Documente Academic
Documente Profesional
Documente Cultură
Efectele Institutionalizarii Asupra Copiilor Din Romania
Efectele Institutionalizarii Asupra Copiilor Din Romania
Încărcat de
Ene CarmenTitlu original
Drepturi de autor
Formate disponibile
Partajați acest document
Partajați sau inserați document
Vi se pare util acest document?
Este necorespunzător acest conținut?
Raportați acest documentDrepturi de autor:
Formate disponibile
Efectele Institutionalizarii Asupra Copiilor Din Romania
Efectele Institutionalizarii Asupra Copiilor Din Romania
Încărcat de
Ene CarmenDrepturi de autor:
Formate disponibile
1
Efectele instituionalizrii asupra copiilor din Romnia
- Studiu concret n judeul Bihor -
Lavinia Onica-Chipea, Simona Stanciu i Floare Chipea, Universitatea din Oradea, Romnia
1. Scurt istoric privind instituionalizarea copilului n Romnia
2. Caracteristici ale vieii n instituiile de protecie a copilului din
Romnia reflectate n opinia persoanelor instituionalizate
1. Scurt istoric privind instituionalizarea copilului n Romnia
n Romnia, politica pronatalist practicat de regimul comunist care ncuraja natalitatea
fr un suport adecvat economic sau a politicilor sociale, alturi de absenta mijloacelor
contraceptive a dus la cresterea numrului de copii ntr-un timp scurt. Interventia statului a constat
n promisiunea de suport a familiilor cu multi copii care nu puteau s-si asume descendentii,
plasnd copiii n institutii numite generic orfelinate. Astfel s-a creat un sistem de institutii cu un
personal angajat care era deficitar att din punct de vedere numeric, ct si ca pregtire de
specialitate. Cile traditionale de protectie a copilului, ca de exemplu plasarea n familia extins au
fost de regul omise, ca si mentinerea fratilor n aceeasi institutie. n leagnele de copii erau
plasati copii de pn mplineau 3 ani, iar dup aceast vrsta ajungeau n alte institutii doar pe
criteriul vrstei, fr a tine cont de individualitatea lor, pn mplineau 18 ani.
Plasarea dintr-o institutie n alta, pierderea identittii si a sentimentului de apartenent la o
familie, alturi de abuzurile frecvente care aveau loc frecvent n aceste institutii au dus la
traumatizarea pe viat a multor copii.
Legea nr.3/1970 introducea cel mai aberant sistem de protectie a copilului aproape
exclusiv institutionalizat care avea s lase urme asupra dezvoltrii copilului, dimensionrii
sistemului, efortului financiar, care nici dup aproape 20 ani de la schimbarea regimului care l-a
introdus nu s-au sters. n urma acestui sistem au rmas: copii care la mplinirea vrstei de 18 ani
erau lsati n strad fr a avea o pregtire suficient pentru viata independent si nici resursele
materiale sau financiare pentru a se descurca reflect de fapt o socializare deficitar a acestora prin
lipsa unei perspective asupra vietii adulte (Zamfir, C., 1997, pp.96-97), persoane care datorit
institutionalizrii prelungite nu au mai prsit niciodat sistemul, devenind asistati pe viat ai
institutiilor pentru persoane cu handicap; ntrzieri mentale, fizice si emotionale, traumatisme
psiho-emotionale grave, distorsiuni n personalitatea copiilor. Sistemul supradimensionat de
institutii, cu sute de locuri, prost ntretinute si dotate, cu conditii de viat precare, de multe ori
construite n zone greu accesibile, departe de ochii populatiei, a fost deservit de un personal
2
neinteresat n cea mai mare parte de situatia copiilor pe care trebuiau s-i protejeze si care a
ntretinut sistemul si o dat cu el privilegiile lui mai mult de 30 de ani.
Casele de copii nu se strduiau s pstreze contactul cu printii copiilor internati, care
veneau foarte rar s-i viziteze. Atmosfera interioar era adesea caracterizat prin primitivism, lips
de participare a copiilor, disciplin bazat pe subordonare si pedepse fizice, program strict, abuzuri
fizice asupra copiilor, tratamente degradante, situatii umilitoare, mergndu-se pn la abuz sexual
din partea copiilor mai mari, dar uneori si a adultilor, a personalului. Toate acestea n situatia n
care institutiile pentru copii trebuie s reprezinte, mai nainte de toate, un substitut al familiei, un
mediu socio-emotional vital pentru dezvoltarea copiilor.
Declinul economic din Romnia, alturi de deficitul de personal specializat n ngrijirea
copiilor institutionalizati, a dus la deteriorarea dramatic a conditiilor n institutii. Nu exist
statistici exacte, ns se estimeaz c la nceputul anului 1990 existau circa 100.000 copii n
institutii (dup Autoritatea National pentru Protectia Drepturilor Copilului, www.copii.ro).
Dup 1989 au avut loc o serie de schimbri n sensul mbunttirii situatiei sociale n
Romnia. Politicile reparatorii din primii ani dup 1990 au vizat protectia copilului
institutionalizat. La descresterea numrului copiilor institutionalizati contribuie si programele de
prevenire a abandonului prin planificare familial si de educatie sexual, (descreste ns si
natalitatea). Urmarea acestor msuri a fost reducerea numrului de copii din institutii, paralel cu un
mare val de adoptii internationale legale si mai ales ilegale, de interes pentru copii prsiti si
orfani, victime ale legii de interzicere a avorturilor din perioada comunist.
n timp are loc modificarea cadrului legislativ si administrativ. Abordarea descentralizat
are ca obiectiv prevenirea institutionalizrii prin sprijinirea familiilor, nchiderea institutiilor de tip
vechi, alturi de gsirea de solutii alternative pentru protectia copilului care s rspund nevoilor
lor individuale, ca reintegrarea n familia de origine, alternative de tip familial (asistentul maternal
profesionist, rude, alte familii/persoane), protectia copilului n csute de tip familial sau
apartamente, servicii de suport (consiliere, ngrijire de zi, servicii de recuperare pentru copilul cu
handicap etc.). Alte msuri vizeaz organizarea asistentei profesionale de protectie a copilului si
din 1990, renfiintare nvtmntului de asistent social (Zamfir, C., 1997, p.244). ncepnd din
1995 Romnia adopt un sistem care vizeaz promovarea si respectarea drepturilor tuturor
copiilor. n vederea pregtirii pentru viat a tinerilor care prsesc sistemul de protectie a copilului
s-a urmrit integrarea lor socio-profesional prin crearea unui cadru legislativ si institutional care
s asigure suportul necesar pentru gsirea unui loc de munc si a unei locuinte, cu instituirea unor
servicii specifice din cadrul Directiilor pentru Protectia Copilului (Directia General de Asistent
Social si Protectia Copilului, http://sas. mmssf.ro/).
3
2. Caracteristici ale vieii n instituiile de protecie a copilului din Romnia reflectate n
opinia persoanelor instituionalizate
Metodologia cercetrii
Cercetarea proiectat si realizat n perioada ianuarie-iulie 2006 n judetul Bihor si-a propune
s identifice gradul de integrare social a persoanelor care au mplinit 18 ani si provin din
institutiile de stat pentru protectia copilului. Am vizat integrarea acestei categorii de persoane
printr-o tripl perspectiv: integrarea persoanelor n munc, n familie si n comunitatea din care
fac parte.
Pe de alt parte, studiul a urmrit identificarea caracteristicilor personale si de grup si a
factorilor care au influentat integrarea social a tinerilor din aceast categorie.
Pentru realizarea scopului mentionat ne-am stabilit urmtoarele obiective:
Reconstructia analitic a caracteristicilor vietii din institutiile pentru protectia copilului;
Investigarea atitudinilor si comportamentelor cu privire la munc, educatie, familie;
Determinarea factorilor care au influentat integrarea social a persoanelor provenite din
institutii;
Determinarea expectantelor si perspectivelor de viitor ;
Realizarea unei tipologii a modului de integrare socio-profesional a tinerilor
postinstitutionalizati din judetul Bihor.
In demersul nostru am folosit urmtoarele metode de cercetare:
ancheta sociologic pe baza chestionarului;
ancheta pe baza interviului;
metoda observatiei;
metoda studiului de caz;
analiza documentelor sociale.
Instrumentele de investigatie utilizate au cuprins dimensiuni si indicatori referitori la
specificul vietii n institutii pentru protectia copilului, la modalitatea concret de integrare n
munc, n familie, n grupurile sociale, n general, la tipurile de comportamente manifestate de
subiectii investigati, la atitudinile fat de familie, scoal, semeni, la expectantele lor.
n cazul anchetei pe baza chestionarului am selectat subiectii pe baza principiului bulgrelui
de zpad, pornind de la faptul c, n judetul Bihor nu a existat o preocupare pentru inventarierea
persoanelor care provin din institutii pe localitti, locuri de munc sau oricare alte criterii. Pe de
alt parte este dificil s stabilesti exact cti tineri dezinstitutionalizati triesc n Oradea sau n judet
avnd n vedere tendinta acestora de a se deplasa dintr-o localitate n alta, fr a avea un domiciliu
stabil, identificabil. De aici si unele dificultti si controverse privind stabilirea responsabilittilor n
acordarea drepturilor de asistent social.
4
Lund n considerare aspectele mentionate am pornit, n procesul de identificare a
persoanelor care provin din institutiile pentru protectia copilului de la consultarea unui lider
informal al acestora, care n prezent are 34 de ani. Persoana identificat se erijeaz n liderul
acestor categorii, cunoscnd sau cel putin pretinznd c cunoaste, situatia fiecrui individ care face
parte din grupul persoanelor dezinstitutionalizate. Aceast oportunitate a facilitat acceptarea
colaborrii n cadrul cercetrii din partea subiectilor si ne-a oferit posibilitatea s completm
informatiile eliptice n cazul unor interviuri.
Tot prin intermediul subiectului mentionat, am reusit s ptrundem dincolo de aparente si s
ne formm o imagine mai realist despre viata, activitatea, asteptrile, valorile, subiectilor cuprinsi
n studiu.
Am cuprins n ancheta sociologic pe baz de chestionar un numr de 90 de subiecti de
vrste, situatii si cu caracteristici diferite, dup cum vom prezenta pe parcursul lucrrii.
Un ghid de interviu care vizeaz relativ aceleasi dimensiuni si indicatori a fost administrat
unui numr de 30 de specialisti care lucreaz cu copiii postinstitutionalizati si cu cei din institutii,
cunoscndu-le specificitatea.
Pentru a sesiza si aspectele cantitative ale fenomenului, att la nivel national ct si la nivelul
judetelor Bihor, am folosit si metoda analizei documentelor sociale, respectiv anuarele statistice,
documentele oferite de Directia General de Asistent Social si Protectie a Copilului si
Autoritatea National pentru Protectia Copilului.
Datele culese prin intermediul acestor metode le-am structurat n dou teme mari:
O tem care va urmri dezbaterea problemei privind identificarea
caracteristicilor socializrii n institutiile pentru protectia copilului, din perspectiva subiectilor,
aspecte care, de altfel vor fi prezentate n materialul de fat.
A doua tem si-a propus cunoasterea modului de integrare socioprofesional,
inclusiv construirea unor tipologii, patternuri de integrare social a tinerilor care au mplinit vrsta
de 18 ani si au prsit institutiile pentru protectia copilului.
Prin intermediul unui set de ntrebri incluse n ancheta pe baza chestionarului ne-am propus
s surprindem caracteristicile vietii din institutiile de protectie a copilului din judetul Bihor, prin
prisma perspectivelor persoanelor care au fost socializate n institutiile respective. Am chestionat
astfel opinia privind viata n institutii, tipurile de activitti desfsurate n perioada socializrii n
institutii, relatiile interpersonale dintre copiii institutionalizati, pregtirea scolar, viata intim,
consumul de alcool si droguri, starea de infractionalitate, implicarea n acte violente si abuz, etc.
Pentru a crea o imagine ct mai adecvat despre specificul vietii din institutii am confruntat,
ori de cte ori a fost posibil, perspectivele persoanelor institutionalizate cu cele ale specialistilor si
chiar cu observatiile personale sau ale operatorilor de chestionar si de interviu.
5
n continuare vom prezenta cteva caracteristici ale vietii din institutii prin prisma tinerilor
postinstitutionalizati.
A. Viaa n instituii
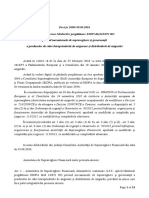
Grafic nr.1. Opinia privind viaa n instituii
17,86
41.65
13,10
13,10
14,29
foarte buna
buna
nici buna nici
rea
rea
foarte rea
Ce prere avei despre viaa n instituii?
n acest context, surprinztor este faptul c o pondere de 59,51% dintre cei intervievati au o
prere bun si foarte bun privind institutiile pentru protectia copilului si numai circa 27 % au
prere rea si foarte rea. Faptul poate fi explicat prin aceea c bun sau rea, institutia pentru
protectia copilului este singura realitate la care aceast categorie de populatie se poate raporta.
Majoritatea copiilor nu au cunoscut alte experiente de viat, nici mcar pentru perioade scurte de
timp. Cea mai mare parte din cei care si-au cunoscut familiile naturale au fost dezamgiti,
considernd c au fost avantajati de faptul c au fost abandonati. Astfel este explicabil c, mai ales
dup trecerea timpului, cnd de regul dispar amintirile neplcute, rmn cu o impresie favorabil
despre copilrie.
