S-ar putea să vă placă și
- Spinal Cord Deseases: Na ShaoDocument38 paginiSpinal Cord Deseases: Na ShaoArvindhanÎncă nu există evaluări
- Peripheral Neuropathies FOR CLASSIFICATIONDocument9 paginiPeripheral Neuropathies FOR CLASSIFICATIONAnnie JoÎncă nu există evaluări
- Guillain-Barré Syndrome OtrDocument5 paginiGuillain-Barré Syndrome OtrMariam PlataÎncă nu există evaluări
- Cwu 2Document31 paginiCwu 2Hakimah K. SuhaimiÎncă nu există evaluări
- Fees Structure For Government Sponsored (KUCCPS) Students: University of Eastern Africa, BaratonDocument3 paginiFees Structure For Government Sponsored (KUCCPS) Students: University of Eastern Africa, BaratonGiddy LerionkaÎncă nu există evaluări
- Acute ScrotumDocument38 paginiAcute ScrotumShochibul KahfiÎncă nu există evaluări
- 4.cardivascular System ExaminationDocument60 pagini4.cardivascular System ExaminationElvisÎncă nu există evaluări
- Stroke & Hemiplegia LocalizationDocument54 paginiStroke & Hemiplegia LocalizationVasu PottabatthiniÎncă nu există evaluări
- Osteomyelitis Metabolic Bone DisordersDocument36 paginiOsteomyelitis Metabolic Bone DisordersVishesh JainÎncă nu există evaluări
- Peripheral Artery Occlusive Disease: What To Do About Intermittent Claudication??Document46 paginiPeripheral Artery Occlusive Disease: What To Do About Intermittent Claudication??Dzariyat_Azhar_9277100% (1)
- College of Medicine & Health SciencesDocument56 paginiCollege of Medicine & Health SciencesMebratu DemessÎncă nu există evaluări
- 30-99!90!1619-Rev.0-Method Statement For Pipeline WeldingDocument21 pagini30-99!90!1619-Rev.0-Method Statement For Pipeline WeldingkilioÎncă nu există evaluări
- Nov 2017 Infantile Spasms WebinarDocument22 paginiNov 2017 Infantile Spasms WebinartetiÎncă nu există evaluări
- Iso 16399-2014-05Document52 paginiIso 16399-2014-05nadim100% (1)
- Rad. Patho - Skeletal SystemDocument77 paginiRad. Patho - Skeletal SystemNikko L. Pescueso100% (1)
- ASTRO UserguideDocument1.054 paginiASTRO UserguideMarwan Ahmed100% (1)
- Juvenile Idiopathic ArthritisDocument4 paginiJuvenile Idiopathic ArthritisAmmarÎncă nu există evaluări
- Case Write-Up - Obstetrics - Gestational Diabetes MellitusDocument17 paginiCase Write-Up - Obstetrics - Gestational Diabetes MellitusHakimah K. Suhaimi89% (38)
- K32 - Pathology of Bone (Dr. Dody)Document60 paginiK32 - Pathology of Bone (Dr. Dody)faris100% (1)
- Osteogenesis Imperfecta Power PointDocument29 paginiOsteogenesis Imperfecta Power PointJonathan Jeffry Pratama100% (1)
- Spinal Cord Injury, DisordersDocument54 paginiSpinal Cord Injury, DisordersChananÎncă nu există evaluări
- Stroke Rsu Banjar: DR Fuad Hanif Sps M.KesDocument80 paginiStroke Rsu Banjar: DR Fuad Hanif Sps M.KesRobert HarrisÎncă nu există evaluări
- Singular and Plural NounsDocument3 paginiSingular and Plural NounsJosé BulquesÎncă nu există evaluări
- N C C N D: Ursing ARE OF Lients With Eurologic IsordersDocument96 paginiN C C N D: Ursing ARE OF Lients With Eurologic IsordersMatt Lao DionelaÎncă nu există evaluări
- Weakness B WDocument62 paginiWeakness B WKhan A RehÎncă nu există evaluări
