Documente Academic
Documente Profesional
Documente Cultură
Otolaryngologists' Role in Improving Cognitive Decline.
Încărcat de
neculavTitlu original
Drepturi de autor
Formate disponibile
Partajați acest document
Partajați sau inserați document
Vi se pare util acest document?
Este necorespunzător acest conținut?
Raportați acest documentDrepturi de autor:
Formate disponibile
Otolaryngologists' Role in Improving Cognitive Decline.
Încărcat de
neculavDrepturi de autor:
Formate disponibile
otoneurology
Otolaryngologists’ role
in improving cognitive decline
Cristina Maria Abstract Rezumat
Blebea,
Laszlo Peter Longevity is expected to rise in the following years, therefore Longevitatea populației globale se așteaptă să crească în
neurological problems become a global health concern. următorii ani, prin urmare afecțiunile neurologice devin
Ujvary, Dementia and hearing loss are highly prevalent pathologies o problemă globală de sănătate. Demența și hipoacuzia
Maximilian in the older population, and a possible association between sunt patologii cu o prevalență înaltă la populația în vârstă,
George them was studied in recent years. Dementia is still considered în ultimii ani fiind studiată o posibilă asociere între ele.
Dindelegan, an incurable disease, but the evolution of the symptoms is Demența este considerată o boală incurabilă, dar evoluția
Violeta Necula, considered manageable by addressing the risk factors. In the simptomelor poate fi gestionată prin abordarea factorilor
latest studies, hearing loss has been considered a modifiable de risc. În ultimele studii, hipoacuzia este considerată factor
Alma Aurelia risk factor for cognitive decline, along with obesity, smoking, de risc modificabil pentru declinul cognitiv, împreună cu
Maniu hypertension, depression and physical inactivity. This paper obezitatea, fumatul, hipertensiunea, depresia și inactivitatea
ENT Departament, presents the potentially pivotal role hearing loss might fizică. Această lucrare prezintă rolul potențial pe care hipo
“Iuliu Hațieganu” University have in the evolution of cognitive decline and a summary acuzia îl poate avea în evoluția declinului cognitiv și un
of Medicine and Pharmacy,
Cluj-Napoca, Romania of studied theories regarding the relationship between rezumat al teoriilor studiate cu privire la relația dintre aceste
Corresponding author:
these pathologies. The recent guideline of the World Health două patologii. Ghidul publicat de Organizația Mondială
Ujvary Laszlo Peter Organization regarding cognitive decline management a Sănătății cu privire la gestionarea declinului congnitiv la
E-mail: ujvarypeter@outlook.com; involves otolaryngologists in the effort of improving populația în vârstă implică otorinolaringologii în efortul de a
ujvary.laszlo@umfcluj.ro
outcomes. îmbunătăți rezultatele.
Keywords: hearing loss, cognitive decline, dementia, risk Cuvinte-cheie: hipoacuzie, declin cognitiv, demență, factor
factor de risc
Submission date:
2.09.2021 Rolul medicului otorinolaringolog în îmbunătățirea declinului cognitiv
Acceptance date: Suggested citation for this article: Blebea CM, Ujvary LP, Dindelegan MG, Necula V, Maniu AA. Otolaryngologists’ role in improving cognitive decline.
15.09.2021 ORL.ro. 2021;52(3):18-20.
Introduction Dementia and hearing loss can present to the clini
Increased longevity worldwide, along with fertility cian with common symptoms, such as not following a
decline, give rise to the phenomenon known as popula line of conversation, difficulty concentrating, commu
tion aging. The global population will continue to grow, nication changes, fatigue, irritation and social isolation.
and by 2050 will reach approximately 10 billion. What Therefore, a high susceptibility must be taken, not to
is notable is that the population aged 60 years old or misdiagnose hearing loss as dementia or to consider
over will grow faster than all younger age groups(1). As symptoms of dementia worsening.
the world’s population increases in age, the neurological
problems are considered one of the significant causes of Where is hearing loss standing regarding
disability among older adults worldwide. dementia?