Grafic nr. 2. Tipurile de activiti desfurate n instituii
Ce activiti ai desfurat n intituii?
1
4
%
3
%
7
%
4
9
%
2
%
1
4
%
1
1
%
curatenie
spectacole
concursuri
sporturi, comcursuri sportive
cules de borcane pentru a
face bani
meditatii
munca
Este semnificativ faptul c doar 11% dintre subiecti si amintesc c au muncit n institutiile
n care au copilrit, mai ales dac corelm datele cu rspunsurile la ntrebarea privind atitudinea
fat de munc, iar 14% declar c fceau meditatii. Pentru restul de 75%, activitile de care i
amintesc sunt concursurile, spectacolele, i activitile de divertisment. Datele oferite de subiecti si
cu aceast ocazie atest slaba pregtire pentru viat, oferit n institutii. n acest sens, n structura
activittilor desfsurate n institutii predomin divertismentul, munca si nvttura, care n mod
normal, ntr-un climat familial optim ocup cea mai mare pondere, sunt practic neglijate.
6
B. Viaa afectiv
Grafic nr.3. Relaiile de prietenie
Ai legat relaii de prietenie n instituii?
2
3
%
4
0
%
2
1
%
1
2
%
4
%
foarte multe multe putine foarte putine niciuna
Cea mai mare pondere, 63% au declarat c au avut multe si foarte multe astfel de relatii si
doar 37% au avut relatii putine, foarte putine sau nici una. Este interesant faptul c n institutii,
tinerii leag relatii foarte puternice ntre ei, considerndu-se o familie. Relatiile strnse de prietenie
si ntr-ajutorare continu si dup dezinstitutionalizare. Studiul i-a identificat mpreun n parcuri,
pe strzi, grupati n aceeasi locuint, pe aceeasi strad. Am ntlnit situatii n care grupul (constituit
din fete si bieti) a ngrijit copiii prietenilor lor, aflati n detentie pentru o anumit perioad de
timp. De altfel am sesizat aceste tendinte de ntr-ajutorare si chiar de renuntare la unele bunuri n
favoarea prietenilor aflati n dificultate, n toate mprejurrile pe care le-am analizat.
Grafic nr. 4. Relaiile de ataament
V-ai ataat de cineva anume ct timp ai fost n instituii?
8.88
68.9
12.22
10
nu da, de o educatoare da, de un iubit /
iubit
da, de un amic /
amic
%
Cei mai multi subiecti declar c nu s-au atasat de nimeni n institutie (68,9%). De altfel
lipsa de atasament este o trstur specific a persoanelor socializate n institutii, dup cum au
demonstrat numeroase studii redate n literatura de specialitate. Bender, de exemplu (1947),
mentioneaz incapacitatea de a iubi, de a intra ntr-o relatie si a o mentine, ca fiind principalul
defect al persoanelor care triesc n institutii, iar Godlfarb (1955) consider incapacitatea de a avea
relatii interpersonale apropiate si capacitatea de a adera la anumite reguli, ca fiind cea mai
semnificativ deviant. Lewis (1954) a aflat c 22% dintre copiii institutionalizati au dificultti de
relationare, iar Becker (1941) c nu au o ntelegere adecvat privind relatiile umane. Multi copii
7
crescuti n orfelinate prezint semne de dezvoltare anormal a personalittii, retard si dereglri
severe ale personalittii. (Godlfarb W, 1955).
Bowlby (1944) a observat c aceast lips de afectivitate apare cel mai adesea n adolescent
si maturitate acolo unde a existat lips de atasament la vrsta de 2-3 ani. Persoana lipsit de
afectivitate este caracterizat prin incapacitatea de a mentine relatii pe termen lung si de lipsa
sentimentului de vinovtie. Incapacitatea de a respecta anumite reguli nu se poate corecta la vrsta
maturittii, tot asa dup cum nu se poate compensa nevoia de afectiune (Bowlby J., 1944).
Subiectii care au declarat c s-au atasat de o anumit persoan din institutie au avut evolutii
diferite, n functie de modelul de viat oferit de persoana respectiv. Din interviurile prezentate
mai trziu a reiesit c cei care au urmat studii universitare, care s-au integrat pozitiv n structura de
roluri sociale au avut ca model, de regul, o educatoare sau o persoan, iubit sau iubit, provenit
dintr-o familie normal. n aceste cazuri a fost confirmat ntr-un mod excelent teoria asociatiilor
diferentiale, formulat de sociologul american Sutherland, conform creia comportamentul
criminal sau noncriminal nu se transmite pe cale ereditar, ci se nvat n cadrul proceselor de
comunicare si de relationare social dintre individul n cauz si diverse grupuri sociale cu care
acesta intr n contact. Aceast comunicare dintre individ si grupurile cu care intr n contact
poate fi verbal sau transmis prin mijloacele mass-media, ct si comportamental, modelele de
comportament fiind transmise prin exemplul altor persoane cu care vine n contact (Sutherland,
E., Cressey, D. R., 1966).
Relativ putini subiecti declar c au avut o relatie de iubire, n general de atasament cu o
persoan de sex opus.
Grafic nr. 5. Viaa intim
n timp ce ai fost instituionalizat ai avut
un/o prieten/ intim/?
5
3
%
4
7
%
da
nu
Viata sexual, desi un subiect sensibil, este relevant n identificarea gradului de
promiscuitate, dar si al unei dezvoltri fizice si psihice normale pentru o anumit vrst.
La ntrebarea dac au avut un prieten intim n timp ce erau institutionalizati, 53% au rspuns
pozitiv iar 47% negativ. Multi din cei care nu au avut un prieten intim n institutii au declarat c nu
au nceput nc viata sexual, iar altii consider acest subiect tabu, refuznd s rspund. Am
constatat c n marea majoritate, fetele sunt cele care declar c nu au nceput viata sexual si tot
ele sunt cele care consider subiectul tabu.
8
Corelnd rspunsurile nregistrate n cadrul anchetei pe baz de chestionar cu datele obtinute
prin intermediul studiilor calitative deducem c fetele au astfel de rezerve si pentru faptul c fiind
integrate n fundatii religioase, acceptarea lor n fundatii este conditionat de virginitate, dup
declaratia lor. Introducnd aceast variabil n explicatie, putem suspecta rspunsurile de
nesinceritate. De altfel interviurile specialistilor au sugerat c fundatiile adopt anumite politici
pentru descurajarea prostitutiei, a maternittii precoce, a vietii trite n promiscuitate, ceea ce ar
putea explica si constrngerea perceput de fetele din fundatii n privinta practicrii relatiilor
sexuale.
Grafic nr.6. Orientarea sexual
S-a ntmplat s cunoatei n intituii persoane cu
o alt orientare sexual?
4
6
%
5
4
%
da
nu
Dup cum se observ, aproape jumtate din subiecti declar c n institutiile pentru protectia
copilului se practic homosexualitatea. Specialistii cuprinsi n studiu au confirmat aceast
constatare, estimnd chiar o pondere mult mai mare dect cea redat de subiecti. Ei explic si
declaratia fetelor cu privire la virginitate prin practicarea lesbianismului. Mai mult, opinia
specialistilor este c homosexualitatea este un comportament care se nvat, institutiile pentru
protectia copilului constituind un exemplu elocvent n acest sens. Se relateaz faptul c abuzurile
sexuale, de tip hetero sau homosexual sunt practicate de multe ori n public, victimele predilecte
fiind bietii sau fetele cele mai retrase si neinitiate. Probabil satisfactia abuzatorului este cu att
mai mare cu ct victima este mai reticent la astfel de comportamente si mai naiv. Din datele
studiilor calitative am retinut c si n prezent tinerii din centrele de plasament sunt tint a
proxenetilor din afara institutiei, iar tinerii accept aceste situatii pentru cstigul obtinut.
C. Devian n instituii
Grafic nr.7. Implicarea n acte de violen i abuz
Ai fost implicat n acte de violen/abuz ct timp
ai fost instituionalizat?
7
2
%
2
8
%
da
nu
9
Rspunsurile subiectilor la ntrebarea privind practicarea btilor si a abuzului n institutiile
de protectia copilului sunt sugestive. O majoritate de 72 % au rspuns c au fost btuti sau abuzati
ct timp au locuit n centrele de plasament si doar 28 % au rspuns c nu au fost victime si nici nu
cunosc astfel de situatii. Datele sugereaz c n institutiile pentru protectia copilului din judetul
Bihor s-a practicat si s-a tolerat abuzul fizic si psihic asupra copiilor, ceea ce a marcat profund
structura personalittii si comportamentul acestora.
Grafic nr. 8. Tipul de abuz
Ce tip de abuz ai suferit?
3
2
%
5
1
%
1
7
%
am fost batut de colegii mai mari
am fost batut(a) de educatori
am fost batut(a) de colegii mai mari si educatori
Dintre cei care au fost abuzati ct timp au fost n institutii, 51 % declar c au fost btuti de
colegii mai mari, dar si de educatori, 32% au btuti de colegii mai mari, iar 17 % au fost btuti de
educatori.
Datele relev clar faptul c n institutiile de protectia copilului, tinerii erau abuzati,
maltratati, mai ales de copiii mai mari, dar si de persoanele care aveau menirea s se ocupe de
educatia lor. n toate cazurile faptele de acest gen sunt prezentate ca amintiri neplcute, cu o
atitudine de revolt, de dezaprobare, subiectii considerndu-se discriminati, prsiti ntr-o lume a
nimnui, n care nu au avut cui s cear compasiune si sprijin, determinati fiind s gseasc
singuri mijloacele de supravietuire n aceast jungl anacronic, departe de modelele de
civilizatie ale lumii moderne.
Grafic nr. 9. Alte tipuri de abuzuri
Ce alte incidente ai mai avut n instituie?
94.8%
5.1%
mi s-au furat haine i alte bunuri
abuz sexual
Din rspunsurile la ntrebarea deschis privind alte tipuri de abuzuri crora copiii din
institutii au fost expusi n perioada institutionalizrii reiese c era o practic generalizat de a se
10
fura haine si alte bunuri n institutiile de protectie, de vreme ce 95% din subiecti se declar victima
unor astfel de abuzuri. Faptul c fenomenul este att de general poate sugera c toti erau victime,
dar n acelasi timp si autori ai unor comportamente de acest tip. Este de nteles n aceast situatie
c furtul n institutii nu se sanctiona, c nu existau preocupri pentru descoperirea autorilor, pentru
descurajarea unor astfel de comportamente deviante. Repetndu-se, fr a fi sanctionate, furturile
au devenit obiceiuri acceptate de membrii grupului. n acest caz este explicabil de ce, dup
dezinstitutionalizare, furtul devine o ocupatie si un mod de trai predilect al unei prti nsemnate
dintre subiectii investigati. Dac mai adugm faptul c nu toti subiectii mrturisesc c au furat,
desi au astfel de obiceiuri, avem temeiuri s sustinem c n realitate infractiunile de furt sunt mult
mai multe dect cele descoperite de organele de politie si dect cele declarate de subiecti, fiind o
caracteristic a comportamentului tinerilor postinstitutionalizati.
Grafic nr. 10. Fumatul n instituii
Aveai prieteni/colegi n intituiicare fumau?
3
0
%
1
2
%
8
%
1
6
%
3
4
%
foarte multi multi putini foarte putini nici unul
La ntrebarea indirect cuprins n chestionar privind fumatul n institutii, cei mai multi
subiecti, 64% au declarat c au avut multi si foarte multi prieteni care fumau, ceea ce nseamn c
fumatul era o practic cvasigeneral printre copiii din institutii, fiind probabil o practic prin care
si revendicau apartenenta la grupul celor maturi, pe care de fapt i imitau prin acest tip de
comportament si care nu difer cu mult de comportamentul adolescentilor proveniti din familii
normale.
Grafic nr. 11. Consumul de alcool
Aveai prieteni/colegi n instituii care consumau alcool
8
%
6
%
1
2
%
1
2
%
5
8
%
4
%
f oarte multi multi putini f oarte putini niciunul ns
Dup cum se poate observa si din diagrama de mai sus, majoritatea, de 58% declar c nu au
avut nici un prieten sau coleg care s fii consumat alcool, putini si foarte putini, 24% si o pondere
11
de 18%, au recunoscut c aveau foarte multi si multi astfel de prieteni. Rspunsurile ntemeiaz
concluzia conform creia consumul de alcool nu reprezenta o practic generalizat n institutii,
chiar dac nu se poate afirma c era necunoscut.
Grafic nr. 12. Consumul de droguri
Aveai prieteni/colegi n instituii care consumau
droguri?
3
%
4
%
2
%
9
1
%
putini foarte putini niciunul NS NR
Dup cum se poate observa si din graficul de mai sus, o pondere redus (3%) declar c au
avut putini prieteni care consumau droguri, iar 4% aveau foarte putini prieteni consumatori de
droguri, n timp ce o majoritate de 92% declar c nu au avut nici mcar un coleg sau prieten n
instituia n care a locuit care s fi consumat astfel de substane.
