S-ar putea să vă placă și
- Staff Nurse Notification-1Document2 paginiStaff Nurse Notification-1Senthil KumarÎncă nu există evaluări
- Library ClerkDocument2 paginiLibrary ClerkSenthil KumarÎncă nu există evaluări
- RenewalPremium 26137073Document1 paginăRenewalPremium 26137073Senthil KumarÎncă nu există evaluări
- Application FormDocument4 paginiApplication FormSenthil KumarÎncă nu există evaluări
- Advertisement Foreign Coach PDFDocument2 paginiAdvertisement Foreign Coach PDFSenthil KumarÎncă nu există evaluări
- Walk in InterviewDocument5 paginiWalk in InterviewSenthil KumarÎncă nu există evaluări
- Ischemia PresentationDocument2 paginiIschemia PresentationMOHAMED ASHICÎncă nu există evaluări
- Icons Pack - OptionalDocument1 paginăIcons Pack - OptionalSenthil KumarÎncă nu există evaluări
- Notification SMI SKDocument2 paginiNotification SMI SKSenthil KumarÎncă nu există evaluări
- AdvportblairDocument6 paginiAdvportblairSenthil KumarÎncă nu există evaluări
- Read - Me (Font Installation) PDFDocument1 paginăRead - Me (Font Installation) PDFAbeanÎncă nu există evaluări
- Application FormDocument4 paginiApplication FormSenthil KumarÎncă nu există evaluări
- Transfer and Posting of Police Officer & Personnel - SP (HQ) DT 18.01.19 PDFDocument2 paginiTransfer and Posting of Police Officer & Personnel - SP (HQ) DT 18.01.19 PDFSenthil KumarÎncă nu există evaluări
- MSc Yoga Regulations at Annamalai UniversityDocument29 paginiMSc Yoga Regulations at Annamalai UniversitySenthil KumarÎncă nu există evaluări
- Application FormDocument4 paginiApplication FormSenthil KumarÎncă nu există evaluări
- ESIC recruitment for Junior EngineersDocument16 paginiESIC recruitment for Junior EngineersChandra SekaranÎncă nu există evaluări
- Dde Time Table - 2019 MayDocument53 paginiDde Time Table - 2019 MaySenthil KumarÎncă nu există evaluări
- Notification NLC India Limited Dy Medical Officer Pharmacist OtherDocument1 paginăNotification NLC India Limited Dy Medical Officer Pharmacist OtherSenthil KumarÎncă nu există evaluări
- Transfer & Posting of SI Order dt.31.10.18 PDFDocument1 paginăTransfer & Posting of SI Order dt.31.10.18 PDFSenthil KumarÎncă nu există evaluări
- Paramedical AdvtDocument14 paginiParamedical AdvtJohnRameshÎncă nu există evaluări
- Transfer and Posting of Police Officer & Personnel - SP (HQ) DT 18.01.19 PDFDocument2 paginiTransfer and Posting of Police Officer & Personnel - SP (HQ) DT 18.01.19 PDFSenthil KumarÎncă nu există evaluări
- Advt 012019Document4 paginiAdvt 012019AjayÎncă nu există evaluări
- Communication Letter - 13112018Document2 paginiCommunication Letter - 13112018Senthil KumarÎncă nu există evaluări
- Application For Administrative Advertisement No: RC/2018-19/33 Advt. Date: 15.10.2018Document12 paginiApplication For Administrative Advertisement No: RC/2018-19/33 Advt. Date: 15.10.2018Senthil KumarÎncă nu există evaluări
- YOGA. Physiology, Psychosomatics, Bioenergetics.Document245 paginiYOGA. Physiology, Psychosomatics, Bioenergetics.yoga_uyf95% (64)
- 4a SWDocument25 pagini4a SWSandeep SagarÎncă nu există evaluări
- Application For Administrative Advertisement No: RC/2018-19/33 Advt. Date: 15.10.2018Document12 paginiApplication For Administrative Advertisement No: RC/2018-19/33 Advt. Date: 15.10.2018Senthil KumarÎncă nu există evaluări
- Transfer & Posting of SI Order dt.31.10.18 PDFDocument1 paginăTransfer & Posting of SI Order dt.31.10.18 PDFSenthil KumarÎncă nu există evaluări
- Application For Administrative Advertisement No: RC/2018-19/33 Advt. Date: 15.10.2018Document12 paginiApplication For Administrative Advertisement No: RC/2018-19/33 Advt. Date: 15.10.2018Senthil KumarÎncă nu există evaluări