Dementia is a pathology that is considerably corre Age-related hearing loss is a multifactorial disease
lated with age, with around 50 million people suffering caused by genetic factors that can be affected by many
from it worldwide, of which almost two-thirds live in conditions, including diabetes mellitus, hypertension,
low- and middle-income countries. The number of people cardiovascular disease, and noise-induced inner ear
who will develop dementia is expected to increase, with damages.
nearly 10 million new cases every year(2). Dementia is also a heterogeneous disease, and its
Hearing loss is another highly prevalent neurologic evolution is also influenced by risk factors like cardio
condition in older adults which – like dementia – impacts vascular disease, cerebrovascular disease, metabolic and
the quality of life. Hearing loss is considered at this mo psychiatric factors, education, lifestyle and diet. The
ment to be the third most common health condition af Lancet Commission on Dementia Prevention, Interven
fecting older adults. Noteworthy is that more than 58% tion and Care results suggest that 65% of dementia risk
of moderate or higher grade hearing loss is experienced factors are potentially non-modifiable – age, genetics,
by the adult population above 60 years of age, affecting apolipoprotein E (ApoE 4). On the other hand, around
one-third of the people over 65 years old and two-thirds 35% of dementia is assignable to a combination of nine
of those aged over 70(3). risk factors(4).
18 ORL.ro No. 52 (3) 2021 • Year XIV • ISSN 2067-6530
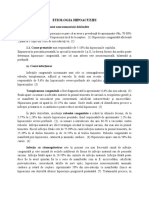
Model of contribution of risk factors to dementia Figure 1. Percentage
distribution of risk
factors for dementia
Poor e
7.5%
ducati
Obe
sity
on
Hy
pe
0.8
rte
%
n
sio
n2
Early li
%
Hea
ring
fe
loss
9.1
%
Mi
dli
fe
Diabetes
1.2%
Social isolation 2.3
%
Physical inactivity
2.6%
Late life Age and
Pote genetic
n s
n 4% mod tially n
De pressio ifiab o
le 65 n-
%
%
5.5
ng
oki
Sm
7%
4
oE
Ap
Potentially non-modifiable 65% Midlife Late life Early life
As prevention is preferable to cure, there is a grow reduction of cognitive decline and dementia, hearing
ing interest in controlling these modifiable risk fac loss is recognized as a risk factor for dementia. Also, the
tors present during a patients’ life span. The Lancet guideline grants priority to hearing loss interventions
Commission on Dementia Prevention, Intervention in the management of those at risk of cognitive impair
and Care published in 2017 a list of nine potential risk ment, as they can substantially improve the outcomes
factors related to early life, midlife, or later life peri for older people in multiple domains(13).
ods. Hearing loss has been distinguished as one of the
Commission’s main potentially modifiable risk factors What does research on dementia
for dementia. and hearing loss reveal?
Although the risk ratio (RR) of hearing loss is com Although epidemiological studies have demonstra
parable with other risk factors, it is a highly prevalent ted this association, the underlying mechanism of how
pathology, occurring in 32% of individuals older than hearing loss increases the risk of cognitive decline and
55 years of age; hence, it explains the high population dementia is not yet precise. Wayne et al.(14) reviewed the
attributable fraction (PAF) of 9%. literature and summarized four possible hypotheses.
As the number of studies that consider a possible The cognitive load hypothesis considers that cog
relationship between these two conditions is growing, nitive decline may reduce the cognitive resources avail
the results suggest that their interrelation may consist able for auditory perception, clinically manifested as
of that hearing loss may be a risk factor for the develop hearing loss. The evidence supporting this hypothesis
ment of dementia in older adults. is limited.
Several studies(5-8), reviews(9,10) and meta-analyses(11) The information degradation hypothesis advo
showed that hearing loss is an independent risk factor cates that sensory deficits may be compensated by older
for dementia in older adults. Lin et al.(12) also indicated adults via increased reliance on cognitive resources. Toil
that the risk of developing dementia increased linearly some listening, present when the accuracy of the audi
with baseline hearing loss severity (1.27 times increased tory input is poor, seems to place greater demands on the
risk per 10 dB of hearing loss). executive function and working-memory resources(15).
