S-ar putea să vă placă și
- Ectoparasites and Parasites On Human'S Skin/Body Surface: Parasitology DepartmentDocument36 paginiEctoparasites and Parasites On Human'S Skin/Body Surface: Parasitology DepartmentJimmy Fran IIÎncă nu există evaluări
- Ectoparasites and Parasites On Human'S Skin/Body Surface: Parasitology DepartmentDocument36 paginiEctoparasites and Parasites On Human'S Skin/Body Surface: Parasitology DepartmentmiaraissaÎncă nu există evaluări
- Ectoparasites and Parasites On Human'S Skin/Body Surface: Parasitology DepartmentDocument38 paginiEctoparasites and Parasites On Human'S Skin/Body Surface: Parasitology DepartmentArifin MuhammadÎncă nu există evaluări
- (K6) Ectoparasites and Parasites On Human's Skinbody SurfaceDocument38 pagini(K6) Ectoparasites and Parasites On Human's Skinbody SurfaceArifin MuhammadÎncă nu există evaluări
- Important Diseases1 - Skin and EyeDocument40 paginiImportant Diseases1 - Skin and EyePeiyong TanÎncă nu există evaluări
- Eukaryotic Diseases - 06Document33 paginiEukaryotic Diseases - 06Vien WhitlockÎncă nu există evaluări
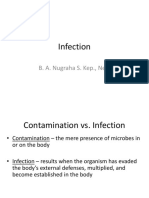
- Infection: B. A. Nugraha S. Kep., NersDocument86 paginiInfection: B. A. Nugraha S. Kep., NersSweatenia MahagoniÎncă nu există evaluări
- Micr Biology: Microbial Diseases of The Skin and EyesDocument62 paginiMicr Biology: Microbial Diseases of The Skin and EyesIvy L VonierÎncă nu există evaluări
- Lesson 8 PEDICULOSISDocument39 paginiLesson 8 PEDICULOSISJulius Memeg PanayoÎncă nu există evaluări
- Fungal ClassificationDocument109 paginiFungal ClassificationMirza Shaharyar BaigÎncă nu există evaluări
- LeishmaniaFilaria Part 1Document45 paginiLeishmaniaFilaria Part 1YS Nate100% (1)
- Derm PathologyDocument21 paginiDerm PathologyMaria GeorgeÎncă nu există evaluări
- Penyakit Kulit Tropis: Heryanto SyamsuddinDocument248 paginiPenyakit Kulit Tropis: Heryanto SyamsuddinBunga Tri AmandaÎncă nu există evaluări
- Parasites Associated With Skin Infection - COR TRANXDocument12 paginiParasites Associated With Skin Infection - COR TRANXAna Cristina MontillanoÎncă nu există evaluări
- Infestation: ScabiesDocument16 paginiInfestation: ScabiesBrix ValdrizÎncă nu există evaluări
- ScabiesDocument8 paginiScabiesJessica Dumayas Dela RosaÎncă nu există evaluări
- Communicable Diseases2Document46 paginiCommunicable Diseases2wanjalakijanahÎncă nu există evaluări
- Notes Skin Eye Ears Infections MicrobioDocument18 paginiNotes Skin Eye Ears Infections MicrobioChristiel John MagtibayÎncă nu există evaluări
- Parasit IntegumenDocument43 paginiParasit Integumenandi mutiah armusÎncă nu există evaluări
- Lecturer 3: Warning!!!! This Should Not Replace Your Note or Textbook in AnyformDocument13 paginiLecturer 3: Warning!!!! This Should Not Replace Your Note or Textbook in AnyformHabibÎncă nu există evaluări
- InfestDocument26 paginiInfestIndraÎncă nu există evaluări
- Foundations in Microbiology: The Cocci of Medical Importance TalaroDocument71 paginiFoundations in Microbiology: The Cocci of Medical Importance TalaroOdurÎncă nu există evaluări