Pornind de la ipoteza c la vicierea mediului de viat din institutii poate contribui si fumatul,
consumul de alcool si de droguri, am introdus n chestionar si ntrebri care au vizat
comportamente de acest gen. Am optat pentru ntrebri indirecte, pentru cresterea gradului de
sinceritate a rspunsurilor. Rspunsurile subiectilor sugereaz c n institutii fumatul este o
practic acceptat de multi tineri. n schimb consumul de alcool si de droguri nu a avut o
rspndire prea mare printre membrii grupului.
D. Educaia
Grafic nr. 13. Nivelul de instrucie al subiecilor
5.56
22.22
45.56
23.33
1.11
1.11
1.11
0.00 5.00 10.00 15.00 20.00 25.00 30.00 35.00 40.00 45.00 50.00
fara studii
7-10 clase
scoala profesionala
liceu
scoala postliceala
colegiu
studii universitare
Pregtire colar
.
Cercetrile privind mobilitatea social au relevat faptul c statusul social ocupat de individ n
societate este puternic influentat de nivelul de instructie al individului (Boudon R., L.,
12
1973). Graficul prezentat sugereaz clar c cei mai multi subiecti (46%) sunt absolventi de scoal
profesional, numai 23 % au absolvit liceul, doar 3% au absolvit studii postliceale si 6% sunt fr
studii. Dac tinem cont de corelatia pozitiv dintre nivelul de instructie si ocuparea statusurilor
sociale, simpla vizualizare a gradului lor de pregtire scolar ne permite s anticipm concluzia
conform creia statusurile sociale pe care le vor ocupa acesti tineri vor fi de un nivel inferior. Pe de
alt parte, chiar structura esantionului confirm ipoteza formulat privind nivelul sczut de
instructie al tinerilor care provin din institutiile pentru protectia copilului.
Copiii institutionalizati au n general rezultate scolare slabe si nu sunt capabili s se
adapteze colectivului (Godfarb W., 1955). Conform studiilor efectuate de Goldfarb, copiii din
institutii sunt cei mai dificili copii la scoal, au o slab motivatie pentru teme si au probleme
severe de nmagazinare a cunostintelor. Aceleasi cercetri au demonstrat c deficitul de atentie,
hiperactivitatea, labilitatea emotional si impulsivitatea sunt alte simptome ale copiilor crescuti n
institutie.
Grafic nr. 14. Atitudinea privind educaia
Considerai c este important educaia?
34%
45%
19%
2%
foarte importnanta
importanta
putin importanta
deloc importanta
Desi nivelul de instructie este sczut dup cum am mentionat deja, subiectii evalueaz n
procent de 89% c educatia este un factor important, respectiv foarte important. Discrepanta dintre
opinia privind rolul educatiei si nivelul de instructie atins poate fi interpretat si ca o reactie de
frustrare generat de constientizarea lipsei lor de oportunitti sociale.
Cercetrile din domeniul sociologiei educatiei au evidentiat faptul c familia are un rol
esential n stimularea interesului copilului pentru studii (Boudon R., L., 1973).
Aceste concluzii sunt reconfirmate si de datele cercetrii prezente. Majoritatea subiectilor,
dup cum rezult din graficul nr. 20, recunosc faptul c rezultatele obtinute la nvttur au fost
mediocre sau slabe. Fiind privati de suportul familiei n perioada socializrii primare si n primii
ani de scoal, cnd se pun bazele acumulrilor urmtoare, subiectii au preferat angajarea ntr-o
viat fr mari responsabilitti, care de regul reclam eforturi intense. Angajarea n activitatea de
nvtare se bazeaz pe constituirea unor motivatii puternice, care la vrste fragede sunt induse doar
de grupul familial.
13
Grafic nr. 15. Autoaprecierea rezultatelor colare
Cum apreciai rezultatele Dvs. scolare?
3
6
%
9
%
5
5
%
foarte bune nici foarte bune nici foarte slabe foarte slabe
Dac am ncerca s corelm nivelul de instructie al subiectilor cu autoaprecierea rezultatelor
scolare am putea constata c nu exist o concordant ntre cele dou caracteristici, majoritatea
subiectilor apreciind c la scoal au nregistrat rezultate medii, 55%, desi, dup cum declar
specialistii care cunosc acesti tineri, majoritate au ntmpinat mari dificultti n nvtare. Procentul
celor care declar c au avut rezultate foarte bune la nvttur este, de asemenea,
supradimensionat, iar cei care declar c au nregistrat rezultate slabe sunt probabil doar cei care se
declar fr scoal. Explicatia poate fi gsit doar n faptul c nu au capacitatea s se autoevalueze,
tocmai pentru c nici nu sunt constienti de ceea ce ar trebui s stie.
n continuare, vom reda punctul de vedere al unui specialist, care a fost intervievat n
legtur cu situatia tinerilor, postinstitutionalizati:
SM-coordonator n cadrul unei fundatii din Oradea:
Din experienta acumulat n activitatea n domeniu as putea s descriu acesti copii ca pe un
grup social distinct (indiferent de etnia lor); experienta institutional a nivelat si uniformizat
personalittile lor, determinnd un model comportamental caracteristic si deviant n acelasi timp.
Dup cum se stie, la vrsta de 3 ani acesti copii au fost supusi evalurii unei comisii care a stabilit
dac sunt integrabili, semi-integrabili sau neintegrabili n societate. n foarte multe cazuri, decizia
s-a dovedit arbitrar si cu rezultate dramatice pentru copii. Ei au fost repartizati n centre diferite n
functie de aceast apreciere si prea putini au reusit s depseasc predestinarea stiintific, fcut
n vremea vechiului regim.
In realitate numai cei mai buni (probabil sub 10%) au prsit institutia, ceilalti sunt n
continuare ntr-o atmosfer psihologic instituional asemenea unui rezervist din armat sau ca
un puscrias care nu mai sesizeaz libertatea, dup repetate ncarcerri. As vrea s mentionez
cteva practici si tratamente traumatizante, n special n ultimii ani ai comunismului, cnd
recesiunea economic a impus conditii de mizerie si iresponsabilitate n aceste institutii.
Lipsa hranei suficiente i-a transformat pe multi n obsedai ai foamei. Lic, un tnr de 25 de
ani, a fost invitat de niste strini la restaurant. Vroiau doar s ia masa mpreun cu el si s-i ofere
acest privilegiu. Lic a mncat rapid tot. Strinii au bnuit c omul este mai mult dect flmnd si
l-au ntrebat ce mai vrea s mnnce. Ca s scurtm relatarea, biatul nu s-a putut abtine usor si a
14
doua zi a avut nevoie de operatie pentru c stomacul a cedat... Biatul locuieste aproape de
fundatia noastr si vi-l pot prezenta. Este simptomatic att pentru fete, ct si pentru bieti,
insaietatea.
Btaia i frigul sunt alte dou terori cu care au fost obisnuiti. Cu stiinta pedagogilor si a
conducerii orfelinatelor, copiii mai mari au avut acces s abuzeze de cei mai mici sau mai slabi.
Era si un mijloc de a-i controla si a-i disciplina pe cei care erau "de ncredere" si aveau grij de cei
mici, n conditiile n care personalul era insuficient si prost pltit. ncepnd cu confiscarea
desertului sau a micului dejun, pn la abuzurile sexuale, btile pentru spectacol, comandate de
cei mari ntre copii mai mici, ceritul sau furtul la comand, erau administrate de legea junglei,
care actiona n institutii
Unele dintre cele mai grave fapte comise n institutii au fost abuzurile sexuale. Cei mari
aveau preferatii lor, relatiile homosexuale erau o practic obisnuit, att la fete ct si la bieti.
Orfelinatul nu permitea nici supraveghere real, nici intimitate. Abuzurile erau cunoscute si de
durat. Fr s am pregtire de psiholog, iat cteva din consecintele acestor abuzuri asupra
comportamentului acestor copii, asa cum le-am observat eu:
- Promiscuitatea. Majoritatea tinerilor postinstitutionalizati sunt bisexuali si au valori
morale extrem de laxe n acest domeniu. H B, de exemplu, este cununat legitim, are 4 copii, sper
c unul este al lui, ceilalti sunt ai altor prieteni, fosti colegi, din perioada n care a fost la
nchisoare. A trit foarte bine pentru c are un corp musculos... De la cumnata lui a luat sifilis. Nu
se stie dac n curte aceast boal s-a rspndit de la el sau de la ea sau de la amndoi.
- Homosexualitatea este, pentru majoritatea celor pe care i cunosc, o alternativ deschis.
Cstoria, de obicei nelegalizat, poate fi o form de proxenetism. Este foarte greu de probat
relatia de lesbianism dintre dou fete care triesc mpreun, mai ales dac lucreaz, sunt cuminti si
disciplinate. Este evident ns lipsa de interes pentru brbati si incapacitatea de se raporta corect
la acestia. Pe de alt parte, exist fete din acelasi mediu, mai putin retinute, care povestesc ct de
comune erau aceste practici (lesbiene).
- Lipsa de discernmnt este de asemenea o circumstant agravant pentru absenta valorilor
morale (care nu aveau de la cine s fie nvtate sau motivate n orfelinat). De exemplu, Irina spune
c ea nu se prostitueaz dect vara pentru c i place nghetata si nu-si poate cumpra altfel.
Angela spune c a venit din oras prin parc si cnd a ajuns acas era nsrcinat. Nici nu se putea
pune problema s-si creasc singur copilul. Cine este tatl? Un biat pe care nu-l cunoaste.
Iuliana, spunea (n 97) c stie cine este tatl copilului ei, dar nu poate s-i spun nimic pentru c i-
a dat atunci 5 mii de lei.
Sandocan, pe care l cunoasteti, gzduieste mereu cte un adolescent, fugit de acas si are
reputatie de pedofil....
15
Concluzii
Familia natural trebuie s reprezinte pentru copil mediul firesc si sigur care s-i asigure
cresterea si dezvoltarea. n acest sens, politicile europene n domeniu iar mai nou si cele
nationale se axeaz pe sprijinirea si responsabilizarea familiei n cresterea si educarea copilului.
Analiza datelor rezultate din cercetarea sociologic concret ne permite s formulm cteva
concluzii cu aplicabilitate practic att pentru cercetrile viitoare, ct si pentru decidentii politici
care, n demersul de combatere a srciei, marginalizrii sociale si discriminrii nu pot face
abstractie de un grup social, care nu cuprinde foarte multi indivizi dar care, dac este neglijat,
poate crea multe disfunctionalitti n cadrul societtii, mai ales prin potentialul infractional pe care
l presupune. Este vorba despre tinerii care au fost socializati n institutiile pentru protectia
copilului iar la vrsta de 18 ani sunt furnizati societtii care nu este pregtit s-i integreze.
Cercetarea sociologic realizat n judetul Bihor are un caracter exploratoriu tinnd cont de
faptul c nu a putut fi stabilit un esantion reprezentativ ntruct nu exist o baz de date care s ne
ofere informatii exacte privind tinerii dezinstitutionalizati care s-au stabilit n judet.
Pornind de la ipotezele cercetrii am urmrit cunoasterea vietii din institutii prin prisma
perspectivelor oferite de cei care au trit n acest mediu de socializare. Toti tinerii intervievati au
fost socializati si n institutiile specifice epocii comuniste, dac lum n considerare faptul c au
vrste de peste 20 de ani (cei care au n prezent 20 de ani au petrecut 4 ani n institutiile din
perioada comunist). Ne-am propus de asemenea s completm aceste perspective cu cele oferite
de specialistii care desfsoar sau au desfsurat diferite activitti n care au fost implicati subiectii
analizati.
Referitor la viata din institutii considerm c sunt relevante cteva caracteristici, pe care le
redm n sintez:
Indiferent de perioada n care au fost institutionalizati si indiferent de vrst, opinia
subiectilor privind viata lor din institutii este una favorabil, majoritatea declarnd c au o prere
bun si foarte bun despre viata din institutii. n legtur cu acest fapt am avansat ipoteza
explicativ conform creia, ndeprtndu-se n timp de acest mediu au retinut doar aspectele
pozitive ale vietii din copilria lor. Pe de alt parte, comparnd viata din institutii, care le oferea
hran, adpost si care le satisfcea necesitatea de incluziune si de protectie, cu viata de afar, care
n multe situatii le refuz pn si un umil adpost sau care presupune munc, efort, program etc.
este normal ca viata din institutii s le apar bun si foarte bun. De altfel multi subiecti au declarat
c cele mai mari greutti cu care s-au confruntat au fost cele provocate de plecarea din institutii si
c cel mai mult n viata lor au fost sprijiniti n perioada petrecut n centrele de plasament.
Activittile desfsurate n institutii, de care si amintesc, sunt cele de divertisment
(spectacole, ntreceri sportive, distractii), munca sau nvttura, meditatiile fiind pomenite n foarte
16
putine cazuri, iar activittile de curtenie a ncperilor n care au trit sau de ngrijire a propriului
corp nu au fost amintite niciodat n lista rspunsurilor, la o ntrebare deschis referitoare la tipul
de activitti realizate n institutii Considerm c aceste atitudini dovedesc o slab preocupare a
institutiilor n vederea pregtirii tinerilor pentru viat.
Multi subiecti nu-si cunosc printii naturali si nici nu doresc s-i cunoasc acuzndu-i
pentru faptul c i-au prsit. Tinerii leag relatii puternice ntre ei n institutii, considerndu-se o
familie, ns relativ putini subiecti declar c au avut o relatie de de atasament cu o persoan de
sex opus.