Therefore, in the latest guideline published in 2019 By activating this mechanism, the cognitive resources
by the World Health Organization (WHO) regarding risk available for other tasks are reduced, but this can be a
ORL.ro No. 52 (3) 2021 • Year XIV • ISSN 2067-6530
19
otoneurology
potentially reversible byproduct of devoting cognitive Do hearing aids improve cognitive decline?
resources to perception. While dementia is not curable, many manifestations
In order to assess hearing loss, pure-tone audiometry of it are now considered to be manageable, with an im
remains the gold standard, but audiometry cannot de provement of the course of the disease. Though hearing
tect age-related synaptopathies. Medium- and low- loss is considered a risk factor for cognitive decline, it is
spontaneous rate auditory nerve fibers are believed to not fully established whether correction – such as hear
be essential for temporal coding fidelity, and therefore a ing aids – can delay or prevent the outset of dementia.
precise representation of frequency information. As they Preliminary studies have shown some degree of stead
appear susceptible to noise damage, their degradation iness and, in some cases, the improvement of cognitive
may underlie the speech in noise difficulties experienced function six months after cochlear implantation(17,18).
by older listeners and can precede pure-tone audiometry In 2016, Taljaard and Olathe published a meta-anal
threshold elevations. ysis on the relationship between hearing impairment
The sensory deprivation hypothesis is considered and cognitive function. An association between hear
the irreversible variant of the information-degradation ing loss and dementia was confirmed in this study, but
mechanism, with more permanent cognitive declines as noteworthy was also the observation that treating hear
a result of chronic auditory deprivation. Atrophy and ing impairment significantly improved the cognitive
reorganization of cortical auditory areas are the implied function(19).
potential mechanisms of this hypothesis. Based on this early research, although not sufficient,
A common cause or shared neurobiological pa- the World Health Organization considers that hearing
thology hypothesis, in which both pathologies are screening of older adults and early intervention may
potentially a joint product of a generalized neurodegen become more relevant, and addressing hearing loss
erative process, is also considered. In this case, hearing through hearing devices may have a positive influence
loss can be considered simply an early manifestation of on the individual’s cognition(3).
dementia during its preclinical stage.
Genetic involvement in dementia is complex, and Conclusions
at the moment the ApoE4 allele is the only known ge By this time, hearing aids have been clearly demon
netic factor that significantly increases susceptibility to strated to be efficacious in patients with sensorineural
late-onset Alzheimer’s disease(4). Research conducted by hearing loss. However, there is still a great need for stud
Morita et al. and other prior studies investigating hear ies to determine the role of routine hearing screening in
ing loss and ApoE4 allele status found no association improving patient’s outcomes, given that the symptoms
between ApoE4 Allele and hearing loss(16). of hearing loss can be mistaken for dementia. n
Microvascular pathology and older age increase the
risk for hearing loss and dementia and might, therefore, Conflicts of interests: The authors declare no con
confound the association. flict of interests.
1. United Nations, Department of Economic and Social Affairs, Population Division. dementia: A systematic review. Laryngoscope Investig Otolaryngol. 2017;2(2):69.
References
World Population Prospects: The 2017 Revision, Key Findings and Advance 11. Liang Z, Li A, Xu Y, Qian X, Gao X. Hearing Loss and Dementia: A Meta-Analysis of
Tables. Working Paper No. ESA/P/WP/248. Prospective Cohort Studies. Front Aging Neurosci. 2021;8(13):695117.
2. World Health Organization. Global action plan on the public health response 12. Lin FR, Yaffe K, Xia J, Xue Q-L, Harris TB, Purchase-Helzner E, Satterfield S,
to dementia 2017-2025. Geneva World Health Organization;2017. Licence: CC Ayonayon HN, Ferrucci L, Simonsick EM. Hearing Loss and Cognitive Decline
BY-NC-SA 3.0 IGO. Among Older Adults. JAMA Intern Med. 2013;173(4):293–9.
