S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Asthma:: Case Scenario: DDXDocument10 paginiAsthma:: Case Scenario: DDXFemale calmÎncă nu există evaluări
- Exam Questions HAAD-RN: HAAD Licensure Examination For Registered NursesDocument5 paginiExam Questions HAAD-RN: HAAD Licensure Examination For Registered NursesGreeshma victorÎncă nu există evaluări
- Design and Development of Multi-Purpose Chair in Educational SettingDocument26 paginiDesign and Development of Multi-Purpose Chair in Educational SettingVinze Jan Santos100% (2)
- MSW Umbilical HerniaDocument7 paginiMSW Umbilical HerniaTurolLinkÎncă nu există evaluări
- Case Study For DiscussionDocument3 paginiCase Study For DiscussionSiti nur Kholifatus samsiyahÎncă nu există evaluări
- Chapter 2 Respiratory AssessmentDocument9 paginiChapter 2 Respiratory AssessmentKathleen Dela CruzÎncă nu există evaluări
- A Systematic Review and Meta-Analysis of Children WithDocument34 paginiA Systematic Review and Meta-Analysis of Children WithDaniela GiraldoÎncă nu există evaluări
- Medical Surgical Nursing: DownloadDocument1 paginăMedical Surgical Nursing: DownloadKim LeeÎncă nu există evaluări
- All PneumologyDocument40 paginiAll PneumologyDiaconu AndreeaÎncă nu există evaluări
- HistoryandPhysicalExamDocument105 paginiHistoryandPhysicalExamsilentscream0618Încă nu există evaluări
- AsthmaDocument2 paginiAsthmaNaeem ZubairÎncă nu există evaluări
- NHH TemplateDocument6 paginiNHH TemplateCaryl EteÎncă nu există evaluări
- Chest Physiotherapy and Postural DrainageDocument24 paginiChest Physiotherapy and Postural DrainageRiza Angela BarazanÎncă nu există evaluări
- Ptk. 51 (Grindelia Pentarkan) For Difficult Breathing / Bronchial Asthma - SchwabeDocument4 paginiPtk. 51 (Grindelia Pentarkan) For Difficult Breathing / Bronchial Asthma - SchwabeDr. Kazy Habibur RahmanÎncă nu există evaluări
- Nursing Care of The Child With Congenital Heart DiseaseDocument5 paginiNursing Care of The Child With Congenital Heart DiseaseAisyahKautsarIlmiÎncă nu există evaluări
- Detailed Health History: PneumoniaDocument6 paginiDetailed Health History: PneumoniaBakushido100% (2)
- Nursing Care Plan Ineffective Airway Clearance: Assessment Diagnosis Outcome IdentificationDocument9 paginiNursing Care Plan Ineffective Airway Clearance: Assessment Diagnosis Outcome IdentificationAngelokeizer GavinoÎncă nu există evaluări
- 409 Pope, B. and Maillie, S. CCRN-PCCN Review Multisystem and Q and ADocument21 pagini409 Pope, B. and Maillie, S. CCRN-PCCN Review Multisystem and Q and Agliftan100% (2)
- Nursing Board:Licensure Exam Answer Key: NP1 Nursing Board Exam November 2008 Answer Key 'Foundation of Professional Nursing Practice'Document6 paginiNursing Board:Licensure Exam Answer Key: NP1 Nursing Board Exam November 2008 Answer Key 'Foundation of Professional Nursing Practice'Thalia RhodaÎncă nu există evaluări
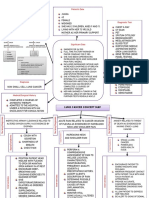
- Lung Cancer Concept Map-Group 2Document2 paginiLung Cancer Concept Map-Group 2Maria Cristina100% (2)
- AlbuminDocument14 paginiAlbuminMaria Chona Penillos HularÎncă nu există evaluări
- Lofnac Suppo Diclofenac Sodium Tablets 100MG PilDocument7 paginiLofnac Suppo Diclofenac Sodium Tablets 100MG PilepakerryÎncă nu există evaluări
- MCQDocument136 paginiMCQRahul Patil100% (1)
- Cap NCPDocument6 paginiCap NCPMarlo Parayno100% (2)
- Hypoxemia in ICU: Prepared by Hadi JazanDocument41 paginiHypoxemia in ICU: Prepared by Hadi JazanHadi JazanÎncă nu există evaluări
- Asthma Action Plan EnglishDocument7 paginiAsthma Action Plan EnglishRizal PharmÎncă nu există evaluări
- Standard Treatment Protocol of Emergency Health Service PackageDocument298 paginiStandard Treatment Protocol of Emergency Health Service PackageF OÎncă nu există evaluări
- Chlorine and Its SafetypDocument54 paginiChlorine and Its SafetypHiranmoy MisraÎncă nu există evaluări
- Case Study: Acute Exacarbation Chronic Obstructive Aspiration Disease (Aecoad)Document5 paginiCase Study: Acute Exacarbation Chronic Obstructive Aspiration Disease (Aecoad)Muhammad Alif100% (1)
- Physiologic Changes in Aging Affecting Various SystemsDocument27 paginiPhysiologic Changes in Aging Affecting Various SystemsMina75% (4)