Nivelul de instructie a persoanelor dezinstitutionalizate este n general, sczut, majoritatea
fiind absolventi ai scolii generale sau ai scolilor profesionale care le-au oferit competente minime.
Sunt putini cei care au urmat clase de liceu si mai putini cei care au absolvit liceul fiind integrati n
prezent n nvtmntul universitar. Se constat c, desi au un nivel de instructie sczut si declar
c nu au avut nclinatie pentru nvttur, apreciaz educatia ca un mecanism important al reusitei
n viat, dorind ca proprii copii s urmeze cariere scolare nalte, tocmai pentru a compensa
esecurile personale.
Multi din cei care sunt studenti au rezultate slabe la nvttur, ntruct au studiat n
nvtmntul preuniversitar n clase de nivel mediu sau inferior, n care cerintele erau minime
Competitia cu studentii care au o pregtire normal sau foarte bun i determin s-si
constientizeze valoarea real, ceea ce le induce sentimente de inferioritate, stri de frustrare, n
consecint ajungnd s se automarginalizeze. De multe ori, pentru a obtine calificative de trecere
recurg la invocarea statutului lor de copii din institutii, ceea ce nu-i deosebeste mult de cei care
solicit alte favoruri, invocnd acelasi statut.
Declaratiile privind abuzurile din institutii, senintatea cu care povestesc amnunte despre
modul n care au fost abuzati fizic, psihic si sexual de ctre cei mai mari si de ctre educatori
dovedesc c astfel de comportamente erau considerate ca firesti n viata acestei categorii de
persoane, motiv pentru care le reitereaz cu naturalete si dup iesirea din institutii. Probabil c
abuzurile comise, n special de ctre cei mari asupra celor mici si neajutorati reprezentau o form
de afirmare a superiorittii, de afisare public a calittii de lider a unora.
Lund n analiz rspunsurile la variabila legat de opinia fat de institutiile pentru
protectia copilului, rezult si n aceste cazuri niveluri ridicate ale satisfactiei fat de viata n aceste
institutii. Toate persoanele intervievate au declarat c n ciuda unor inconveniente, de altfel foarte
grave, ca abuzul sexual, violenta, deposedare de bunuri, viata n aceste institutii este una plcut,
relaxant, dar si mai important, ti ofer o anumit sigurant. Este evident c n astfel de situatii,
grilele de valori ale persoanelor institutionalizate difer semnificativ fat de cele ale
macrosocialului; desi ele condamn anumite abuzuri foarte grave care s-au produs n timpul
17
instutionalizrii lor, atitudinea de condamnare este una mecanic, probabil c este mai mult un
rspuns dezirabil la anumite stereotipii sociale. Viata institutionalizat a produs o atenuare a
perceptiei gravittii unor asemenea abuzuri, ele au fcut parte din modelul micro cultural de viat
cotidian a acestor persoane si s-a produs o crestere a permisivittii fat de fapte deviante care au
cptat caracter de normalitate. Pe de alt parte, n logica legitimist-pozitiv a vietii de
institutionalizat, dimensiunea sigurantei zilnice, n raport cu exteriorul incert, capt o important
determinant fat de abuzurile intermitente, considerate normale, prin sistemele de valori
cotidiene ale copiilor institutionalizati.
Deci, am putea concluziona spunnd c sistemele institutionalizate au creat o lume n sine,
micro modele culturale, distincte de restul societtii, caracterizate prin fenomene de atenuare
psihologic a perceptiei fat de gravitatea unor fapte antisociale, iar acest model de reprezentri a
rmas functional si n viata post-institutionalizare. Credem c si printr-o asemenea logic rezidual
a reprezentrilor colective pot fi explicate atitudinile si comportamentele persoanelor post-
institutionalizate (atitudinea fat de munc, educatie, faptele antisociale); ea este generatoarea
unor actiuni sociale a permisivittilor, pe fundalul unor structuri morale n care etica
responsabilittii, n acceptiunea ei macrosocial, este extrem de fluid. Este evident c pentru
aceste persoane legitimarea social a unei asemenea permisivitti comportamentale nu este fcut
prin constientizarea precarittii sistemului lor normativ ci printr-o ideologie a marginalului,
puternic ngrosat legitimist n perioada post-institutionalizare, care gseste n exterior explicatii
pentru a-si legitima statutul social, culpabiliznd sistemul social n care nu se mai poate integra. n
logica lor legitimist, paternalismul institutiilor de ocrotire trebuie prelungit printr-un paternalism
etatist.
Imaginea despre viata din institutii si trsturile de personalitate ale persoanelor care au
fost socializate n acest mediu au fost completate de specialistii intervievati ntregind portretele
persoanelor analizate. Au fost adugate, astfel trsturi specifice de personalitate ale copiilor
socializati n institutii, precum: insatietate, lips de responsabilitate pentru activittile desfsurate
ca si fat de propria lor viat, promiscuitate, cu mare probabilitate de a fi continuat dup iesirea
din institutii, cultivarea, n institutii a relatiilor homosexuale, oferirea modelelor de pedofilie, care
de asemenea vor fi reiterate n viata din afara institutiilor, hiperactivitate, limbaj srac, legnatul
corpului, suptul degetului, ca manifestare a unor frustrri, nempliniri, revolt fat de printii care
i-au abandonat, tendinte de nesupunere, de nclcare a regulilor, incapacitate de efort prelungit, de
a se supune unui regim de viat ordonat care presupune respectarea celuilalt si respectarea unui
program de activitate, un anumit retard n dezvoltarea psihic, naivitate, etc.
n prezent, legislatia romneasc prevede msuri favorabile integrrii acestei categorii
sociale, dup cum am mentionat n lucrare, dar problema tinerilor nu este solutionat, nici pentru
18
cei care n acest an au prsit institutiile, numrul contractelor de solidaritate este mic n raport cu
numrul potentialilor beneficiari.
Summary
Effects of Institutionalization on Children. Case study in Bihor County.
This paper proposes a brief history of the child institutionalization in Romania. Also, we present the
resulting aspects of the social research we carried out in Bihor County, about the characteristics of life in
the Romanian child institution system, in the opinion of participating persons.
Bibliografie
Boudon R., L, Inegalite de chances. La mobilite sociale dans les societes industrielles, Hachette, Paris,
1973;
Bowlby J., Attachment and loss, Vol. I si Vol. II, Penguin Books, London, 1944;
Godfarb W., Emotional and Intellectual Conseqences of Psiychologic deptivation in infancy: a
revaluation, Hoch P, Zubin J, eds. Psichopathology of childhood. NY: Grune & Stratton, 1955;
Sutherland, E., Cressey, D. R., Principes des criminologie, Editura Cujas, Paris, 1966;
Zamfir, C. (coord.), Pentru o societate centrat pe copil, Editura Alternative, Bucuresti, 1997;
Zamfir, C., Stoica, L. (coord.), O nou provocare: dezvoltarea social, Editura Polirom, Iasi, 2006;
Autoritatea National pentru Protectia Drepturilor Copilului, www.copii.ro
Directia General de Asistent Social si Protectia Copilului, http://sas. mmssf.ro/
Acte normative interne i internaionale:
Convenia cu privire la Drepturile Copilului, adoptat de Adunarea General ONU la 20 noiembrie 1989,
intrat n vigoare la 2 septembrie 1990 si ratificat de Romnia prin Legea nr.18/1990 publicat n
Monitorul Oficial nr.109 din 28 septembrie 1990;
Convenia european n materia adopiei de copii, ncheiat la Strasbourg la 24 aprilie 1967 si la care
Romnia a aderat prin Legea nr.15/25 martie 1993 publicat n Monitorul Oficial nr.67 din 31 martie 1993;
H.G. nr. 679 din 12 iunie 2003 privind condiiile de obinere a atestatului, procedurile de atestare i
statutul asistentului maternal profesionist, publicat n Monitorul Oficial, nr.443 din 23 iunie 2003;
Legea nr. 47 din 1993 cu privire la declararea judectoreasc a abandonului de copii, publicat n
Monitorul Oficial al Romniei, Partea I, nr. 153 din 8.07.1993;
Legea nr. 67 din 1995 privind ajutorul social, publicat n Monitorul Oficial al Romniei, Partea I, nr.131
din 29 iunie 1995;
Legea nr. 275 din 2004, pentru modificarea O.U.G. nr. 12 din 2001, privind nfiintarea Autorittii
Nationale pentru Protectia Copilului si Adoptie, publicat n Monitorul Oficial, nr. 557 din 23 iunie 2004;
Legea nr. 47 din 8 martie 2006 privind sistemul naional de asisten social, publicat n Monitorul
Oficial nr.239 din 16 martie 2006;
O.U.G nr.26 din 1997 privind protecia copilului n dificultate publicat n Monitorul Oficial nr.120 din
1997, aprobat prin Legea nr. 108/1997 publicat n Monitorul Oficial nr. 205 din 1998;
Ordonana de urgen nr. 44 din 14 iunie 2006, publicat n Monitorul Oficial al Romniei nr. 545 din 23
iunie 2006.
Primit 12.11.2008
19
Protecia drepturilor copilului aflat n dificultate n Romnia
Lavinia Onica-Chipea, Floare Chipea i Simona Stanciu, Universitatea din Oradea, Romnia
1. Politici de protectie a copilului abandonat n regimul comunist n Romnia
2. Politici de protectie a copilului aflat n dificultate dup anul 1989
1. Politici de protecie a copilului abandonat n regimul comunist
n Romnia
Regimul comunist a lsat n privinta statutului copilului i a mamei o situaie extrem de
contradictorie. Cu obsesia de a crea o nou societate si un om nou, regimul comunist a
acordat de la nceput o atentie special copilului si tinerei generatii. Intentia de a modela copilul
social-politic si moral, n spiritul ideologiei proprii, a fost dublat de o investitie masiv de resurse
n conditiile de viat ale acestuia. ntr-o perioad istoric relativ scurt s-a cristalizat un sistem
generos de protectie social a copilului si familiei cu copii, subventionarea masiv a bunurilor
pentru copii, distribuirea cu prioritate a locuintelor familiilor cu copii, dezvoltarea unui sistem de
servicii necesare copiilor: crese si cmine, grdinite, scoala obligatorie si gratuit, tabere de
vacant, activitti culturale si sportive, sistem de ngrijire medical corespunztor (Zamfir C.,
Zamfir, E, 1995, pp.120-121); reducerea de impozite, alocatii pentru copil care cresteau progresiv
cu numrul copiilor. Mai mult, n primii ani ai regimului comunist s-au atribuit copilului si familiei
cu multi copii resurse substantiale, fapt ce avea s aib ca rezultat pozitiv mbunttirea rapid a
conditiilor de viat ale copilului, mult mai mult dect pentru celelalte segmente ale populatiei. Ea a
creat o destul de ridicat egalitate a sanselor si n unele situatii (de exemplu n cazul admiterii n
nvtmntul superior), chiar o discriminare mpotriva copiilor proveniti din alte medii dect cele
muncitoresti si trnesti. Romnia a adoptat de fapt, nc din 1953, Codul familiei, act normativ n
vigoare si n prezent, cu modificrile ce i-au fost aduse; pentru anii 1953 actul normativ de
reglementare a situatiei familiei si, implicit a statutului copilului n familie, drepturilor si
obligatiilor printesti, drepturilor de care se bucur copilul n familie venea s ofere sperante n
legtur cu locul important pe care statul l acord familiei si copilului. De altfel, existenta n
cadrul aceluiasi act normativ a reglementrilor legate de familie, stare civil, cstorie, desfacerea
cstoriei, copil, ocrotirea copilului, adoptie, rudenie, filiatie, situatia legal a copilului, tutela,
curatela, autoritatea tutelar, demonstreaz abordarea unitar a familiei si copilului, orientarea
progresist pentru aceea perioad si preluarea cu responsabilitate a reglementrilor unor
documente internationale referitoare la aceast problematic si existente n momentul respectiv.
20
Modernizarea societtii romnesti, rapida ei urbanizare, combinat cu standardul de viat
sczut, au produs un declin continuu al natalitii, care a ajuns n 1966 la un nivel foarte sczut.
Regimul a suprareactionat la aceast tendint apelnd la un mijloc brutal si anume interzicerea
avorturilor prin Decretul 770/1966 si descurajarea utilizrii oricror procedee moderne de
control al naterilor. Cresterea numeric a populatiei nu s-a realizat ns. Femeile au recurs la
metode empirice de ntrerupere a sarcinilor, ceea ce a dus la creterea ratei deceselor materne si a
mortalitii infantile. Valul cresterii nasterilor atinge nivelul maxim n 1967 si prima parte a anului
1968, cnd indicele conjunctural al fertilittii creste la 3,6 fat de 1,9 n 1966, dup care se
nregistreaz o continu scdere pn n 1985, cnd prin Decretul 410/1985 s-a ncercat
reafirmarea politicii pronataliste fortate, dar care nu a dat rezultate. Rata mortalittii materne a
ajuns n 1990 la 263 decese nregistrate la 100.000 nasteri vii, ceea ce a plasat Romnia, pn n
1991, pe primul loc n privinta deceselor materne n Europa. Aceeasi situatie s-a nregistrat n
privinta mortalittii infantile, care desi n scdere fat de 1970, nregistra n 1990, 26,9.