3. World report on hearing. Geneva: World Health Organization; 2021. Licence: CC 13. Risk reduction of cognitive decline and dementia: WHO guidelines. Geneva:
BY-NC-SA 3.0 IGO . World Health Organization; 2019. Licence: CC BY-NC-SA 3.0 IGO.
4. Livingston G, Sommerlad A, Orgeta V, Costafreda SG, Huntley J, Ames D, Ballard 14. Wayne RV, Johnsrude IS. A review of causal mechanisms underlying the link
C, Banerjee S, Burns A, Cohen-Mansfield J, Cooper C, Fox N, Gitlin LN, Howard between age-related hearing loss and cognitive decline. Ageing Res Rev.
R, Kales HC, Larson EB, Ritchie K, Rockwood K, Sampson EL, et al. Dementia 2015;23:154–66.
prevention, intervention, and care. Lancet. 2017;390(10113):2673–734. 15. Amichetti NM, Stanley RS, White AG, Wingfield A. Monitoring the capacity of
5. Lin FR, Metter EJ, O’Brien RJ, Resnick SM, Zonderman AB, Ferrucci L. Hearing working memory: Executive control and effects of listening effort. Mem Cogn.
Loss and Incident Dementia. Arch Neurol. 2011;68(2):214-20. 2013;41(6):839–49.
6. Deal JA, Betz J, Yaffe K, Harris T, Purchase-Helzner E, Satterfield S, Pratt S, 16. Morita Y, Sasaki T, Takahashi K, Kitazawa M, Nonomura Y, Yagi C, Yamagishi
Govil N, Simonsick EM, Lin FR. Hearing impairment and incident dementia and T, Ohshima S, Izumi S, Wakasugi M, Yokoseki A, Narita I, Endo N, Horii A. Age-
cognitive decline in older adults: The health ABC study. Journals Gerontol - Ser A related Hearing Loss Is Strongly Associated with Cognitive Decline Regardless of
Biol Sci Med Sci. 2017;72(5):703–9. the APOE4 Polymorphism. Otol Neurotol. 2019;40(10):1263–7.
7. Gurgel RK, Ward PD, Schwartz S, Norton MC, Foster NL, Tschanz JT. Relationship 17. Issing C, Baumann U, Pantel J, Stöver T. Impact of Hearing Rehabilitation Using
of hearing loss and dementia: A prospective, population-based study. Otol Cochlear Implants on Cognitive Function in Older Patients. Otol Neurotol.
Neurotol. 2014;35(5):775–81. 2021;42(8):1136-1141.
8. Gallacher J, Ilubaera V, Ben-Shlomo Y, Bayer A, Fish M, Babisch W, Elwood P. 18. Mosnier I, Bebear JP, Marx M, Fraysse B, Truy E, Lina-Granade G, Mondain M,
Auditory threshold, phonologic demand, and incident dementia. Neurology. Sterkers-Artières F, Bordure P, Robier A, Godey B, Meyer B, Frachet B, Poncet-
2012;79(15):1583–90. Wallet C, Bouccara D, Sterkers O. Improvement of cognitive function after
9. Loughrey DG, Kelly ME, Kelley GA, Brennan S, Lawlor BA. Association of Age- cochlear implantation in elderly patients. JAMA Otolaryngol Head Neck Surg.
Related Hearing Loss With Cognitive Function, Cognitive Impairment, and 2015;141(5):442–50.
Dementia: A Systematic Review and Meta-analysis. JAMA Otolaryngol Neck Surg. 19. Taljaard DS, Olaithe M, Brennan-Jones CG, Eikelboom RH, Bucks RS. The
2018;144(2):115–26. relationship between hearing impairment and cognitive function: a meta-
10. Thomson RS, Auduong P, Miller AT, Gurgel RK. Hearing loss as a risk factor for analysis in adults. Clin Otolaryngol. 2016;41(6):718–29.