- DMS-1 K6 EktoparasitDocument24 paginiDMS-1 K6 EktoparasitDevina KriskineyaÎncă nu există evaluări
- Monkey PoxDocument29 paginiMonkey PoxMalavika A GÎncă nu există evaluări
- Bacterial InfectionDocument41 paginiBacterial InfectionUmmi Rinandari100% (1)
- Overview of Skin InfectionsDocument53 paginiOverview of Skin Infectionsadamu mohammadÎncă nu există evaluări
- 2F and 2H Lecture 10Document50 pagini2F and 2H Lecture 10Mark PalomarÎncă nu există evaluări
- ScabiesDocument39 paginiScabiesShahzeb KhanÎncă nu există evaluări
- Skin Infestation PDFDocument30 paginiSkin Infestation PDFHampson MalekanoÎncă nu există evaluări
- Leishmaniasis - Postgraduate ClassDocument33 paginiLeishmaniasis - Postgraduate Classodhiambo samwelÎncă nu există evaluări
- Document From BenjaminfjodDocument21 paginiDocument From BenjaminfjodBenjamin VanlaltlansangaÎncă nu există evaluări
- Reviewer in Micro para Lec FinalsDocument9 paginiReviewer in Micro para Lec FinalsJohn Carl CastilloÎncă nu există evaluări
- General Study Guide - 2: - For Each Insect/pathogen CombinationDocument20 paginiGeneral Study Guide - 2: - For Each Insect/pathogen CombinationHerold Riwaldo SÎncă nu există evaluări
- Overview Common Dermatologic Problems in ChildrenDocument26 paginiOverview Common Dermatologic Problems in Childrenokwadha simionÎncă nu există evaluări
- Dermatology 3Document24 paginiDermatology 3حسين طاهر حاتم طاهرÎncă nu există evaluări
- Sarcoptes Scabiei: ScabiesDocument39 paginiSarcoptes Scabiei: ScabiesEx CalioseÎncă nu există evaluări
- Microbial Diseases of Skin & EyesDocument29 paginiMicrobial Diseases of Skin & Eyesbriterry2008Încă nu există evaluări
- wk11 INFECTIOUS DISORDER PART TWODocument52 paginiwk11 INFECTIOUS DISORDER PART TWOclaire yowsÎncă nu există evaluări
- Bacterial - Viral InfectionsDocument61 paginiBacterial - Viral InfectionsMoayad NawaflehÎncă nu există evaluări
- Skin Diseases Presentation2Document40 paginiSkin Diseases Presentation2DaniTadeÎncă nu există evaluări
- Skin Infections and InfestationsDocument37 paginiSkin Infections and InfestationsAremu OlatayoÎncă nu există evaluări
- Pathogens That Involve The SkinDocument57 paginiPathogens That Involve The SkinLeeShauran100% (2)
- Bacterial Infections: Infections Caused by Gram Positive OrganismsDocument81 paginiBacterial Infections: Infections Caused by Gram Positive OrganismsJamalul AdilÎncă nu există evaluări
- Superficial Mycoses Group 4Document38 paginiSuperficial Mycoses Group 4prudence azenaborÎncă nu există evaluări
- Bullous Disorders, Bacterial and Fungal Skin InfectionsDocument95 paginiBullous Disorders, Bacterial and Fungal Skin InfectionsDeborah ChemutaiÎncă nu există evaluări
- Scabies and PediculosisDocument22 paginiScabies and PediculosisEvady IllusionÎncă nu există evaluări
- Infectious Diseases of The Skin and EyesDocument29 paginiInfectious Diseases of The Skin and EyesgracegozaliÎncă nu există evaluări
- Cme 2012 WarrenDocument69 paginiCme 2012 WarrenMateen ShukriÎncă nu există evaluări
- Classification and Epidemiology of Communicable DiseasesDocument40 paginiClassification and Epidemiology of Communicable DiseasesRwapembe StephenÎncă nu există evaluări