- Transfer & Posting of SI Order dt.31.10.18 PDFDocument1 paginăTransfer & Posting of SI Order dt.31.10.18 PDFSenthil KumarÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- 12 Week Duathlon Training ProgramDocument7 pagini12 Week Duathlon Training ProgramJairuz Agang-angÎncă nu există evaluări
- Why Is Keeping Active Important?Document4 paginiWhy Is Keeping Active Important?Waseem QureshiÎncă nu există evaluări
- Best Upper Body Workout RoutineDocument35 paginiBest Upper Body Workout RoutineMATHIEU95120Încă nu există evaluări
- 8-Week Dumbbell Body Weight Fusion Fat Loss ProgramDocument33 pagini8-Week Dumbbell Body Weight Fusion Fat Loss ProgramPedro Jaquez100% (1)
- Resume - Kendra 3 1Document3 paginiResume - Kendra 3 1api-269185495Încă nu există evaluări
- Personal Fitness Webquest Update 10-12-07Document16 paginiPersonal Fitness Webquest Update 10-12-07Information Point KapurthalaÎncă nu există evaluări
- Hybrid Kettlebell Strength and Conditioning Main ManualDocument28 paginiHybrid Kettlebell Strength and Conditioning Main ManualMark100% (6)
- Muscle Up Program PDFDocument3 paginiMuscle Up Program PDFjan100% (1)
- The Periodization BibleDocument41 paginiThe Periodization BibleKyle Carter100% (1)
- Fitness FirstDocument5 paginiFitness FirstvarunÎncă nu există evaluări
- Strength Training Influences on Muscle SizeDocument40 paginiStrength Training Influences on Muscle SizeromeroidasÎncă nu există evaluări
- Strength and Conditioning For Rugby League and Rugby Union Part 1Document10 paginiStrength and Conditioning For Rugby League and Rugby Union Part 1kurupirockeroÎncă nu există evaluări
- Hygiene Handbook for Housekeeping and Hairdressing StaffDocument23 paginiHygiene Handbook for Housekeeping and Hairdressing Staffdettystudent100% (1)
- Fitness Brochure 8/14Document2 paginiFitness Brochure 8/14winchesterpandrÎncă nu există evaluări
- Kemampuan Keluarga Dalam Merawat Orang Dengan Gangguan JiwaDocument7 paginiKemampuan Keluarga Dalam Merawat Orang Dengan Gangguan JiwaDian ZaizyulÎncă nu există evaluări
- Built Like A BadassDocument15 paginiBuilt Like A BadassSheldon Kranendonk100% (1)
- 30 DayDocument11 pagini30 DayEduardo Iparralde100% (1)
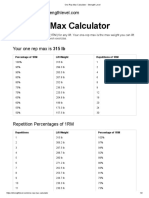
- Deadlift One Rep Max Calculator - Strength LevelDocument2 paginiDeadlift One Rep Max Calculator - Strength Leveltim winkelmanÎncă nu există evaluări
- THE ORIGINAL ALL-WEATHER TRACKSDocument9 paginiTHE ORIGINAL ALL-WEATHER TRACKSMarcelo Da Silva100% (2)
- Justin Age 13 Client Assessment MatrixDocument2 paginiJustin Age 13 Client Assessment Matrixapi-441311906Încă nu există evaluări
- The Tools You Need To Build The Body You Want: Field Manual: A Training Guide For Those With Little Time & EquipmentDocument1 paginăThe Tools You Need To Build The Body You Want: Field Manual: A Training Guide For Those With Little Time & EquipmentMario RendonÎncă nu există evaluări
- A Beginners Guide To Calisthenics 1 PDFDocument26 paginiA Beginners Guide To Calisthenics 1 PDFAnonymous eYvR9pw80% (10)
- 1607 BENCHMARK WODSDocument310 pagini1607 BENCHMARK WODSfernandocmbenedetteÎncă nu există evaluări
- Building The Monolith (KG)Document36 paginiBuilding The Monolith (KG)zenphanÎncă nu există evaluări
- Calisthenics LogDocument4 paginiCalisthenics LogWardÎncă nu există evaluări
- Effects of Speed Agility Quickness Train PDFDocument8 paginiEffects of Speed Agility Quickness Train PDFRaquel DanielÎncă nu există evaluări
- Tempo Workouts For Sprinters BlackmerDocument5 paginiTempo Workouts For Sprinters BlackmerGM RibauwÎncă nu există evaluări
- 5 Minute Fat Burning Workouts at Home - Best Exercises To Lose WeightDocument19 pagini5 Minute Fat Burning Workouts at Home - Best Exercises To Lose WeightBhupendra TyagiÎncă nu există evaluări
- 01+The+DUP+Method+Main+Manual+FINAL K2optDocument146 pagini01+The+DUP+Method+Main+Manual+FINAL K2optxaviermayÎncă nu există evaluări