- Seminar 5 - Thyroid Disease in PregnancyDocument25 paginiSeminar 5 - Thyroid Disease in PregnancyHakimah K. SuhaimiÎncă nu există evaluări
- XDM-300 IMM ETSI B00 8.2.1-8.2.2 enDocument386 paginiXDM-300 IMM ETSI B00 8.2.1-8.2.2 enHipolitomvn100% (1)
- Clinical Features of Amyotrophic Lateral Sclerosis and Other Forms of Motor Neuron Disease UpToDate PDFDocument21 paginiClinical Features of Amyotrophic Lateral Sclerosis and Other Forms of Motor Neuron Disease UpToDate PDFThái BảoÎncă nu există evaluări
- Duchenne Muscular Dystrophy: An OverviewDocument32 paginiDuchenne Muscular Dystrophy: An OverviewMr.P.Ramesh, Faculty of Physiotherapy, SRUÎncă nu există evaluări
- LATHYRISM AND PHOTOSENSiTIZATIONDocument33 paginiLATHYRISM AND PHOTOSENSiTIZATIONSunilÎncă nu există evaluări
- Skin CancerDocument5 paginiSkin CancerEl FaroukÎncă nu există evaluări
- Acute Flaccid ParalysisDocument4 paginiAcute Flaccid ParalysisZharah RuzÎncă nu există evaluări
- Pediatric Department Faculty of MedicineDocument100 paginiPediatric Department Faculty of MedicineIrfanÎncă nu există evaluări
- Craniovertebral Junction Anatomy & RadiologyDocument130 paginiCraniovertebral Junction Anatomy & Radiologydrarunrao100% (1)
- Dr Saif Darif's Guide to Rheumatic DiseasesDocument30 paginiDr Saif Darif's Guide to Rheumatic DiseasesMohamed A SalehÎncă nu există evaluări
- Localisation of Spinal Cord LesionsDocument218 paginiLocalisation of Spinal Cord LesionsGoh Sheen YeeÎncă nu există evaluări
- Birth DefectsDocument36 paginiBirth DefectsSohera NadeemÎncă nu există evaluări
- Alopecia AreataDocument71 paginiAlopecia AreatadrbhaveshpÎncă nu există evaluări
- Alterations in Neurological, Mental Health and Cognition FunctionsDocument133 paginiAlterations in Neurological, Mental Health and Cognition Functionsthe4gameÎncă nu există evaluări
- AthetosisDocument2 paginiAthetosisapi-19973386Încă nu există evaluări
- ACHONDROPLASIADocument18 paginiACHONDROPLASIAJennie Mayaute AllcaÎncă nu există evaluări
- Neuromuskular: Dr. Ketut Widyastuti, SP.SDocument81 paginiNeuromuskular: Dr. Ketut Widyastuti, SP.SMirae RoseÎncă nu există evaluări
- Seizures and Epilepsy: Haining Li General Hospital of Ningxia Medical UniversityDocument50 paginiSeizures and Epilepsy: Haining Li General Hospital of Ningxia Medical UniversityArvindhanÎncă nu există evaluări
- Achondroplasia GuideDocument30 paginiAchondroplasia GuideRayyan HidayatÎncă nu există evaluări
- Cerebellar Disorders: Dr. Mohamed Nasreldin HamdoonDocument14 paginiCerebellar Disorders: Dr. Mohamed Nasreldin HamdoonMohamed Nasreldin HamdoonÎncă nu există evaluări
- Glycogen Storage Disease, Type II (Pompe Disease) : BackgroundDocument7 paginiGlycogen Storage Disease, Type II (Pompe Disease) : Background201111000Încă nu există evaluări
- Lymphadenopathy in Children: Causes, Evaluation and ManagementDocument34 paginiLymphadenopathy in Children: Causes, Evaluation and ManagementAlchemyAdvisory100% (1)
- Motor Neuron Disease: Amyotrophic Lateral Sclerosis (ALS)Document2 paginiMotor Neuron Disease: Amyotrophic Lateral Sclerosis (ALS)james cordenÎncă nu există evaluări