Situatia economic a Romniei s-a deteriorat progresiv si a devenit vizibil si simtit tot mai
violent prin scderea nivelului de trai al populatiei care s-a nruttit din ce n ce mai mult dup
1980. Scderea dramatic a performantelor economice s-a reflectat n deteriorarea conditiilor de
viat si a calittii serviciilor pentru copil si familie. Suportul statului pentru familie si copil s-a
diminuat treptat dup 1970 dar a cunoscut o scdere mai accentuat dup 1980. n anul 1985, statul
a ncercat o rennoire a politicii pro-nataliste si a emis un Decret Lege care acorda o serie de
drepturi financiare de suport pentru familie si copil. Alocaia de stat pentru copil era acordat unei
categorii mai mari de beneficiari dar era n continuare inaccesibil copiilor ai cror printi nu erau
angajati n ntreprinderile de stat (nu primeau alocatii de stat pentru copii printii care erau angajati
ai ntreprinderilor mestesugresti sau ai cooperativelor agricole de productie). Au fost acordate
alocaii financiare pentru soiile militarilor n termen, gravide dup luna a V-a de sarcin si erau
atribuite alocaii pentru mamele cu muli copii (alocatii viagere pentru mamele care au avut n
ntretinere de la un numr de 3 copii n sus).
Situaia copilului aflat n dificultate a cunoscut ns, n perioada 1970-1990, cea mai
drastic depreciere. Ca urmare a cresterii numrului de familii care nu mai puteau sau nu mai
doreau s-si ndeplineasc functiile de crestere si educare, Guvernul a adoptat n 1970 principalul
act normativ privind protectia copilului aflat n dificultate si anume Legea nr.3/1970 privind
regimul ocrotirii unor categorii de minori. Analizat n contextul anilor 70, aparitia acestei legi a
coincis cu perioada baby boom care a urmat Decretului 770 din octombrie 1966 ce interzicea
ntreruperile voluntare ale sarcinii. Se impunea atunci o solutie pentru contracararea numrului
mare de copii nedoriti. Justificat prin nevoi reale si pertinente, Legea nr.3/1970 introducea cel mai
aberant sistem de protectie a copilului aproape exclusiv institutionalizat care avea s lase urme
21
asupra dezvoltrii copilului, dimensionrii sistemului, efortului financiar, care nici dup 10 ani de
la schimbarea regimului care l-a introdus nu s-au sters: copii care la mplinirea vrstei de 18 ani
erau lsati n strad fr a avea o pregtire suficient pentru viata independent si nici resursele
materiale sau financiare pentru a se descurca. S-a realizat de fapt o socializare deficitar a acestora
prin lipsa unei perspective asupra vietii adulte (Zamfir, C., 1997, pp. 96-97); persoane care datorit
institutionalizrii prelungite nu au mai prsit niciodat sistemul, devenind asistati pe viat ai
institutiilor pentru persoane cu handicap; un sistem supradimensionat de institutii, cu sute de
locuri, prost ntretinute si dotate, cu conditii de viat precare, de multe ori construite n zone greu
accesibile, departe de ochii populatiei; un personal neinteresat n cea mai mare parte de situatia
copiilor pe care trebuiau s-i protejeze si care a ntretinut sistemul si o dat cu el privilegiile lui
mai mult de 30 de ani; ntrzieri mentale, fizice si emotionale, traumatisme psihologice-emotionale
grave, distorsiuni n personalitatea copiilor.
Mai mult, pornind de la estimarea c n cazul copiilor mici este nevoie n principal de
ngrijire medical, leagnele (copii 0-3 ani) erau organizate dup principii medicale. Subordonarea
lor Ministerului Snttii nu era ntmpltoare. Ele semnau mai mult cu spitalele, copiii fiind
uneori siliti s-si petreac cea mai mare parte a timpului n pat, n camere uriase cu 10-50 copii,
primind hran si medicamente, dar fiind aproape ignorati din punct de vedere social si psiho-
afectiv. Medicalizarea nu era att efectul unei conceptii gresite, ci mai degrab efectul unui proces
real de degradare a conditiilor de viat: scderea resurselor alocate si a numrului de angajati.
Copiii de peste 3 ani, pe lng hran si mbrcminte, se presupunea c trebuie s primeasc,
n primul rnd, educatie n scoal/grdinit care erau ncorporate n casele de copii. Casele de copii
erau subordonate Ministerului nvtmntului. Ambianta uman att de vital pentru dezvoltarea
normal a copilului lipsea, cele mai multe forme de organizare social, ntrite de conditiile
obiective (cldiri improprii, personal putin si fr calificare de tip social) erau forme primitive,
quasi-militare, adesea de tipul nchisorii. Institutiile erau nchise publicului, accesul era permis
doar unui numr restrns de vizitatori, care venea din partea unor organisme locale, medicale,
politice, etc. care de fapt sprijineau puterea central. Rareori veneau printii copiilor internati s-si
viziteze copiii, atmosfera din institutii era adesea caracterizat prin lips de participare a copiilor,
subordonare si pedepse chiar abuzuri psihice si fizice asupra copiilor. Toate acestea n situatia n
care institutiile pentru copii trebuie s reprezinte, mai nainte de toate, un substitut al familiei, un
mediu socio-emotional vital pentru dezvoltarea copiilor.
De asemenea scopurile declarate ale retelei de ocrotire a copiilor de ctre stat distonau
puternic cu cele realizate n concret (Roth-Szamoskzi, M., 1999, p.218).
Tabel nr. 1: Scopuri declarate si realizarea lor n cadrul retelei de ocrotire a copilului de
ctre stat nainte de 1989
22
1.Scopuri declarate i realizarea lor nainte de 1989
asigurarea unui adpost, dar
aglomerat, fr asigurarea unui spatiu
personal
adpost, dar lipsit de confort
satisfacerea necesittilor
biologice
necesittile biologice au fost
satisfcute la standarde minime
educatie principal
(comunist), bazat pe rolul
colectivittii
educatie nediferentiat
educatie si instruire
specializat, care s pregteasc copiii
pentru viat
educatie orientat n mic
msur ctre integrarea copiilor n
viata social
asigurarea unei dezvoltri
armonioase a personalittii copiilor
frecvente cazuri de tulburri
de personalitate, dizarmonii
suplinirea lipsei familiei abordarea impersonal a
copiilor, hospitalism
evaluarea capacittilor
intelectuale ale copiilor si orientarea
lor scolar corespunztoare
diagnostice de multe ori
superficiale, chiar gresite
Noua lege de protectie a copilului (3/1970) oferea protectie urmtoarelor categorii de minori
(Comnescu, I., Mihut, I., Petrescu, R., 1989, pp.234-235):
a) copii cu printi decedati, necunoscuti, sau n orice alt situatie care duce la
instituirea tutelei, dac acestia nu dispun de bunuri sau alte mijloace materiale proprii si nu exist
persoane care s aib, potrivit legii, obligatii de ntretinere pentru copil;
b) copii care fiind deficienti, au nevoie de ngrijire special ce nu le poate fi asigurat
n familie;
c) copii a cror dezvoltare fizic, moral, intelectual sau stare de sntate este
primejduit n familie;
d) copii care au svrsit fapte prevzute de legea penal, dar nu rspund penal sau sunt
expusi s svrseasc asemenea fapte, ori ale cror purtri sunt n pericol s contribuie la
rspndirea de vicii sau deprinderi imorale n rndul altor minori.
Legea pentru protectia copilului n dificultate, prevedea pentru prima dat n Romnia,
organizarea la nivel judetean sau a municipiului Bucuresti, a Comisiei pentru Ocrotirea Minorului,
organism administrativ cu atributii n luarea msurilor de protectie pentru copilul aflat n
dificultate, cu exceptia plasamentului familial (care putea fi hotrt de Oficiul de asisten
social), urmrirea aplicrii msurilor si a modului de dezvoltare a copilului protejat si schimbarea
msurilor de protectie n functie de situatia familiei si a copilului. Organizarea Comisiilor pentru
Ocrotirea Minorilor era imaginat conform acestei legi la trei nivele: central (Comisia Central
pentru Ocrotirea Minorului), judetean (Comisia Judeean pentru Ocrotirea Minorului) si
municipal sau orsenesc (Comisia Municipal pentru Ocrotirea Minorilor) organizate prin
decizia Comisiei Centrale pentru Ocrotirea Copilului. La nivel national, pentru ndrumarea si
23
coordonarea activittii de protectie functiona Comisia Central pentru Ocrotirea Minorilor, la
nivelul Ministerului Muncii.
Legea instituit n 1970 prevedea, asa cum am mentionat anterior, si separarea competentelor
privind hotrrea msurilor de protectie a copilului n dificultate. Competenta atribuirii msurii
plasamentului familial era dat organului de asistent social, Oficiul de asisten social din
cadrul Directiei Muncii si Ocrotirii sociale al consiliului judetean sau al Municipiului Bucuresti.
Luat cu acordul printilor sau tutorelui pentru copilului ai crui printi erau decedati, necunoscuti
sau a cror sntate era primejduit n familie, aceast msur temporar poate fi considerat, ca o
actiune de prevenire, care evita ncredintarea copilului unei institutii de ocrotire. Practic, nainte de
1990, msura plasamentului era singura msur alternativ pentru protecia copilului n
dificultate si se realiza de regul n cadrul familiei extinse. Din pcate, servicii de specialitate care
s urmreasc evolutia copilului n familia de plasament nu existau, Oficiul de asistent din cadrul
Directiei de Munc si Ocrotiri Sociale Judetene sau a Municipiului Bucuresti se limita, dup
acordarea hotrrii de plasament, numai la plata alocatiei de ntretinere care era prevzut de lege
n cazul n care persoana sau familia la care minorul era plasat, nu avea obligatia de ntretinere
conform Codului familiei.
La aceast situatie se adugau dou alte elemente deosebit de importante. Primul si cel mai
important se refer la pregtirea profesional a personalului acestor organe teritoriale de asistent
social. n 1969, deci cu un an naintea intrrii n vigoare a acestei legi, care prevedea atributii de
asistent social, Ceausescu decidea nchiderea scolii romnesti de asistent social, care desi
insuficient dimensionat, avea deja o reputatie n privinta calittii pregtirii, sub motiv c, n
Romnia, nu ar mai exista probleme sociale sau dac acestea exist pot fi rezolvate numai la
nivelul Comitetelor obstesti teritoriale. De astfel, ndrumrile elaborate pentru aplicarea
acestei legi, prevedeau sprijinul autorittii tutelare, a colectivelor de sprijin pentru asistent social,
a comisiilor de femei, precum si a altor organizatii obstesti pentru urmrirea dezvoltrii din punct
de vedere fizic, moral si intelectual a minorilor fat de care s-au luat o msur de protectie.
Aceast situatie a dus la deprofesionalizarea serviciilor si transformarea lor n simple prestatoare
de alocatii financiare. Un recensmntul realizat n anul 1990 privind numrul absolventilor de
scoli de asistent social activi, a consemnat existenta numai a unui numr de 200 de persoane
calificate, multe dintre ele refugiate n sistemul de sntate ca asistente de ocrotire.
O alt problem care ngreuna urmrirea unei msuri de protectie ntr-un cadru institutional
era numrul limitat de posturi aferent unui oficiu judetean de asistent social. Astfel, numrul de
posturi, care era corelat cu numrul locuitorilor unui judet era ntre dou si cinci posturi/judet.
Teoretic, Comisiile pentru Ocrotirea Minorilor puteau hotr msura ncredinrii n familie
pentru minorii care nu au putut fi plasati n familii, fie din cauza neidentificrii unei familii care s
24
prezinte garantii materiale, morale, de sntate si s accepte luarea unui copil n plasament, fie din
cauza nendeplinirii altor conditii, cum ar fi acceptul printilor copilului prin deciziile serviciilor
de asistent social. Practic, msura era cvasi ignorat din lipsa serviciilor sociale de specialitate si
a specialistilor, ca si n cazul plasamentului familial.
Pentru minorii care nu puteau fi plasati sau ncredintati n familii si minorii cu deficiente,
Comisiile pentru Ocrotirea Minorului puteau decide ncredinarea lor pentru cresterea, educarea,
pregtirea scolar si profesional n instituii de ocrotire, organizate n subordinea diferitelor
ministere tehnice (Ministerul Muncii si Ocrotirii Sociale, Ministerul nvtmntului, Ministerul
Snttii), n functie de vrst, deficient, grad de handicap, astfel:
Leagne pentru copii n vrst de pn la 3 ani care necesit protectie n afara familiei
naturale sau pentru minorii cu deficiente n sectii organizate diferentiat;
Case de copii pentru precolari i colari care necesit protectie n afara familiei
biologice;
Grdinie pentru copii deficieni recuperabili n vrst de peste trei ani pn la ncadrarea n
scoala general;
coli generale pentru deficieni recuperabili n vrst scolar (cu exceptia celor cu
deficiente locomotorii accentuate);
Licee de cultur general pentru deficienii recuperabili, absolventi ai scolii generale;
coli profesionale pentru deficieni recuperabili, absolventi ai scolii generale sau care au
ntrerupt nvtmntul obligatoriu sau nu l-au frecventat si au depsit vrsta de 14 ani;
Licee de specialitate pentru deficieni recuperabili absolventi ai scolii generale;
Cmine coal pentru deficieni oligofreni, partial recuperabili care primesc instruire n
limita posibilittilor intelectuale, precum si pentru deficienti motori cu infirmitti grave care
urmeaz cursurile de cultur general dup regimul scolilor din nvtmntului de mas;
Cmine atelier pentru deficieni partial recuperabili n vrst de peste 16 ani;
Cmine pentru deficieni nerecuperabili care nu pot presta nici un fel de activitate.