- Gram Positive Rod of Medical Imortance IIDocument36 paginiGram Positive Rod of Medical Imortance IIJoeyÎncă nu există evaluări
- Skin Disease: Roshana MallawaarachchiDocument51 paginiSkin Disease: Roshana MallawaarachchiRoshana Mallawaarachchi100% (1)
- Microbial Diseases of The Skin & EyesDocument52 paginiMicrobial Diseases of The Skin & EyesAna100% (3)
- Monkeypox RA and MX 27 Mei 2022Document45 paginiMonkeypox RA and MX 27 Mei 2022alfonso de albuquerqueÎncă nu există evaluări
- Bacterial InfectionDocument41 paginiBacterial InfectionrranindyaprabasaryÎncă nu există evaluări
- P.S Very Nice!! May Pa-Picture Si Mayora!:D: FolliculitisDocument7 paginiP.S Very Nice!! May Pa-Picture Si Mayora!:D: FolliculitisBea SartoÎncă nu există evaluări
- Case Presentation CLMDocument30 paginiCase Presentation CLMShinta Dewi RahmadhaniÎncă nu există evaluări
- Foundations in Microbiology: TalaroDocument71 paginiFoundations in Microbiology: Talaromertx013Încă nu există evaluări
- The Science Which Deals With The Relation of Insects, Arachnids, and Other Arthropods To Parasitic Infestations and Diseases of Man and AnimalsDocument44 paginiThe Science Which Deals With The Relation of Insects, Arachnids, and Other Arthropods To Parasitic Infestations and Diseases of Man and AnimalsRabin BaniyaÎncă nu există evaluări
- Peranan Reseptor Progesteron Terhadap Kanker Endometrium: Referat Onkologi GinekologiDocument1 paginăPeranan Reseptor Progesteron Terhadap Kanker Endometrium: Referat Onkologi GinekologiLydia KosasihÎncă nu există evaluări
- H PyloriDocument8 paginiH PyloriLydia KosasihÎncă nu există evaluări
- Novena For: To ST Josemaría EscriváDocument12 paginiNovena For: To ST Josemaría EscriváLydia KosasihÎncă nu există evaluări
- Diagnostic of H PyloriDocument15 paginiDiagnostic of H PyloriLydia KosasihÎncă nu există evaluări
- BJMP 2015 8 1 A804Document10 paginiBJMP 2015 8 1 A804Lydia KosasihÎncă nu există evaluări
- EpidemiologiDocument10 paginiEpidemiologiLydia KosasihÎncă nu există evaluări
- Kimia Kanker ParuDocument8 paginiKimia Kanker ParuLydia KosasihÎncă nu există evaluări
- Lung Cancer Fact Sheet - American Lung AssociationDocument7 paginiLung Cancer Fact Sheet - American Lung AssociationLydia KosasihÎncă nu există evaluări
- Ca ParuDocument35 paginiCa ParuLydia KosasihÎncă nu există evaluări
- Ca ParuDocument35 paginiCa ParuLydia KosasihÎncă nu există evaluări
- Presentation 1Document4 paginiPresentation 1Lydia KosasihÎncă nu există evaluări
- Aterioskleorisi & PJK - CVS-K33Document36 paginiAterioskleorisi & PJK - CVS-K33Lydia KosasihÎncă nu există evaluări
- Dr. Bambang SugengDocument32 paginiDr. Bambang SugengLydia KosasihÎncă nu există evaluări
- Characteristic of Cardiac Muscle Cells - CVSK4Document36 paginiCharacteristic of Cardiac Muscle Cells - CVSK4Lydia KosasihÎncă nu există evaluări
- Mdentom NotesDocument30 paginiMdentom NotesMacy MarianÎncă nu există evaluări
- Defense Cheat SheetDocument5 paginiDefense Cheat SheetAngelica Kayte MontalboÎncă nu există evaluări
- 144 Diagnosa Non SpesialistikDocument26 pagini144 Diagnosa Non SpesialistikAlfani FlorenceÎncă nu există evaluări