- HEMOPHILIADocument27 paginiHEMOPHILIAr DÎncă nu există evaluări
- Understanding Bell's Palsy: Causes, Symptoms and TreatmentDocument25 paginiUnderstanding Bell's Palsy: Causes, Symptoms and TreatmentNovita Indah YantiÎncă nu există evaluări
- Type Gene Description: Becker's Muscular Dystrophy Duchenne Muscular Dystrophy DystrophinDocument4 paginiType Gene Description: Becker's Muscular Dystrophy Duchenne Muscular Dystrophy DystrophinNikhilKapoorÎncă nu există evaluări
- Frozen ShoulderDocument29 paginiFrozen ShoulderMárcia PatríciaÎncă nu există evaluări
- Osteogenesis ImperfectaDocument6 paginiOsteogenesis ImperfectaWirahadi SanjayaÎncă nu există evaluări
- Legg-Calvé-Perthes Disease - An Overview With Recent LiteratureDocument10 paginiLegg-Calvé-Perthes Disease - An Overview With Recent LiteratureFranz BlacuttÎncă nu există evaluări
- Cerebral Palsy: Kalaiselvi. P Assistant Professor Srinivas Institute of Nursing SciencesDocument41 paginiCerebral Palsy: Kalaiselvi. P Assistant Professor Srinivas Institute of Nursing SciencesKarthikeyan Guru100% (1)
- Chapter # 4: Physical Assessment As A Screening ToolDocument89 paginiChapter # 4: Physical Assessment As A Screening Toolmuhammad awaisÎncă nu există evaluări
- BronchiolitisDocument12 paginiBronchiolitisEz BallÎncă nu există evaluări
- Nephrotic Syndrome and Glomerulonephritis GuideDocument40 paginiNephrotic Syndrome and Glomerulonephritis GuidesangheetaÎncă nu există evaluări
- CHP 11 Cerebral Air EmbolismDocument8 paginiCHP 11 Cerebral Air EmbolismSrinivas GokulnathÎncă nu există evaluări
- Seizures and EpilepsyDocument64 paginiSeizures and EpilepsyrajaeasÎncă nu există evaluări
- Normal Pressure HydrocephalusDocument59 paginiNormal Pressure Hydrocephalusrys239Încă nu există evaluări
- Getahun Mengistu, MD, MSC, Internist, Neurologist & Specialist in Headache Medicine, Department of Neurology, AAU-MFDocument85 paginiGetahun Mengistu, MD, MSC, Internist, Neurologist & Specialist in Headache Medicine, Department of Neurology, AAU-MFashuÎncă nu există evaluări
- KEPILEPSY PresentationDocument39 paginiKEPILEPSY PresentationalotfyaÎncă nu există evaluări
- Name: Urwa Hafeez Roll No.: BZOF17M037 Topic:: Hypersensitivity Type-IIIDocument30 paginiName: Urwa Hafeez Roll No.: BZOF17M037 Topic:: Hypersensitivity Type-IIIurwa hafeezÎncă nu există evaluări
- Neurological Exam LectureDocument114 paginiNeurological Exam LectureLolla SinwarÎncă nu există evaluări
- Cerebral Malaria (CM) Prof. WBP Matuja, MuhasDocument20 paginiCerebral Malaria (CM) Prof. WBP Matuja, MuhasAnonymous TCZf45C10Încă nu există evaluări
- Approach To Viral Hepatitis andDocument38 paginiApproach To Viral Hepatitis andVijay ShankarÎncă nu există evaluări
- Buerger'S Disease: By: Ns. Yulia Prodi S1 Keperawatan Stikes Kepanjen 2014Document18 paginiBuerger'S Disease: By: Ns. Yulia Prodi S1 Keperawatan Stikes Kepanjen 2014atik mayasariÎncă nu există evaluări
- Synovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandSynovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Cme Acs 2. Stemi (Izzah)Document36 paginiCme Acs 2. Stemi (Izzah)Hakimah K. SuhaimiÎncă nu există evaluări