Cheltuielile necesare pentru protectia copiilor n institutii au fost n toat aceast perioad
suportate de la bugetul de stat iar persoanele care aveau obligatii de ntretinere pentru copiii
ncredintati institutiilor de protectie erau obligate pn n 1990, de ctre Comisia pentru Ocrotirea
Minorului, s contribuie lunar, n functie de venitul lor mediu, la ntretinerea copilului pe toat
durata msurii de protectie, conform Decretului 253/1971 privind contributia de ntretinere n
unele institutii scolare.
Sistemul de protectie a copilului, n special cel referitor la protectia copilului n dificultate, a
constituit sistemul cel mai criticat dup 1990 si care si-a dovedit ineficienta att din punct de
vedere al respectrii drepturilor copilului ct si din punct de vedere al costurilor bnesti sau
25
sociale. Perioada 1970-1990 a reprezentat, n special n anii 80, perioada neagr din istoria
Romniei, care a acumulat indicatori demografici si ai strii de sntate pentru copil si femeie care
au plasat-o pe primul loc n Europa din punct de vedere al neglijrii acestor categorii sociale.
1. Politici de protecie a copilului aflat n dificultate dup 1989
n Romnia
Specialistii, forurile internationale guvernamentale si neguvernamentale se asteptau ca
imediat dup 1990, situatia copilului n general, dar mai ales cea a copilului n dificultate s se
schimbe rapid si fundamental. Scurta perioad de schimbri pozitive a durat aproximativ 2 ani.
Astfel, imediat dup decembrie 1989, Guvernul Romniei a dus o politic de reparare a greselilor,
inegalittilor si frustrrilor suferite si acumulate de populatie, cu precdere dup 1980. Se poate
deci considera c, politica social a Romniei n 1990 a fost o politic reparatorie (Zamfir, E.,
Zamfir, C., 1995, p. 122).
Trei directii importante au vizat politica social reparatorie a anilor 1990: protectia familiei,
politica locuintelor, protectia copilului institutionalizat.
n acest interval relativ scurt, s-au luat msuri de crestere a numrului de angajati n institutii,
egalizare a alocatiilor pentru copii din mediul rural si pentru cei din mediul urban, acceptarea de
ajutoare internationale si organizarea asistentei profesionale de protectie a copilului cu
introducerea unor metode noi, pe cheltuiala organizatiilor strine. Urmarea acestor msuri a fost
reducerea numrului de copii din instituii, paralel cu un mare val de adopii internaionale legale
i mai ales ilegale. Impactul importantului interes al strinttii pentru copii prsiti si orfani,
victime ale legii de interzicere a avorturilor din perioada Ceausescu, a dus la ameliorarea calitii
vieii n aceste instituii, precum si a sistemului local de protectie a copilului (Roth-Szamoskzi,
M., 1999, p.28).
Din 1989 si pn n 1997, prima etap din politica public de protectie a copilului, statul s-a
preocupat de modificarea parial a cadrului normativ i administrativ de ocrotire a minorului.
Dar, lipsa unei strategii nationale n materia protectiei copilului a fcut dificil si activitatea
actorilor privati, precum organizatiile neguvernamentale (Mihilescu, I., 2000, p.145).
Cadrul legislativ se modific prin adoptarea Conveniei cu privire la drepturile copilului
(Legea 18/1990 de ratificare a Conventiei) dar fr urmri n ceea ce priveste modificarea Legii
3/1970, conform reglementrilor si principiilor cuprinse n conventie. n ceea ce priveste situatia
copilului n dificultate, imediat dup 1990 numrul copiilor protejati n institutii rezidentiale a
nregistrat o scdere explicabil prin numrul mare de adoptii din anii 1990-1991 dar si prin
efectele abrogrii decretului privind interzicerea ntreruperilor de sarcin. n timp ns, nruttirea
conditiilor de viat n Romnia, srcia, cresterea numrului de persoane fr loc de munc, lipsa
26
de educatie si a programelor de planificare familial, lipsa serviciilor sociale la nivelul tuturor
judetelor a determinat creterea numrului de copii internai n instituii. Decizia institutionalizrii
copilului, desi nu era singura msur ce putea fi luat, rmne n continuare majoritar, cu toate c
ncredintarea si plasamentul ntr-o familie erau msuri reglementate expres de actul mentionat. A
crescut n aceeasi perioad de timp numrul copiilor internati n institutii de protectie pentru
copilul cu handicap att n institutiile clasice, cmine spital, ct si n institutii mascate care desi se
declarau institutii medicale protejau n acelasi timp copii cu probleme sociale, sectii de recuperare
pediatric, neuropsihiatrie infantil, HIV/SIDA etc.
Pn la nceputul anului 1997 (cnd adoptarea O.U.G. nr.26/1997 privind protecia copilului
n dificultate determin abrogarea expres a Legii 3/1970), sistemul de protectie a copilului n
dificultate, instituit n anul 1970, a rmas nemodificat, desi ncepnd cu anul 1990, o dat cu
schimbarea regimului politic, Romnia si afirmase intentia unei transformri prin ratificarea n
1990 a Conveniei O.N.U. privind drepturile copilului. Ratificarea acestei Conventii ONU a atras
dup sine includerea n Constitutia Romniei a principiilor care garanteze libera dezvoltare a
personalittii umane: Copiii se bucur de un regim special de protectie si asistent n realizarea
drepturilor lor;
Comisia pentru Ocrotirea Minorului (COM), instanta administrativ autorizat s hotrasc
adoptarea unei msuri de protectie a copilului, avea posibilitti de decizie limitat. Vechea lege nu
privea nici o form de sprijin a familiei naturale pentru prevenirea institutionalizrii copilului.
Acest sistem aberant care s-a pstrat aproximativ 30 de ani si care a nclcat n toat aceast
perioad drepturile copilului, n special dreptul de a fi crescut si educat n familie, a gzduit
anual aproximativ 50.000 de copii n institutii de protectie: leagne, case de copii, cmine spital
(Alexiu, M.,T.,Clive, S., 2000, p.95).
O dinamic a numrului copiilor din institutiile rezidentiale de protectie n perioada 1990-
1997 se prezint astfel:
Tabel nr. 2: Dinamica numrului copiilor din institutiile rezidentiale n perioada 1990-1997
Sursa: Departamentul pentru Protectia Copilului
Cresterea numrului de copii din institutii a determinat Guvernul s caute solutii permanente
pentru copil. Astfel, n anul 1990 a fost adoptat Legea nr.11 privind ncuviinarea adoptiei pe care
Tipul
instituiei
1990 1991 1992 1993 1994 1995 1996 1997
Leagn 8286 7968 9979 8442 8555 8622 9863 9309
Casa de
copii
28954 26144 29021 30746 33431 33431 31960 35165
Cmin
spital
3354 3617 4204 4349 3940 4586 4130 4473
27
a modificat-o n anul 1991 avnd n vedere necesitatea alinierii la Conventiile internationale n
materie, care presupuneau acorduri ntre statele care conveneau s colaboreze n materia adoptiei,
urmrirea si raportarea situatiei copilului n tara adoptatoare pe o perioad de doi ani (Legea nr.11
din 1990 privind ncuviinarea adopiei republicat n Monitorul Oficial nr.159 din 26 iulie 1991).
Paralel cu adoptarea actului normativ mentionat si datorit cresterii masive a numrului adoptiilor
internationale n aceast perioad, fenomen care a devenit aproape imposibil de controlat, s-a
hotrt nfiintarea prin H.G. nr.63/1991 a Comitetului Romn pentru Adopii (CRA) n scopul
supravegherii si sprijinirii actiunilor de ocrotire a minorilor prin adoptie si al realizrii cooperrii
internationale n aceast materie (extras din Legea 11/1990, modificat si republicat n 1991).
Pentru mbunttirea activittii de adoptie, Romnia ader prin Legea 100/1992 la Convenia de la
Haga asupra aspectelor civile ale rpirii internaionale de copii si ulterior ratific Convenia
asupra proteciei copilului i cooperrii n materia adopiei internaionale Haga (Legea
15/1993, respectiv Legea 84/1994). Totodat pentru a putea fi solutionat o problem cum este cea
a abandonului copiilor n institutii, se instituie prin Legea 47/1993, declararea judectoreasc a
abandonului (Legea nr. 47 din 1993 cu privire la declararea judectoreasc a abandonului de
copii, publicat n Monitorul Oficial al Romniei, Partea I, nr. 153 din 8.07.1993). Desi
controversat, legea si gseste aplicatie prin aceea c pentru un mare numr de copii cei
abandonati - se poate apela la o alt msur dect institutionalizarea.
Situatia economic din ce n ce mai deteriorat si ca urmare nivelul de trai al populatiei din
ce n ce mai sczut a determinat adoptarea n 1993 a Legii 61/1991 privind alocaia de stat pentru
copii, care instaura principiul universalittii si instituia copilul ca beneficiar al alocatiei (Legea
nr.61 din 1993 privind alocaia de stat pentru copii republicat, publicat n Monitorul Oficial
nr.56/08.02.1999). Din pcate nici aceast intentie bun nu a putut fi sustinut financiar si nu a
putut fi corelat cu inflatia. Aceasta a determinat scderea valorii reale a alocatiei de stat pentru
copii transformnd-o ntr-un simbol si nicidecum ntr-o form de protectie si a situat Romnia
printre ultimele tri din regiune n privinta acestei alocatii bugetare.
n perioada 1997-1999, guvernul a decis schimbarea cadrului normativ i administrativ
pentru protecia copilului aflat n dificultate si a elaborat o nou strategie de protecie a acestuia
centrat pe protectia copilului n familie sau ntr-un cadru ct mai apropiat de mediul familial, n
detrimentul protectiei n institutiile rezidentiale. Strategia elaborat a vizat reforma cadrului juridic
si administrativ de protectie a drepturilor copilului, descentralizarea activittii de protectie,
restructurarea si diversificarea institutiilor de ocrotire a copilului n dificultate, dezvoltarea
alternativelor de tip familial la ocrotirea rezidential, prevenirea prenatal a abandonului, cresterea
rolului societtii civile n activitatea de protectie a drepturilor copilului.
28
Intervalul 1997-1999 poate fi definit ca perioad care a marcat realizarea reformei sistemului
de protecie a copilului aflat n dificultate. Desi schimbrile nu au cuprins dect domeniul
protectiei copilului aflat n dificultate, ele au permis crearea premiselor pentru constituirea unui
sistem descentralizat care s rspund nevoilor copilului n general.
Reforma cadrului normativ n protectia copilului a impus abrogarea Legii 3/1970 privind
regimul ocrotirii unor categorii de minori si a Legii 11/1990 privind ncuviinarea adopiei. n
iunie 1997 au fost adoptate OUG nr.26 privind protecia copilului n dificultate si OUG
nr.25/1997 cu privire la adopie; noile acte normative au stat la baza crerii noului sistem
descentralizat de protectie a copilului, la elaborarea noilor msuri de protectie a copilului n
dificultate (prin copil n dificultate ntelegndu-se conform legii copilul a crui dezvoltare,
integritate fizic sau moral este periclitat) si a actorilor institutionali pentru hotrrea, aplicarea
si urmrirea acestor msuri (Comisia pentru Protecia Copilului, Serviciul Public judeean sau
de sector a Municipiului Bucureti, Organismelor private Autorizate de Comisia pentru Protecia
Copilului s desfsoare activitti de protectie a copilului, Comitetul Romn pentru Adopii). A fost
de altfel realizat un parteneriat ntre autorittile centrale si cele locale pentru sustinerea activittilor
de prevenire a situatiilor de risc pentru familie si de protectie a copilului aflat n dificultate prin
alocarea de fonduri, initierea de servicii specializate si recrutarea de personal calificat pentru
sustinerea acestor activitti.
Ordonanta de Urgent a Guvernului nr.26/1997 privind protectia copilului n dificultate
stabileste msuri de protectie a acestuia si asigur aplicarea lor corespunztoare prin serviciul
public pentru protectia copilului sau printr-un organism privat autorizat s desfsoare activitti de
protectie a acestuia: ncredintarea copilului unei familii, unei persoane sau unui organism privat
autorizat; ncredintarea copilului n vederea adoptiei; ncredintarea provizorie a copilului ctre
serviciul public specializat; plasamentul copilului la o familie sau la o persoan; plasamentul
copilului la un serviciu public specializat sau organism privat autorizat; plasamentul copilului n
regim de urgent; plasamentul copilului la o familie asistat. Pentru prima dat este introdus ntr-
un act normativ romnesc (OUG nr.26/1997) plasamentul / ncredintarea copilului aflat n
dificultate la asistentul maternal profesionist, oferindu-se astfel posibilitatea protectiei copilului
prin alternative de tip familial la ocrotirea institutionalizat. H.G. nr. 218 din 1998 cu privire la
condiiile de obinere a atestatului de asistent maternal profesionist, abrogat ulterior prin H.G.
nr.679 din 12 iunie 2003, coroborat cu OUG nr.26/1997 pune bazele juridice ale noii alternative
de protectie a copilului ntr-un cadru familial. Profesia este asimilat cu cea de foster care sau
famille d accueil (Alexiu, T.M., 2000, p.25) care este foarte rspndit n tri cu experient n
protectia copilului si a fost introdus n Nomenclatorul Functiilor si Ocupatiilor din Romnia prin
Ordinul comun al Ministerului Muncii si Protectiei Sociale si Ministerul Educatiei Nationale,
29
publicat n Monitorul Oficial al Romniei nr.374 din 23.12.1997.
