S-ar putea să vă placă și
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsDe la EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsÎncă nu există evaluări
- Temporary Pacemakers-SICU's 101 PrimerDocument51 paginiTemporary Pacemakers-SICU's 101 Primerwaqas_xsÎncă nu există evaluări
- Pacing Week PresentationsDocument54 paginiPacing Week PresentationsjoejenningsÎncă nu există evaluări
- Anaesthesia Management of Patient of PacemakerDocument92 paginiAnaesthesia Management of Patient of PacemakerSiva KrishnaÎncă nu există evaluări
- ECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!De la EverandECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!Încă nu există evaluări
- ECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasDe la EverandECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasEvaluare: 5 din 5 stele5/5 (2)
- ACLS Advanced Cardiovascular Life Support Provider Manual 2023De la EverandACLS Advanced Cardiovascular Life Support Provider Manual 2023Încă nu există evaluări
- Basic EP 01Document53 paginiBasic EP 01Hany100% (2)
- Cardiac Pacing (Landes Bioscience Vademecum) PDFDocument155 paginiCardiac Pacing (Landes Bioscience Vademecum) PDFConstantinescu RasvanÎncă nu există evaluări
- Eps Course Basic ElectrophysiologyDocument23 paginiEps Course Basic Electrophysiologytisya_endut2081100% (1)
- Ventricular Arrhythmias: Robert J. Hariman, MDDocument51 paginiVentricular Arrhythmias: Robert J. Hariman, MDusfcardsÎncă nu există evaluări
- Pediatric Cardiac Arrest AlgorithmDocument27 paginiPediatric Cardiac Arrest AlgorithmLinna AndrianiÎncă nu există evaluări
- European Society of Cardiology-Esc Guidelines Desk Reference 2011 - Compendi PDFDocument379 paginiEuropean Society of Cardiology-Esc Guidelines Desk Reference 2011 - Compendi PDFAsri SetiawanÎncă nu există evaluări
- 7.5.2016 IBHRE CCDS Physician 17 - FINAL PDFDocument8 pagini7.5.2016 IBHRE CCDS Physician 17 - FINAL PDFAlexander Edo TondasÎncă nu există evaluări
- 12 Lead InterpretationDocument33 pagini12 Lead InterpretationTodd CoxÎncă nu există evaluări
- Basics & Timing-PmDocument120 paginiBasics & Timing-PmWiwik Puji Lestari100% (1)
- Basic and Bedside ElectrocardiographyDocument464 paginiBasic and Bedside ElectrocardiographyBimo Panji Kumoro100% (2)
- Podrid S Real-World ECGs Volume 5B - Narrow and Wide Complex Tachyarrhythmias and Abberation Practice Cases 2016Document336 paginiPodrid S Real-World ECGs Volume 5B - Narrow and Wide Complex Tachyarrhythmias and Abberation Practice Cases 2016Akama BetaÎncă nu există evaluări
- Hemodynamic Drug InfusionsDocument45 paginiHemodynamic Drug InfusionsDawit MucheÎncă nu există evaluări
- Hemodynamics in The Cath Lab 2Document45 paginiHemodynamics in The Cath Lab 2usfcards100% (1)
- @ebookmedicin Cardiology Clinics February 2017Document19 pagini@ebookmedicin Cardiology Clinics February 2017mulyadiÎncă nu există evaluări
- Basic ElectrophysiologyDocument46 paginiBasic Electrophysiologyiin setiyanaÎncă nu există evaluări
- EpalsDocument3 paginiEpalsmkemnitzwcsÎncă nu există evaluări
- Geriatric NeuroanesthesiDocument333 paginiGeriatric NeuroanesthesiAdi Wira HadiÎncă nu există evaluări
- Intro To EPDocument48 paginiIntro To EPusfcards100% (2)
- Cardiology 2023 FinalDocument208 paginiCardiology 2023 FinalBelinda ELISHA100% (1)
- 439 3 Electrophysiology & ECG BasicsDocument34 pagini439 3 Electrophysiology & ECG BasicsjpoutreÎncă nu există evaluări