- Cwu 1 OrthoDocument14 paginiCwu 1 OrthoHakimah K. Suhaimi100% (1)
- Stroke UpdatesDocument72 paginiStroke UpdatesHakimah K. SuhaimiÎncă nu există evaluări
- Urology Case Presentation - Scrotal Mass 1Document20 paginiUrology Case Presentation - Scrotal Mass 1Hakimah K. Suhaimi100% (1)
- Cme Acs 1. Ua, Nstemi (Hakimah)Document53 paginiCme Acs 1. Ua, Nstemi (Hakimah)Hakimah K. SuhaimiÎncă nu există evaluări
- Workshop-Scrotal Mass-Ensuring A Correct DXDocument3 paginiWorkshop-Scrotal Mass-Ensuring A Correct DXHakimah K. SuhaimiÎncă nu există evaluări
- Multiple SCL AAMDocument58 paginiMultiple SCL AAMHakimah K. SuhaimiÎncă nu există evaluări
- 2 - Psychiatric Emergencies - Violence (Hakimah)Document14 pagini2 - Psychiatric Emergencies - Violence (Hakimah)Hakimah K. SuhaimiÎncă nu există evaluări
- FTP YDocument11 paginiFTP YnetifarhatiiÎncă nu există evaluări
- Saturday Teach inDocument1 paginăSaturday Teach inHakimah K. SuhaimiÎncă nu există evaluări
- 2 - Lens and CataractDocument24 pagini2 - Lens and CataractHakimah K. SuhaimiÎncă nu există evaluări
- 3) Painless & Solid Scrotal Swellings (Reviewed)Document13 pagini3) Painless & Solid Scrotal Swellings (Reviewed)Hakimah K. SuhaimiÎncă nu există evaluări
- Dementia Vs Delirium Acad of Med, 21st AprilDocument106 paginiDementia Vs Delirium Acad of Med, 21st AprilHakimah K. SuhaimiÎncă nu există evaluări
- THE CALL (Part 1)Document7 paginiTHE CALL (Part 1)Hakimah K. SuhaimiÎncă nu există evaluări
- Seminar Acute Poststreptococcal GlomerulonephritisDocument33 paginiSeminar Acute Poststreptococcal GlomerulonephritisHakimah K. SuhaimiÎncă nu există evaluări
- Hakimah's - Edited Q12 TDocument7 paginiHakimah's - Edited Q12 THakimah K. SuhaimiÎncă nu există evaluări
- Seminar 5 - Urinary Tract Infection in PregnancyDocument33 paginiSeminar 5 - Urinary Tract Infection in PregnancyHakimah K. Suhaimi100% (1)
- Hakimah's - Edited Q12 ChiDocument15 paginiHakimah's - Edited Q12 ChiHakimah K. SuhaimiÎncă nu există evaluări
- Important Qs in Pediatrics HX TakingDocument2 paginiImportant Qs in Pediatrics HX TakingHakimah K. SuhaimiÎncă nu există evaluări
- Fetal MonitoringDocument38 paginiFetal MonitoringHakimah K. SuhaimiÎncă nu există evaluări
- Seminar 5 - Systhemic Lupus Erythematosus in PregnancyDocument12 paginiSeminar 5 - Systhemic Lupus Erythematosus in PregnancyHakimah K. SuhaimiÎncă nu există evaluări
- Seminar Acute Post Streptococcal Glomerulonephritis (Edited Version)Document35 paginiSeminar Acute Post Streptococcal Glomerulonephritis (Edited Version)Hakimah K. SuhaimiÎncă nu există evaluări
- Seminar 5 - RH Iso Immunization in PregnancyDocument23 paginiSeminar 5 - RH Iso Immunization in PregnancyHakimah K. SuhaimiÎncă nu există evaluări
- Physiology of The Menstrual Cycle: by Zafirah Hani Bte Ramli 2008289204Document64 paginiPhysiology of The Menstrual Cycle: by Zafirah Hani Bte Ramli 2008289204dr_aleen89Încă nu există evaluări
- Seminar 5 - DM in PregnancyDocument19 paginiSeminar 5 - DM in PregnancyHakimah K. SuhaimiÎncă nu există evaluări
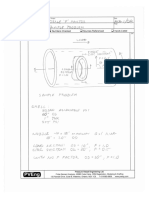