Desi, din cauza conditiilor economice, numrul de cereri de instituionalizare si protectie a
copiilor de ctre stat a crescut la peste 44.000 anual (numrul cererilor de sprijin adresate
serviciilor publice pentru protectia copilului a crescut cu 12% n 1998 comparativ cu aceeasi
perioad a anului 1997, datorit degradrii conditiilor socio-economice), rata instituionalizrii a
sczut prin actiunile de prevenire a institutionalizrii si/sau intrarea acestuia ntr-o situatie de risc
si prin protectie n alternative familiale, respectndu-se astfel interesul superior al copilului. Astfel,
de exemplu, numrul copiilor institutionalizati a sczut de la 98.872 n mai 1997 la 91.785 n iunie
1998 iar numrul celor protejati n familii, a crescut de la 11.081 n 1997 la 44.171 n iunie 1998.
De asemenea, dintr-un total de 44.679 cazuri noi intrate n sistem ntr-un an, noile Comisii pentru
Protectia Copilului au dat decizii de institutionalizare a copiilor n peste 8.514 cazuri, iar ceilalti
36.165 copii au fost mentinuti n propriile familii sau au fost protejati n familii substitutive
(Alexiu, T.M., 2000, p.101).
O situatie a protectiei copilului aflat n dificultate, conform cadrului legal, n perioada 1997-
1999 se prezint astfel:
Tabel nr. 3: Situatia protectiei copilului n dificultate n perioada 1997-1999
Sursa: DPC, MEN, SSPH
Tipuri msuri de
protecie
Instituia responsabil Numr beneficiari
Plasament/ncredintare n
centre de plasament
publice
Consiliul Judetean/ Serviciul
public specializat pentru protectia
copilului
35.013
Plasament/ncredintare n
centre de plasament
private
ONG
2.597
Plasament n cmine-
spital
Secretariatul de Stat pentru
Persoane cu Handicap
3.497
Total copii protejati n
institutii rezidentiale
41.089
Plasament/ncredinatare
n familii
Servicii publice specializate
pentru protectia copilului
19.793
Beneficiari ai
activittilor de prevenire
Servicii publice specializate
pentru protectia copilului
11.087
Copii n nvtmntul
special
Ministerul nvtmntului 52.444
Total copii n dificultate
120.076
Numr servicii noi
nfiintate
Servicii publice specializate
pentru protectia copilului
180
30
Prin Strategia Naional de dezvoltarea a sistemului pentru protecia copilului adoptat de
Guvernul Romniei n iulie 2000, Agentia National pentru Protectia Drepturilor Copilului si-a
propus continuarea procesului de creare a unui nou sistem de protecie a copilului care s
favorizeze protectia copilului alturi de familia sa sau ntr-un cadru ct mai apropiat de modelul
familial. Dintre obiectivele strategiei amintim: restructurarea serviciilor si institutiilor de tip
rezidential existente si reorientarea utilizrii resurselor existente pentru diversificarea de servicii
alternative la ngrijirea rezidential; mbunttirea/armonizarea cadrului legislativ necesar
organizrii si functionrii sistemului de protectie a drepturilor copilului; crearea si dezvoltarea unui
sistem national de monitorizare si evaluare a situatiei copilului n dificultate sau n situatie de risc,
a activittii serviciilor si institutiilor de ngrijire si protectie a drepturilor copilului, a resurselor
financiare disponibile, avnd capacitatea de a prevedea eventualele crize bugetare ale sistemului de
protectie a copilului; ntrirea capacittii institutionale a Agentiei Nationale pentru Protectia
Drepturilor Copilului; sustinerea dezvoltrii capacittii institutionale a autorittilor administratiei
publice locale; dezvoltarea resurselor umane care intervin n sistemul de protectie a drepturilor
copilului, prin definirea si promovarea statutului su profesional; promovarea participrii societtii
civile la dezvoltarea sistemului national de protectie a drepturilor copilului.
Pe parcursul anului 2000, parteneriatul public-privat n protecia copilului, prin serviciile
dezvoltate la nivelul comunittilor locale care au permis o interventie timpurie n familia cu risc si
un sprijin acordat familiei n dificultate prin consiliere, ajutor material si financiar, servicii pentru
copil n centre de zi, centre mam-copil, au reusit s previn institutionalizarea sau abandonul
pentru un numr de 15.734 copii, n toat aceast perioad familiile acestora fiind monitorizate si
sprijinite pentru depsirea situatiei de criz. n anul 2000, serviciile publice pentru protectia
copilului au avut n evident si au protejat n parteneriat cu serviciile private pentru protectia
copilului un numr de 103.903 copii:
Tabel nr. 4: Distributia copiilor protejati n anul 2000 de ctre servicii publice si private
Numr copii protejati
temporar n institutii
rezidentiale publice
sau private
Numr copii protejati
temporar n familiile
rudelor, alte familii
din comunitate sau la
asistenti maternali
profesionisti
Numr copii mentinuti
n familia natural cu
suport
material/financiar,
servicii de consiliere,
centre de zi, centre
maternale
Total copii n
evidenta serviciilor
pentru protectia
copilului
57.597 30.572 15.734 103.903
Sursa: Agentia National pentru Protectia Drepturilor Copilului
Desi noul cadrul normativ a pus bazele crerii unui sistem care s-i permit fiecrui copil
dezvoltarea armonioas a personalittii sale ntr-o familie, sistemul de ocrotire rezidenial nu a
31
disprut nc, dei a fost mult schimbat. Institutiile rezidentiale clasice au fost transformate n
centre de plasament, n subordinea serviciilor publice pentru protectia copilului judetene sau ale
sectoarelor municipiului Bucuresti, urmnd a proteja pentru o perioad determinat de timp copilul
pentru care nu a fost posibil mentinerea n familia natural sau protectia ntr-o familie
substitutiv. Paralel, numeroase organizatii neguvernamentale si-au creat propriile centre de
plasament desfsurnd activitti de protectie a drepturilor copilului n parteneriat cu serviciile
publice pentru protectia drepturilor copilului. Desi studii de specialitate au demonstrat c sistemul
rezidential de protectie reprezint cea mai nepotrivit solutie pentru protectia copilului si cea mai
scump n acelasi timp, nu s-a luat nc o decizie ferm n sensul nchiderii tuturor institutiilor
rezidentiale si desfsurrii activittilor de protectie prin servicii alternative dezvoltate la nivel
comunitar.
De asemenea, cadrul institutional din domeniul protectiei drepturilor copilului este marcat n
aceast perioad de o autoritate public central responsabil cu elaborarea si coordonarea
implementrii politicii guvernamentale n domeniu si anume Autoritatea Naional pentru
Protecia Copilului i Adopie (ANPCA), nfiintat prin O.U.G. 12/2001 si aflat n subordinea
Secretariatului General al Guvernului. n vederea atingerii scopurilor pentru care a fost nfiintat,
A.N.P.C.A. si nsuseste si promoveaz prevederile tratatelor si conventiilor internationale
definitorii pentru domeniul propriu de activitate, pornind de la Declaratia Universal a Drepturilor
Omului, Conventia cu privire la drepturile copilului, ratificat prin Legea 18/1990, Conventia
asupra protectiei copiilor si cooperrii n materia adoptiei internationale adoptat la Haga.
Activitatea structurilor administratiei centrale este completat la nivel local de activitatea a
dou institutii constituite n directa subordonare a Consiliului judetean/consiliilor locale ale
sectoarelor Municipiului Bucuresti: comisia judeean pentru protecia copilului si serviciul public
descentralizat, n spet direcia judeean pentru protecia copilului, ambele nfiintate, asa cum am
mai artat anterior, prin O.U.G. nr.26/1997. n ianuarie 2003, Guvernul Romniei adopt o H.G.
nr.90 avnd drept obiectiv aprobarea Regulamentului cadru de organizare i funcionare a
serviciului public de asisten social. Potrivit prevederilor sale, n exercitarea atributiilor ce le
revin potrivit prevederilor Legii nr.705/2001 privind sistemul naional de asisten social,
consiliile judetene, respectiv Consiliul General al Municipiului Bucuresti, precum si consiliile
locale ale municipiilor, oraselor si sectoarelor municipiului Bucuresti, denumite consilii locale,
nfiinteaz si organizeaz serviciul public de asisten social. nfiintarea sa se va realiza, pn la
data de 31 martie 2003, prin reorganizarea serviciilor publice cu atributii n domeniu aflate n
subordine, sau dup caz a compartimentelor din aparatul propriu si prin redistribuirea personalului
32
existent n cadrul acestora, urmnd ca aceste dispozitii s nu fie aplicabile serviciilor publice
pentru protectia copilului organizate la nivel judetean (Art.4 alin. 1 si 2 din H.G. nr. 90/2003).
Serviciul public de asisten social de la nivelul judeelor, respectiv al municipiului
Bucuresti, are rolul de a sigura aplicarea la acest nivel a politicilor si strategiilor de asistent
social n domeniul protectiei familiei, persoanelor singure, persoanelor vrstnice, persoanelor cu
handicap, precum si a oricrei persoane aflate n nevoie. Serviciul public local are rolul de a
identifica si de a solutiona problemele sociale ale comunittii din domeniul protectiei copilului,
familiei, persoanelor singure, persoanelor vrstnice, persoanelor cu handicap, precum si a oricror
persoane aflate n nevoie. Deci, domeniile n care serviciul public local desfsoar activitti sunt:
domeniul protectiei copilului, domeniul protectiei persoanelor adulte, domeniul institutiilor de
asistent social publice sau private, domeniul finantrii asistentei sociale. Dintre atributiile
concrete ale acestei institutii n domeniul protectiei copilului mentionm (Art.3 lin.2 lit.A, din
Regulamentul-Cadru de organizare i funcionare a serviciului public de asisten social,
publicat n Monitorul Oficial nr.81/7.II.2003): monitorizarea si analiza situatiei copiilor din
unitatea administrativ-teritorial respectiv, respectarea si realizarea drepturilor lor; identificarea
copiilor aflati n dificultate, elaborarea documentatiei pentru stabilirea msurilor speciale de
protectie a acestora si sustinerea n fata organelor competente a msurilor de protectie propuse;
realizarea si sprijinirea activittii de prevenire a abandonului copilului; exercitarea dreptului de a
reprezenta copilul si de a-i administra bunurile; organizarea si sustinerea dezvoltrii de servicii
alternative de tip familial. Atributiile cuprind si: urmrirea si asigurarea aplicrii msurilor
educative stabilite de organele competente pentru copilul care a svrsit o fapt prevzut de legea
penal, dar nu rspunde penal; realizarea de parteneriate si colaborri cu organizatii
neguvernamentale si cu reprezentanti ai societtii civile n vederea dezvoltrii si sustinerii
msurilor de protectie a copilului; asigurarea accesului n institutiile de asistent social destinate
copilului sau mamei si copilului si evaluarea modului n care sunt respectate drepturile acestora.
n legtur direct cu protectia drepturilor copilului, pentru diminuarea srciei severe, s-a
introdus un suport institutional si financiar, Legea 416 din 2001 a venitului minim garantat, cu
modificrile si completrile ulterioare (Legea nr. 115 din 2006, de modificare si completare a
Legii nr. 416 din 2001, publicat n Monitorul Oficial, Partea I, nr. 401 din 2006).
n al doilea rnd, ca cerint a Uniunii Europene (Conferinta de la Nisa din decembrie 2000)
s-a luat decizia de constituire a Comisiei Naionale Anti-Srcie i Promovare a Incluziunii
Sociale.