- Dermoscopy in General DermatologyDocument16 paginiDermoscopy in General DermatologyMaestro JadÎncă nu există evaluări
- FNCP PEDICULOSISDocument1 paginăFNCP PEDICULOSISmichaelurielÎncă nu există evaluări
- s00436 020 06847 5Document19 paginis00436 020 06847 5Diary JafÎncă nu există evaluări
- Grade 2 Health CGDocument10 paginiGrade 2 Health CGAriah TugadoÎncă nu există evaluări
- Cattle and Sheep Medicine. 1ed. Philip R Scott. 2011-MinDocument241 paginiCattle and Sheep Medicine. 1ed. Philip R Scott. 2011-MinPaula Alejandra Moreno M100% (1)
- Flyer PediculosisDocument3 paginiFlyer Pediculosisronan_2905Încă nu există evaluări
- Roseola-Red Tide-Pediculosis-Covid19Document7 paginiRoseola-Red Tide-Pediculosis-Covid19christian quiaoitÎncă nu există evaluări
- Nclex New Lastest 1Document240 paginiNclex New Lastest 1Nadim KhalidÎncă nu există evaluări
- CD7 2021 InfestationsDocument20 paginiCD7 2021 InfestationsNhelia Santos BañagaÎncă nu există evaluări
- 16 Lice & ScabiesDocument32 pagini16 Lice & ScabiesRory WilliamsÎncă nu există evaluări
- Pediculosis: Pubis (Pubic Louse)Document4 paginiPediculosis: Pubis (Pubic Louse)christian quiaoitÎncă nu există evaluări
- Miscellaneous DrugsDocument59 paginiMiscellaneous Drugsreadbooks86Încă nu există evaluări
- 4 Tra - Communicable Disease NursingDocument44 pagini4 Tra - Communicable Disease NursingJoshua Delantar100% (1)
- Nail Changes: III-A '07 - Derma MegatableDocument21 paginiNail Changes: III-A '07 - Derma MegatableAileen Peña100% (2)
- Management of Client With Integumentary DisordersDocument97 paginiManagement of Client With Integumentary Disordersduday76100% (1)
- DLP Health 2 - 2nd QuarterDocument14 paginiDLP Health 2 - 2nd QuarterJennifer Parillo-BalangÎncă nu există evaluări
- Clinical Practice Update:: Pediculosis CapitisDocument8 paginiClinical Practice Update:: Pediculosis CapitisAnizha AdriyaniÎncă nu există evaluări
- Lice (Pediculosis) and HomoeopathyDocument11 paginiLice (Pediculosis) and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- Daftar Penyakit Kompetensi 4ADocument12 paginiDaftar Penyakit Kompetensi 4ARoy Sandy PermanaÎncă nu există evaluări
- Artikel JambiDocument12 paginiArtikel JambiRifka Purnama SariÎncă nu există evaluări
- ScabiesDocument39 paginiScabiesShahzeb KhanÎncă nu există evaluări
- Hair Care: BY:-Mrs. Neelofur I. AliDocument20 paginiHair Care: BY:-Mrs. Neelofur I. AliNeelofur Ibran Ali100% (1)
- Cymbopogon Nardus (Citronella) Leaves Extract: Insecticidal Effect On Pediculus Humanus Capitis (Head Lice)Document17 paginiCymbopogon Nardus (Citronella) Leaves Extract: Insecticidal Effect On Pediculus Humanus Capitis (Head Lice)Maris PolintanÎncă nu există evaluări
- Skin DisordersDocument202 paginiSkin DisordersMj Briones100% (1)
- Nclex New Lastest New LastDocument266 paginiNclex New Lastest New LastNadim Khalid0% (2)
- No. Nama Penyakit Kode Dan Nama Diagnosa ICD 10Document16 paginiNo. Nama Penyakit Kode Dan Nama Diagnosa ICD 10Sari Eka RahayuÎncă nu există evaluări
- Hair CareDocument11 paginiHair Carepreeti sharmaÎncă nu există evaluări