- FRP/HDPE septic tank specificationDocument2 paginiFRP/HDPE septic tank specificationpeakfortuneÎncă nu există evaluări
- Nidhi Investment Consultant: Magic Mix Illustration For Mr. AB Prafulbhai (Age 18)Document2 paginiNidhi Investment Consultant: Magic Mix Illustration For Mr. AB Prafulbhai (Age 18)jdchandrapal4980Încă nu există evaluări
- Building MassingDocument6 paginiBuilding MassingJohn AmirÎncă nu există evaluări
- Explosive Loading of Engineering Structures PDFDocument2 paginiExplosive Loading of Engineering Structures PDFBillÎncă nu există evaluări
- Data Structures LightHall ClassDocument43 paginiData Structures LightHall ClassIwuchukwu ChiomaÎncă nu există evaluări
- Introduction To South Korean History, Cultures, Traditions, & BeliefsDocument8 paginiIntroduction To South Korean History, Cultures, Traditions, & BeliefsKatriceÎncă nu există evaluări
- Sheet Metal FormingDocument13 paginiSheet Metal FormingFranklin SilvaÎncă nu există evaluări
- CM - Scope of ServicesDocument3 paginiCM - Scope of ServicesMelvin MagbanuaÎncă nu există evaluări
- Lab 1 Boys CalorimeterDocument11 paginiLab 1 Boys CalorimeterHafizszul Feyzul100% (1)
- Dxgbvi Abdor Rahim OsmanmrDocument1 paginăDxgbvi Abdor Rahim OsmanmrSakhipur TravelsÎncă nu există evaluări
- DRUG LISTDocument45 paginiDRUG LISTAmitKumarÎncă nu există evaluări
- Securifire 1000-ExtractedDocument2 paginiSecurifire 1000-ExtractedWilkeey EstrellanesÎncă nu există evaluări
- Calculate Capacity of Room Air Conditioner: Room Detail Unit Electrical Appliances in The RoomDocument2 paginiCalculate Capacity of Room Air Conditioner: Room Detail Unit Electrical Appliances in The Roomzmei23Încă nu există evaluări
- Reasons for Conducting Qualitative ResearchDocument12 paginiReasons for Conducting Qualitative ResearchMa. Rhona Faye MedesÎncă nu există evaluări
- Nozzle F Factor CalculationsDocument5 paginiNozzle F Factor CalculationsSivateja NallamothuÎncă nu există evaluări
- New Directions Formative TestDocument1 paginăNew Directions Formative TestAnonymous xGQcti3qK100% (1)
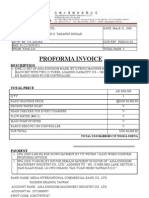
- Proforma Invoice: DescriptionDocument3 paginiProforma Invoice: Descriptionanon-690278Încă nu există evaluări
- Communication Networks Chapter 1 SolutionsDocument10 paginiCommunication Networks Chapter 1 SolutionsJ PrakashÎncă nu există evaluări
- DesignWS P1 PDFDocument673 paginiDesignWS P1 PDFcaubehamchoi6328Încă nu există evaluări
- Brief Cop27 Outcomes and Cop28 EngDocument24 paginiBrief Cop27 Outcomes and Cop28 EngVasundhara SaxenaÎncă nu există evaluări
- Water 07 02314Document36 paginiWater 07 02314Satyajit ShindeÎncă nu există evaluări
- Linear Circuit Analysis (ELEN-1100) : Lecture # 13: More On Mesh Current AnalysisDocument11 paginiLinear Circuit Analysis (ELEN-1100) : Lecture # 13: More On Mesh Current AnalysisPhD EEÎncă nu există evaluări
- Bylaw 16232 High Park RezoningDocument9 paginiBylaw 16232 High Park RezoningJamie_PostÎncă nu există evaluări
- Rapid ECG Interpretation Skills ChallengeDocument91 paginiRapid ECG Interpretation Skills ChallengeMiguel LizarragaÎncă nu există evaluări