări
- Care of Clients With Problems in Oxygenation (Part 2)Document88 paginiCare of Clients With Problems in Oxygenation (Part 2)mikErlhÎncă nu există evaluări
- Fistulectomy: - Prepared byDocument65 paginiFistulectomy: - Prepared byMonette Abalos MendovaÎncă nu există evaluări
- Types of ShocksDocument33 paginiTypes of Shocksmark OrpillaÎncă nu există evaluări
- Sub - Medical Surgical Nursing: Assignment On CVP MonitoringDocument11 paginiSub - Medical Surgical Nursing: Assignment On CVP Monitoringkamini ChoudharyÎncă nu există evaluări
- Sultan Kudarat State University College of Health SciencesDocument7 paginiSultan Kudarat State University College of Health SciencesRheal P EsmailÎncă nu există evaluări
- CVP - Nursing Performance ChecklistDocument3 paginiCVP - Nursing Performance ChecklistJoy Jarin75% (4)
- NCP'SDocument10 paginiNCP'SEjie Boy IsagaÎncă nu există evaluări
- Tracheostomy CareDocument4 paginiTracheostomy CareEriel Custodio Quijada100% (2)
- Discharge Planning PaperDocument5 paginiDischarge Planning Paperapi-283173905Încă nu există evaluări
- Critical CareDocument5 paginiCritical Careapi-353947564Încă nu există evaluări
- Case Study: Christine Joy P. de Chavez, SNDocument23 paginiCase Study: Christine Joy P. de Chavez, SNHELLOÎncă nu există evaluări
- First Semester 2020-2021 Study Guide: University of The CordillerasDocument13 paginiFirst Semester 2020-2021 Study Guide: University of The CordillerasJonalyn EtongÎncă nu există evaluări
- Vital SignsDocument6 paginiVital SignsJan Jamison ZuluetaÎncă nu există evaluări
- Cardiac MonitoringDocument19 paginiCardiac MonitoringYaska Musa100% (1)
- OxygenationDocument57 paginiOxygenationscent0730100% (3)
- Kidney CancerDocument31 paginiKidney CancerEfren Elico VenguaÎncă nu există evaluări
- Intensive Nursing Practicum: Bachelor of Science in NursingDocument7 paginiIntensive Nursing Practicum: Bachelor of Science in NursingMichelle Gliselle Guinto MallareÎncă nu există evaluări
- Fundamentals of Nursing NCLEX Practice Questions Quiz 1Document39 paginiFundamentals of Nursing NCLEX Practice Questions Quiz 1Regine Mae Encinada100% (1)
- Transcult - Nursing PPT Nurs 450 FinalDocument32 paginiTranscult - Nursing PPT Nurs 450 FinalJuan Cruz100% (1)
- Gastro NotesDocument24 paginiGastro NotesMicah EllaÎncă nu există evaluări
- Administering Oxygen by Nasal Catheter, CannulaDocument28 paginiAdministering Oxygen by Nasal Catheter, CannulaAngie Mandeoya100% (1)
- Case StudyDocument23 paginiCase StudyFarah Jelimae BagniÎncă nu există evaluări
- Respiratory ModalitiesDocument87 paginiRespiratory ModalitiesLj Ferolino100% (2)
- Ethico Legal Considerations and Issues in The Care of Sick Mother and Child QuestionsDocument5 paginiEthico Legal Considerations and Issues in The Care of Sick Mother and Child QuestionsQueeny Anne ApilÎncă nu există evaluări
- Pulmonary HypertensionDocument10 paginiPulmonary HypertensionCkaye GansubinÎncă nu există evaluări
- CYSTOCLYSISDocument1 paginăCYSTOCLYSISzerpthederpÎncă nu există evaluări
- Digestive System Anatomy PhysiologyDocument20 paginiDigestive System Anatomy PhysiologyKids JangÎncă nu există evaluări
- Nursing Care of A Family When A Child Has A Long-Term or Terminal Illness Nursing Care of A Family When A Child Has A Long-Term or Terminal IllnessDocument31 paginiNursing Care of A Family When A Child Has A Long-Term or Terminal Illness Nursing Care of A Family When A Child Has A Long-Term or Terminal IllnessJoanna Mie EstrososÎncă nu există evaluări
- Cretenism Case StudyDocument8 paginiCretenism Case StudyMonica Marie MoralesÎncă nu există evaluări
- ATELECTASISDocument4 paginiATELECTASISAshley Jane MacapayadÎncă nu există evaluări
- Nursing Care of Clients in Emergency Situation 1Document48 paginiNursing Care of Clients in Emergency Situation 1Danica FrancoÎncă nu există evaluări
- Can Cancer Be Prevented: o Classification of NeoplasmsDocument5 paginiCan Cancer Be Prevented: o Classification of NeoplasmsMarielle ChuaÎncă nu există evaluări
- GRP 20 Final Abscess Case StudyDocument14 paginiGRP 20 Final Abscess Case StudyBorja, Kimberly GraceÎncă nu există evaluări
- Anti - Anginal MedicationDocument41 paginiAnti - Anginal MedicationShine StephenÎncă nu există evaluări
- Colostomy CareDocument7 paginiColostomy CareChrismon Arek KeneÎncă nu există evaluări
