S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- ABO Blood Group SystemDocument61 paginiABO Blood Group Systemmail2jackal50% (2)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Symptoms of Low PotassiumDocument3 paginiSymptoms of Low PotassiumCharlene Mae Calanoy100% (1)
- TCM Patent-Study Guide - FinalDocument9 paginiTCM Patent-Study Guide - FinalpranajiÎncă nu există evaluări
- Developing Biocompatibility For Medical DevicesDocument30 paginiDeveloping Biocompatibility For Medical DevicesNagula Naresh100% (1)
- დ მიქელაძის-ბიოქიმიაDocument201 paginiდ მიქელაძის-ბიოქიმიაJuli JulianaÎncă nu există evaluări
- ContactDocument65 paginiContactKhun Leang ChhunÎncă nu există evaluări
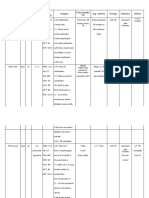
- Patients Age Sex Imagery Dig Method Therapy Outcome Others Clinical Finding Lab Finding Extra-Hepatic TBDocument9 paginiPatients Age Sex Imagery Dig Method Therapy Outcome Others Clinical Finding Lab Finding Extra-Hepatic TBkhunleangchhunÎncă nu există evaluări
- ContactDocument65 paginiContactKhun Leang ChhunÎncă nu există evaluări
- Hepatic Tuberculosis (New)Document23 paginiHepatic Tuberculosis (New)khunleangchhun0% (1)
- A Diagnostic ConundrumDocument3 paginiA Diagnostic ConundrumkhunleangchhunÎncă nu există evaluări
- Diagnosis and Management of Acute Rheumatic Fever and Rheumatic Heart Disease in AustraliaDocument100 paginiDiagnosis and Management of Acute Rheumatic Fever and Rheumatic Heart Disease in AustraliakhunleangchhunÎncă nu există evaluări
- Artikel Bahasa Inggris (Farmasi)Document3 paginiArtikel Bahasa Inggris (Farmasi)Nadia Putri AuliaÎncă nu există evaluări
- Greyson 2019Document10 paginiGreyson 2019Ziha Zia Leonita FauziÎncă nu există evaluări
- Autism AlarmDocument2 paginiAutism AlarmUmair KaziÎncă nu există evaluări
- Neurogenic Fever After Acute Traumatic Spinal Cord Injury: A Qualitative Systematic ReviewDocument8 paginiNeurogenic Fever After Acute Traumatic Spinal Cord Injury: A Qualitative Systematic Reviewreha89_drpkukraÎncă nu există evaluări
- Managing Pain After AppendectomyDocument2 paginiManaging Pain After AppendectomyChatoh SanaoÎncă nu există evaluări
- Capalbo A Et Al 2023 On The Reproductive Capabilities of Aneuploid Human Preimplantation EmbryosDocument10 paginiCapalbo A Et Al 2023 On The Reproductive Capabilities of Aneuploid Human Preimplantation EmbryosJorge Alberto Salazar CartinÎncă nu există evaluări
- Name_Naw Aung_La Mai Patient Focused ProceduresDocument2 paginiName_Naw Aung_La Mai Patient Focused ProceduresEileenÎncă nu există evaluări
- Leucorrhea KnowledgeDocument3 paginiLeucorrhea KnowledgeAnamika ChoudharyÎncă nu există evaluări
- Gingival Periodontal IndexDocument23 paginiGingival Periodontal Indexxodia_04100% (3)
- Daftar PustakaDocument6 paginiDaftar PustakaChintiaÎncă nu există evaluări
- Jeyaraj Jeeva's Series of Expected Questions Jeyaraj Jeeva's Series of Expected QuestionsDocument8 paginiJeyaraj Jeeva's Series of Expected Questions Jeyaraj Jeeva's Series of Expected QuestionsruchikaÎncă nu există evaluări
- 10 Must Know Factors of OcclusionDocument2 pagini10 Must Know Factors of OcclusionGreg Sitek0% (1)
- Science 4 1st Summative TestDocument2 paginiScience 4 1st Summative TestEmz FloresÎncă nu există evaluări
- NLR As Biomarker of DeleriumDocument9 paginiNLR As Biomarker of DeleriumbrendaÎncă nu există evaluări
- Anxiety Disorder: Student Name: Malinda SirueDocument9 paginiAnxiety Disorder: Student Name: Malinda SirueEsmareldah Henry SirueÎncă nu există evaluări
- Local Data: Roanoke City and Alleghany Health Districts / 12.28.21Document2 paginiLocal Data: Roanoke City and Alleghany Health Districts / 12.28.21Pat ThomasÎncă nu există evaluări
- Maritime Declaration of HealthDocument1 paginăMaritime Declaration of HealthKarym DangerousÎncă nu există evaluări
- Merged Document 14 PDFDocument9 paginiMerged Document 14 PDFMurali SmatÎncă nu există evaluări
- MODUL 1 FKG UnairDocument61 paginiMODUL 1 FKG UnairLaurensia NovenÎncă nu există evaluări
- Understanding BenzodiazepinesDocument7 paginiUnderstanding BenzodiazepinesChris Patrick Carias StasÎncă nu există evaluări
- Zinc Oxide-Eugenol and Calcium HydroxideDocument5 paginiZinc Oxide-Eugenol and Calcium HydroxideJulioÎncă nu există evaluări
- CHN 1 Week 13 Lecture MHGAPDocument71 paginiCHN 1 Week 13 Lecture MHGAPAech EuieÎncă nu există evaluări
- Androgenetic Alopecia and Current Methods of TreatmentDocument4 paginiAndrogenetic Alopecia and Current Methods of TreatmentPamela TrujilloÎncă nu există evaluări
- Kala-Azar (Leishmaniasis) Symptoms, Signs, DiagnosisDocument36 paginiKala-Azar (Leishmaniasis) Symptoms, Signs, Diagnosisatulbd2006Încă nu există evaluări
- Afterword by Ilyene BarskyDocument5 paginiAfterword by Ilyene Barskykkleiman_ppscÎncă nu există evaluări