- Antrim ED Handbook 2019Document238 paginiAntrim ED Handbook 2019Chris Jardine LiÎncă nu există evaluări
- ICD Troubleshooting (Heart)Document13 paginiICD Troubleshooting (Heart)Prem KumarÎncă nu există evaluări
- Sinus Node DysfunctionDocument11 paginiSinus Node DysfunctionVasishta Nadella100% (1)
- ECG IMM 2020.docx.2Document25 paginiECG IMM 2020.docx.2Abdul QuyyumÎncă nu există evaluări
- Pocket Tutor ECG Interpretation PDFDocument165 paginiPocket Tutor ECG Interpretation PDFasri100% (3)
- PALS Pulseless Arrest Algorithm: Kleinman, M. E. Et Al. Circulation 2010 122:S876-S908Document3 paginiPALS Pulseless Arrest Algorithm: Kleinman, M. E. Et Al. Circulation 2010 122:S876-S908YONE LENINÎncă nu există evaluări
- ECMO Learning PackageDocument35 paginiECMO Learning PackageAndrewÎncă nu există evaluări
- AGT Applied Anatomy Notes1.1Document69 paginiAGT Applied Anatomy Notes1.1Akshay ChauhanÎncă nu există evaluări
- Global Longitudinal StrainDocument7 paginiGlobal Longitudinal StrainBinod KumarÎncă nu există evaluări
- Bedside Approach To Electrocardiography JapyeeDocument188 paginiBedside Approach To Electrocardiography JapyeeRichard MelialaÎncă nu există evaluări
- Arterial Line Waveform Interpretation UHL Childrens Intensive Care GuidelineDocument5 paginiArterial Line Waveform Interpretation UHL Childrens Intensive Care GuidelineDhony100% (1)
- ECMO Monitoring - PediatrikDocument24 paginiECMO Monitoring - PediatrikIsran IsRanÎncă nu există evaluări
- Cardiac PacingDocument89 paginiCardiac Pacingsandwhale056Încă nu există evaluări
- Modes of Cardiac Pacing, Nomenclature and SelectionDocument32 paginiModes of Cardiac Pacing, Nomenclature and SelectionMohammad AlmuhaiminÎncă nu există evaluări
- Practical Guide For The Students Version 2.0Document906 paginiPractical Guide For The Students Version 2.0tejuteju06750% (2)
- Cardiac NotesDocument24 paginiCardiac NotesYary MayorÎncă nu există evaluări
- The History of Perfusion PumpsDocument28 paginiThe History of Perfusion PumpsMiguel Angel CastroÎncă nu există evaluări
- Aortic Stenosis AmendillaDocument31 paginiAortic Stenosis AmendillaVadim BursacovschiÎncă nu există evaluări
- Cardiac Electrophysiology Technician or Electrophysiology TechniDocument2 paginiCardiac Electrophysiology Technician or Electrophysiology Techniapi-78900391Încă nu există evaluări
- Cardiac Resynchronization Therapy (Sep 19 2007) - (1841846376) - (CRC Press)Document337 paginiCardiac Resynchronization Therapy (Sep 19 2007) - (1841846376) - (CRC Press)Morozovschi VitalieÎncă nu există evaluări
- Approach To TruamaDocument29 paginiApproach To TruamaIbsa ShumaÎncă nu există evaluări
- Advanced ICD Troubleshooting Part 2 PACE 2006 PDFDocument27 paginiAdvanced ICD Troubleshooting Part 2 PACE 2006 PDFSrajner PéterÎncă nu există evaluări
- Mechanical Circulatory SupportDocument241 paginiMechanical Circulatory Supporthamida100% (1)
- Pacemaker Learning Package: Paula Nekic CNE Liverpool Hospital ICU January 2016Document46 paginiPacemaker Learning Package: Paula Nekic CNE Liverpool Hospital ICU January 2016Zahangir Kabir AshikÎncă nu există evaluări
- Percutaneous InterventionsDocument55 paginiPercutaneous InterventionsShannon Bellamy-FoggÎncă nu există evaluări
- Strain ImagingDocument54 paginiStrain ImagingKhalid Mehdi100% (1)
- Ecmo and SepsisDocument37 paginiEcmo and SepsisMarckus BrodyÎncă nu există evaluări