20 ORL.ro No. 52 (3) 2021 • Year XIV • ISSN 2067-6530
Copyright of ORL.ro is the property of MEDICHUB MEDIA, S.R.L. and its content may not
be copied or emailed to multiple sites or posted to a listserv without the copyright holder's
express written permission. However, users may print, download, or email articles for
individual use.
S-ar putea să vă placă și
- Urechea ppt1Document32 paginiUrechea ppt1neculavÎncă nu există evaluări
- DGN HADocument106 paginiDGN HAneculavÎncă nu există evaluări
- Programul de Screening AuditivDocument12 paginiProgramul de Screening AuditivneculavÎncă nu există evaluări
- Importanta Abordarii MultidisciplinareDocument18 paginiImportanta Abordarii MultidisciplinareneculavÎncă nu există evaluări
- FESS IngrijiriDocument28 paginiFESS IngrijirineculavÎncă nu există evaluări
- Genetica HA (Autosaved)Document24 paginiGenetica HA (Autosaved)neculavÎncă nu există evaluări
- IC de La ScreeningDocument28 paginiIC de La ScreeningneculavÎncă nu există evaluări
- Copilul HipoacuzicDocument79 paginiCopilul HipoacuzicneculavÎncă nu există evaluări
- Lumea Prin Culoare Si Sunet 37 - Hear-RingDocument1 paginăLumea Prin Culoare Si Sunet 37 - Hear-RingneculavÎncă nu există evaluări
- Factori de Prognostic În SBIDocument23 paginiFactori de Prognostic În SBIneculavÎncă nu există evaluări
- Hipoacuzia Genetica - Dismorfiile CFDocument26 paginiHipoacuzia Genetica - Dismorfiile CFneculavÎncă nu există evaluări
- 2-Etiologia HADocument11 pagini2-Etiologia HAneculavÎncă nu există evaluări
- (QHJJQTHQDM) : Buletin de RezultateDocument3 pagini(QHJJQTHQDM) : Buletin de RezultateneculavÎncă nu există evaluări
- Ionel TeodoreanuLa MedeleniVol.1 - Hotarul NestatornicDocument185 paginiIonel TeodoreanuLa MedeleniVol.1 - Hotarul NestatornicLaura Tulei100% (1)
- Sinuzitele FungiceDocument35 paginiSinuzitele FungiceneculavÎncă nu există evaluări
- Impedansmetria-Arad 2018Document45 paginiImpedansmetria-Arad 2018neculavÎncă nu există evaluări
- Algoritm DGN AudiologicDocument39 paginiAlgoritm DGN Audiologicneculav100% (1)
- Ghidurile de Practica Medicala PDFDocument366 paginiGhidurile de Practica Medicala PDFbrukner30Încă nu există evaluări
- Andrew Gross - Singurul Om PDFDocument307 paginiAndrew Gross - Singurul Om PDFAura Ciobotaru100% (1)
- Hipoacuzia Si Impactul Ei Asupra ComunicariiDocument23 paginiHipoacuzia Si Impactul Ei Asupra ComunicariineculavÎncă nu există evaluări
- Anatomie, FiziologieDocument36 paginiAnatomie, FiziologieneculavÎncă nu există evaluări
- DNG HAT Cu MT InchisaDocument23 paginiDNG HAT Cu MT InchisaneculavÎncă nu există evaluări
- HipoacuziaDocument18 paginiHipoacuzianeculavÎncă nu există evaluări
- DNG HAT Cu MT InchisaDocument23 paginiDNG HAT Cu MT InchisaneculavÎncă nu există evaluări
- Hipoacuzia CopiluluiDocument19 paginiHipoacuzia CopiluluineculavÎncă nu există evaluări
- Chestionar Glasgow CorectatDocument3 paginiChestionar Glasgow CorectatneculavÎncă nu există evaluări
- Boala MeniereDocument13 paginiBoala MeniereneculavÎncă nu există evaluări
- Istoria IncaltaminteiDocument6 paginiIstoria IncaltaminteineculavÎncă nu există evaluări
- Hipoacuzia La CopiiDocument6 paginiHipoacuzia La Copiineculav100% (1)