- Drugs Acting On Respiratory SystemDocument15 paginiDrugs Acting On Respiratory SystemQusai BassamÎncă nu există evaluări
- Management of Tuberculosis: A guide for clinicians (eBook edition)De la EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Încă nu există evaluări
- Problems With OxygenationDocument92 paginiProblems With OxygenationEbiÎncă nu există evaluări
- The Respiratory System or Pulmonary SystemDocument53 paginiThe Respiratory System or Pulmonary Systemfharidaismail47Încă nu există evaluări
- Biological Disaster - Biological Disaster Management & Types of Biological DisastersDocument3 paginiBiological Disaster - Biological Disaster Management & Types of Biological DisastersS DÎncă nu există evaluări
- HashimotoDocument9 paginiHashimotoFrinkooFrinkoBÎncă nu există evaluări
- Stem Cell Research Thesis TopicsDocument7 paginiStem Cell Research Thesis Topicsdnqjxbz2100% (2)
- Claw Hand: Presentation By: Preksha, Nevil and ShubhamDocument21 paginiClaw Hand: Presentation By: Preksha, Nevil and ShubhamvaishnaviÎncă nu există evaluări
- Rash and Fever After Sulfasalazine UseDocument5 paginiRash and Fever After Sulfasalazine UseChistian LassoÎncă nu există evaluări
- Disorders of The EarDocument8 paginiDisorders of The EarVinz Khyl G. CastillonÎncă nu există evaluări
- Community Medicine Card QuestonsDocument10 paginiCommunity Medicine Card Questons202Manjida Rahman OniÎncă nu există evaluări
- EnglishDocument12 paginiEnglishAditya RajÎncă nu există evaluări
- Exit Screening QuestionnaireDocument2 paginiExit Screening QuestionnaireСвити ОдинÎncă nu există evaluări
- Essentials of Orthodontics PDFDocument591 paginiEssentials of Orthodontics PDFKENAN ABBARA100% (1)
- Ace Score Resilience Q 2Document5 paginiAce Score Resilience Q 2KhadijaAnamÎncă nu există evaluări
- Causes and Characteristics of Horizontal Positional NystagmusDocument9 paginiCauses and Characteristics of Horizontal Positional NystagmusRudolfGerÎncă nu există evaluări
- Chap 1Document27 paginiChap 1MownikaÎncă nu există evaluări
- Home ScienceDocument39 paginiHome ScienceBridgit OsebeÎncă nu există evaluări
- Proposed by Ms Dinopol, M., Ms Awayan, S., Ms Regis, S. (2018) 1Document4 paginiProposed by Ms Dinopol, M., Ms Awayan, S., Ms Regis, S. (2018) 1Franz goÎncă nu există evaluări
- Avika ReportDocument2 paginiAvika ReportChinish KalraÎncă nu există evaluări
- Inflammation, Infection, and Microbiome in Cancers Evidence, Mechanisms, and Implications by Jun SunDocument513 paginiInflammation, Infection, and Microbiome in Cancers Evidence, Mechanisms, and Implications by Jun SunSaiyan DianÎncă nu există evaluări
- Ensayo - InglésDocument11 paginiEnsayo - InglésMery RosalesÎncă nu există evaluări
- B Science 10 Quarter 3 Module 2 (Week 3)Document17 paginiB Science 10 Quarter 3 Module 2 (Week 3)Daisy Soriano PrestozaÎncă nu există evaluări
- Congenital Anomalies of KidneDocument7 paginiCongenital Anomalies of KidneSanthosh.S.U100% (2)
- MD0170 Arthropod Identification Surveys PDFDocument124 paginiMD0170 Arthropod Identification Surveys PDFDonT_RNÎncă nu există evaluări
- CP-PHC 1 Removal ExamDocument6 paginiCP-PHC 1 Removal ExamJuana I. Dela Cruz100% (1)
- Prevenção Secundária Avc Isquêmico - Guideline 2022Document41 paginiPrevenção Secundária Avc Isquêmico - Guideline 2022Felipe Stoquetti de AbreuÎncă nu există evaluări
- Icu - Training Module Outline 7Document7 paginiIcu - Training Module Outline 7MikhaelEarlSantosTacorda100% (1)
- Part 2. 3Document40 paginiPart 2. 3Karen mae alvarroÎncă nu există evaluări
- The Management of Seborrheic Dermatitis 2020Document11 paginiThe Management of Seborrheic Dermatitis 2020Sema GigaramadanÎncă nu există evaluări
- Comparison of Chest X-Ray Findings Between Primary and Secondary Multidrug Resistant Pulmonary TuberculosisDocument8 paginiComparison of Chest X-Ray Findings Between Primary and Secondary Multidrug Resistant Pulmonary TuberculosismahyaÎncă nu există evaluări
- Virulence FactorsDocument49 paginiVirulence FactorsHira PanhwerÎncă nu există evaluări
- Diabetes Pridiction Using Machine LearningDocument31 paginiDiabetes Pridiction Using Machine LearningAbhishekÎncă nu există evaluări
- PresbycusisDocument2 paginiPresbycusisRomano Paulo BanzonÎncă nu există evaluări