- Read ECGDocument128 paginiRead ECGrehmatakuÎncă nu există evaluări
- Braunwald Lecture Series #2Document33 paginiBraunwald Lecture Series #2usfcards100% (2)
- Cardiac Pacing& CRT. ESC Pocket Guidelines 2021. Dr. Amro ShakerDocument68 paginiCardiac Pacing& CRT. ESC Pocket Guidelines 2021. Dr. Amro Shakermohammed salahÎncă nu există evaluări
- Heart Failure 2022-2023 First Semester - FinalDocument69 paginiHeart Failure 2022-2023 First Semester - FinalAlaa zayadnehÎncă nu există evaluări
- Electrical Activity of The HeartDocument156 paginiElectrical Activity of The HeartNIRANJANA SHALINIÎncă nu există evaluări
- Surgical Management of Ischemic Heart Disease - An UpdateDocument48 paginiSurgical Management of Ischemic Heart Disease - An UpdateRezwanul Hoque BulbulÎncă nu există evaluări
- Mitral Valve Replacement With Preservation of Valve ApparatusDocument20 paginiMitral Valve Replacement With Preservation of Valve ApparatusRezwanul Hoque BulbulÎncă nu există evaluări
- Tetralogy of FallotDocument73 paginiTetralogy of FallotRezwanul Hoque Bulbul0% (1)
- Cardiac Anatomy For SurgeonsDocument49 paginiCardiac Anatomy For SurgeonsRezwanul Hoque BulbulÎncă nu există evaluări
- Dr. Md. Rezwanul Hoque: Associate Professor Department of Cardiac Surgery BSMMU, Dhaka, BangladeshDocument48 paginiDr. Md. Rezwanul Hoque: Associate Professor Department of Cardiac Surgery BSMMU, Dhaka, BangladeshRezwanul Hoque Bulbul100% (1)
- Myocardial Protection - An UpdateDocument67 paginiMyocardial Protection - An UpdateRezwanul Hoque Bulbul100% (5)
- Mitral Valve Diseases & ManagementDocument74 paginiMitral Valve Diseases & ManagementRezwanul Hoque BulbulÎncă nu există evaluări
- Cardiac Tamponade and ManagementDocument42 paginiCardiac Tamponade and ManagementRezwanul Hoque Bulbul100% (2)
- Ventricular Septal Defect-OverviewDocument42 paginiVentricular Septal Defect-OverviewRezwanul Hoque Bulbul100% (1)
- Rheumatic Heart DiseaseDocument39 paginiRheumatic Heart DiseaseRezwanul Hoque Bulbul100% (1)
- Postoperative Sternal Wound Complication & ManagementDocument37 paginiPostoperative Sternal Wound Complication & ManagementRezwanul Hoque BulbulÎncă nu există evaluări
- Aortic Valve SurgeryDocument73 paginiAortic Valve SurgeryRezwanul Hoque Bulbul100% (2)
- Cardiopulmonary by PassDocument62 paginiCardiopulmonary by PassRezwanul Hoque Bulbul100% (1)
- Surgical Restoration of Ventricular FunctionDocument40 paginiSurgical Restoration of Ventricular FunctionRezwanul Hoque BulbulÎncă nu există evaluări
- Mechanical Ventilation & Respiratory Support TherapyDocument42 paginiMechanical Ventilation & Respiratory Support TherapyRezwanul Hoque Bulbul100% (2)
- Cell Membrane Structure and FunctionDocument10 paginiCell Membrane Structure and FunctionkyleeebooggÎncă nu există evaluări
- Seeley's Chapter 8 Nervous SystemDocument100 paginiSeeley's Chapter 8 Nervous SystemChristine Tapawan88% (8)
- Botulinum Toxins in Clinical Aesthetic Practice 3rd Edition Volume Two - Functional Anatomy and Injection Techniques 2018Document237 paginiBotulinum Toxins in Clinical Aesthetic Practice 3rd Edition Volume Two - Functional Anatomy and Injection Techniques 2018Dogukan Demir75% (4)
- PeriodisationDocument6 paginiPeriodisationZahra SativaniÎncă nu există evaluări
- Cat Muscles and O.I.A.: Body Region Muscle Origin Insertion ActionDocument5 paginiCat Muscles and O.I.A.: Body Region Muscle Origin Insertion ActioneumarasiganÎncă nu există evaluări
- Voice Disorder 2011 PDFDocument6 paginiVoice Disorder 2011 PDFfaidgustisyarifÎncă nu există evaluări
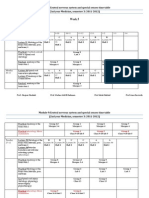
- Week 5: Module 9:central Nervous System and Special Senses Time Table (2nd Year Medicine, Semester 3: 2011-2012)Document17 paginiWeek 5: Module 9:central Nervous System and Special Senses Time Table (2nd Year Medicine, Semester 3: 2011-2012)Hairul AnuarÎncă nu există evaluări
- Transfer To Definitive Care EcaDocument40 paginiTransfer To Definitive Care EcaFahrurido Kusbari100% (1)
- Bio Quiz BeeDocument2 paginiBio Quiz BeeRuchi Briam James LagitnayÎncă nu există evaluări
- College of Nursing INUR3302: Nursing Process and Basic Health Assessment Monitoring Blood PressureDocument4 paginiCollege of Nursing INUR3302: Nursing Process and Basic Health Assessment Monitoring Blood Pressuregladz25Încă nu există evaluări
- AnatomyDocument8 paginiAnatomyRobbie WoelkersÎncă nu există evaluări
- Rula SheetDocument2 paginiRula SheetCarl Christian CabelloÎncă nu există evaluări
- Kara Gianni 2015Document7 paginiKara Gianni 2015devaaÎncă nu există evaluări
- Bioenergetics 1Document30 paginiBioenergetics 1suni alditaÎncă nu există evaluări
- The Scarecrow Queen (Excerpt)Document36 paginiThe Scarecrow Queen (Excerpt)I Read YA50% (2)
- Gangguan Dan Keseimbangan Cairan Dan ElektrolitDocument37 paginiGangguan Dan Keseimbangan Cairan Dan ElektrolitFyana PutriÎncă nu există evaluări
- Ineffective Airway Clearance NCPDocument1 paginăIneffective Airway Clearance NCPBenz ParCoÎncă nu există evaluări
- Lecture 3 Innate ImmunityDocument26 paginiLecture 3 Innate ImmunitytimcarasÎncă nu există evaluări
- Acute Effects of Tissue Flossing On Ankle Range of Motion and Tensiomyography Parameter - Matjaz Vogrin 2021Document8 paginiAcute Effects of Tissue Flossing On Ankle Range of Motion and Tensiomyography Parameter - Matjaz Vogrin 2021YngaMarquezJairÎncă nu există evaluări
- Dr. Vijetha Shenoy Belle Associate Professor & In-Charge Clinical Biochemistry Laboratory Department of Biochemistry KMC ManipalDocument53 paginiDr. Vijetha Shenoy Belle Associate Professor & In-Charge Clinical Biochemistry Laboratory Department of Biochemistry KMC ManipalKavya GaneshÎncă nu există evaluări
- Abbot, Diabetes ManagementDocument1 paginăAbbot, Diabetes ManagementMelissa Grace DizonÎncă nu există evaluări
- Steps HemodialysisDocument3 paginiSteps HemodialysisCes LoÎncă nu există evaluări
- Excretory ReviewDocument2 paginiExcretory Reviewapi-240662720Încă nu există evaluări
- BMJ - Hypovolemic ShockDocument5 paginiBMJ - Hypovolemic ShockSamer Darwiche Yasiin100% (1)
- CropSci101 Module 3Document11 paginiCropSci101 Module 3Jetro Neil GapasinÎncă nu există evaluări
- (Jagaran Josh) Science PDFDocument136 pagini(Jagaran Josh) Science PDFPiyush KumarÎncă nu există evaluări
- Agriculture& Horticulture Conference BrochureDocument6 paginiAgriculture& Horticulture Conference BrochureAgriculture conferenceÎncă nu există evaluări
- Extroverts (Also Spelled Extraverts: ExtroversionDocument8 paginiExtroverts (Also Spelled Extraverts: Extroversionrams4u_001Încă nu există evaluări
- Pop Gen Practice Problems SP 14Document4 paginiPop Gen Practice Problems SP 14Pia ViloriaÎncă nu există evaluări
- Nutrisi Cedera KepalaDocument46 paginiNutrisi Cedera Kepalatsunami555Încă nu există evaluări