Dezinstituionalizarea copiilor a reprezentat un proces continuu, initiat n perioada 1997-
1998, asa cum am mentionat anterior, si care a ctigat n amploare n perioada 2001 - 2005. Ca
prim rezultat concret, la nivel national numrul copiilor instituionalizai a sczut de la 53.335 n
33
anul 2000 la 27.039 n martie 2005. De asemenea, numrul instituiilor mari (cu un numr mai
mare de 100 copii protejati) a sczut de la 205 institutii la nceputul anului 2001, la 131 institutii la
sfrsitul anului 2002 si respectiv 51 n martie 2005. n acelasi timp, numrul copiilor protejai n
mediul familial a crescut de la 16.782 n anul 2001, la 21.414 n anul 2005. Acest din urm rezultat
a fost obtinut, n principal, prin sprijinirea rudelor pentru a-si asuma responsabilitatea cresterii si
educrii copiilor, dar si prin promovarea protectiei prin intermediul institutiei asistentul maternal
profesionist.
nchiderea instituiilor de tip vechi a reprezentat o mare provocare pentru sistemul de
protectie a copilului. S-a constatat c noua misiune acordat institutiilor pentru copii nu mai poate
fi ndeplinit n fostele locatii, indiferent de eforturile care s-au fcut (reparatii capitale,
restructurri, modulri etc.). Din acest motiv s-a luat decizia mutrii copiilor n locatii adecvate
care s rspund nevoilor lor individuale. La sfrsitului anului 2002, un numr de 93 institutii de
tip vechi erau nchise (27 foste internate ale scolilor speciale, 5 foste cmine spital, 4 institutii
transferate de la Ministerul Snttii si 57 centre de plasament). De asemenea numrul centrelor
de plasament funcionale a crescut de la 758 n anul 2001 la 1375 n anul 2005. Printre solutiile
adoptate n vederea rezolvrii acestor situatii amintim: reintegrarea copilului n familia natural,
protectia copiilor prin alternative de tip familial (asistentul maternal profesionist, rude, alte
familii/persoane), protectia copilului n csute de tip familial sau apartamente. Totodat, n functie
de nevoile copilului si ale familiei, acestia au beneficiat si de anumite servicii de suport (consiliere,
ngrijire de zi, servicii de recuperare pentru copilul cu handicap etc.).
n perioada 2001 - 2005, reeaua de asisten maternal s-a dezvoltat n mod semnificativ,
fiind nregistrat o crestere a numrului de asistenti maternali profesionisti de la 3.228 la 14.111.
La sfrsitul anului 2005, n structura Directiilor Generale de Asistent Social si Protectia
Copilului au fost dezvoltate un numr de 593 servicii alternative: 58 centre maternale, 118 centre
de zi, 50 servicii de asistent si sprijin pentru tinerii care provin din centrele de plasament, 70
centre de consiliere si sprijin pentru printi, 46 servicii de prevenire a abandonului n perioada
preconceptiv si servicii de monitorizare, asistent si sprijin al femeii gravide predispus la
abandonul copilului, 48 centre de pregtire si sprijinire a reintegrrii si integrrii copilului n
familie, 92 centre de ngrijire de zi si recuperare a copilului cu dizabilitti, 16 servicii de orientare,
supraveghere si sprijinire a reintegrrii sociale a copilului delincvent, 10 centre de asistent si
sprijin pentru readaptarea psihologic a copilului cu probleme psihosociale, 23 servicii pentru
sprijinirea copilului n exercitarea drepturilor sale, inclusiv a dreptului la exprimarea liber a
opiniei, 18 servicii pentru copiii strzii, 18 centre de consiliere si sprijin pentru copilul maltratat,
abuzat, neglijat, inclusiv victim a violentei n familie si 26 alte servicii.
34
Integrarea socio-profesional a tinerilor care prsesc sistemul de protecie a copilului
reprezint un alt domeniu cruia i se acord atenie. n aceast perioad s-a urmrit att crearea
unor servicii adecvate n cadrul Directiilor pentru Protectia Copilului care s se concentreze asupra
pregtirii pentru viat a adolescentilor si tinerilor, ct si crearea unui cadru legislativ si institutional
care s asigure suportul necesar tinerilor pentru gsirea unui loc de munc si a unei locuinte. Cu
toate acestea problemele nu au fost solutionate.
n vederea pregtirii adolescentilor si tinerilor pentru viat, n structura Directiilor pentru
Protectia Copilului au nceput s fie dezvoltate servicii specifice. Marea majoritate a acestora o
reprezint apartamentele n care tinerii se autogospodresc cu un nivel minim de supraveghere din
partea adultilor (personalului angajat). La nivel national, exist un numr de 50 de astfel de
servicii, dezvoltate fie prin programul de interes national nr. 4 din anul 2002, fie prin Programul de
reform finantat de BIRD si BDCE si prin Programul Phare 1999 Copiii mai nti. n anul 2001,
a fost realizat primul plan de actiune pentru reintegrarea social a copiilor strzii si totodat a fost
momentul constientizrii faptului c acest domeniu necesit timp si resurse financiare, materiale si
umane importante. Implementarea msurilor propuse n perioada 2001- 2002 a avut drept rezultat
reducerea semnificativ a dimensiunilor fenomenului. Astfel, la sfrsitul anului 2002, numrul de
copii si tineri adulti care triau n strad a sczut de la 2500 la 1500 la nivel national si de la 700 la
aproximativ 400 n Bucuresti.
Prin Ordonanta de Urgent nr. 121/10.2001, aprobat prin Legea nr.347/2002, au fost
suspendate pe o perioada de 12 luni de la data intrrii n vigoare a acesteia, toate procedurile
avnd ca obiect adopia copiilor romni de ctre o persoan sau o familie cu cetenie strin ori
de ctre o persoan sau o familie cu cetenie romn i cu domiciliul sau cu reedina pe
teritoriul altui stat. Termenul prevzut de art. (1) din OUG nr. 121/2001 a fost prorogat, astfel
nct suspendarea este valabil pn la data de 1 Martie 2003. Aceast decizie a fost luat urmare
numeroaselor critici adresate Guvernului Romniei, din partea organizatiilor si institutiilor
internationale. Dup luarea deciziei de suspendare, la 20 noiembrie 2001, prin Decizia Primului
Ministru nr. 401, s-a constituit Grupul Independent de Analiz a Sistemului de Adoptii
Internationale (GIASAI), format din 3 experti independenti. Potrivit responsabilittilor stabilite
prin Decizia Primului Ministru, acest grup a naintat la data de 26 martie 2002 raportul de evaluare
cu privire la reorganizarea sistemului de adoptii internationale si de protectie a copilului n
dificultate.
Grupul de lucru legislativ, constituit n baza prevederilor Strategiei privind implementarea
msurilor cuprinse n raportul ntocmit de GIASAI, a elaborat un prim proiect de lege privind
regimul juridic al adopiei. Principalele elemente de noutate aduse prin acest proiect vizeaz:
35
promovarea cu prioritate a adoptiei nationale si abordarea adoptiei internationale ca msur
de protectie a unui copil n dificultate doar ca solutie ultim;
eliminarea organismelor private din procedura adoptiei si ntrirea rolului si
responsabilittilor sectorului public n acest proces;
realizarea ncetrii drepturilor printesti numai prin procedur judectoreasc (nu si prin
procedur administrativ, cum prevedea legislatia precedent);
sublinierea si ntrirea, prin noile proceduri, a rolului printilor n ngrijirea propriilor copii,
precum si a obligativittii responsabililor din domeniu de a face toate demersurile pentru
mentinerea copilului n cadrul familiei naturale/lrgite (doar dup parcurgerea obligatorie a acestei
etape, adoptia poate fi luat n considerare).
In 2005, moratoriul a fost nlocuit de actuala lege, Legea 273 din 2004 privind regimul
juridic al adopiei, care permite adoptia international a copiilor romni numai de ctre rude, cel
mult de gradul al doilea.
Dar, pentru conturarea ct mai cuprinztoare a cadrului legislativ privind protectia
drepturilor copilului, legiuitorul romn adopt n aceeasi perioad acte normative importante
precum: Legea 272 din 2004 privind protecia i promovarea drepturilor copilului, Hotrrea
Guvernului nr. 1434 din 2004 privind atribuiile i Regulamentul cadru de organizare i
funcionare a Direciei generale de asisten social i protecia copilului, Hotrrea Guvernului
nr. 1437 din 2004 privind organizarea si metodologia de functionare a comisiei pentru protecia
copilului, Hotrrea Guvernului nr. 1438 din 2004 pentru aprobarea regulamentelor cadru de
organizare si functionare a serviciilor de prevenire a separrii copilului de familia sa, precum si a
celor de protecie special a copilului lipsit temporar sau definitiv de ocrotirea prinilor si,
Hotrrea Guvernului nr. 1439 din 2004 privind serviciile specializate destinate copilului care a
svrit o fapt penal i nu rspunde penal, Hotrrea Guvernului nr. 1440 din 2004 privind
conditiile si procedura de licentiere si inspectie a serviciilor de prevenire a separrii copilului de
familia sa, precum si a celor de protecie special a copilului lipsit temporar sau definitiv de
ocrotirea prinilor si; Ordonana de urgen a Guvernului nr. 12 din 2001 privind nfiintarea
Autoritii Naionale pentru Protecia Drepturilor Copilului.
De asemenea, n temeiul art. 105 din Legea nr. 272/2004 si a prevederilor H.G. nr. 1434/
2004 ia fiint la nivelul fiecrui judet Direcia General de Asisten Social i Protecia
Copilului. Ea reprezint o institutie public cu personalitate juridic, care functioneaz n
subordinea Consiliului Judetean prin comasarea Serviciului Public de Asistent Social si a
Serviciului Public Specializat pentru Protectia Copilului de la nivel judetean si preia n mod
corespunztor atributiile si functiile celor dou institutii, precum si ntreg personalul acestora,
personal care se consider transferat, n conditiile legii. Directia General de Asistent Social si
36
Protectia Copilului realizeaz, la nivel judetean, msurile de asistent social n domeniul
protectiei copilului, familiei, persoanelor singure, persoanelor vrstnice, persoanelor cu handicap,
precum si a oricror persoane aflate n nevoie. n vederea realizrii atributiilor prevzute de lege
Directia general ndeplineste n principal urmtoarele functii: de strategie, n temeiul creia
asigur elaborarea strategiei de asistent social, a planului de asistent social pentru prevenirea si
combaterea marginalizrii sociale, precum si a programelor de actiune antisrcie; de coordonare a
activittilor de asistent social si protectie a copilului de la nivel judetean; de administrare a
fondurilor pe care le are la dispozitie; de colaborare cu serviciile publice deconcentrate ale
ministerelor si institutiilor care au responsabilitti n domeniul asistentei sociale, cu serviciile
publice locale de asistent social, precum si cu reprezentantii societtii civile care desfsoar
activitti n domeniu; de execuie, prin asigurarea mijloacelor umane, materiale si financiare
necesare pentru implementarea strategiilor cu privire la actiunile antisrcie, prevenire si
combatere a marginalizrii sociale, precum si pentru solutionarea urgentelor sociale individuale si
colective la nivelul judetului, respectiv al sectoarelor municipiului Bucuresti; de reprezentare a
consiliului judetean, respectiv a consiliului local al sectorului municipiului Bucuresti, pe plan
intern si extern, n domeniul asistentei sociale si protectiei copilului.
Prin Legea nr. 275 din 2004, Autoritatea National pentru Protectia Copilului si Adoptie este
nlocuit de Autoritatea Naional pentru Protecia Drepturilor Copilului, ca organ de specialitate
al administratiei publice centrale cu personalitate juridic, n subordinea Ministerului Muncii,
Solidarittii Sociale si Familiei. Atributiile din domeniul protectiei copilului prin adoptie vor fi
preluate de Oficiul Romn pentru adopii.
Pe parcursul anului 2005 a fost elaborat, de asemenea, cu consultarea tuturor factorilor
responsabili, Strategia naional n domeniul proteciei i promovrii drepturilor copilului pentru
perioada 2006-2013 si Planul Operational pentru perioada 2006-2008. Strategia va asigura
mobilizarea resurselor necesare, responsabilizarea factorilor relevanti si asigurarea unui parteneriat
eficient n vederea protectiei si respectrii drepturilor copilului, precum si a mbunttirii conditiei
copilului si valorizrii sale n societatea romneasc.
Strategia are n vedere cei aproximativ 4,5 milioane copii ai Romniei si se refer la
implementarea drepturilor acestora, asa cum sunt ele definite n Conventia ONU si n alte
documente internationale ratificate de Romnia, n toate domeniile de interes pentru copii: social,
familial, educational, de sntate etc. Totodat sunt vizati si copiii cetteni romni aflati n
strintate, precum si copiii fr cettenie aflati pe teritoriul Romniei, copiii refugiati si copiii
cetteni strini aflati pe teritoriul Romniei, n situatii de urgent. Totodat, Strategia si propune
s acopere un domeniu pentru care Romnia s-a angajat n urm cu 15 ani, dar nu s-a realizat
complet pn n prezent, monitorizarea respectrii drepturilor copiilor si msuri concrete
37
legislative si administrative n vederea promovrii si respectrii lor att de ctre familie, persoane
fizice, ct si de institutii si autoritti.
De asemenea, potrivit prevederilor HG nr. 1217 din 6 septembrie 2006 Comisia anti
srcie si promovare a incluziunii sociale CASPIS si-a ncetat activitatea. Potrivit aceluiasi act
normativ a fost nfiintat Comisia naional privind incluziunea social iar coordonarea
activittilor din domeniul incluziunii sociale revine Ministerului Muncii, Solidarittii Sociale si
Familiei.
Tendinta politicilor n domeniul protectiei si promovrii drepturilor copilului se axeaz din
acest moment pe descentralizare si responsabilizarea comunittii locale. n acest sens comunitatea
local este considerat a fi n msur s identifice si s previn situatiile de risc, precum si s
identifice resursele si solutiile primare de interventie.
Legea nr.272/2004 privind protecia i promovarea drepturilor copilului defineste clar
obligatia autorittilor administratiei publice locale de a garanta si promova respectarea drepturilor
copiilor din unittile administrativ-teritoriale, asigurnd prevenirea separrii copilului de printii
si, precum si protectia special a copilului lipsit temporar sau definitiv de ngrijirea printilor si.
n capitolul VII, art.103 este specificat faptul c Autorittile administratiei publice locale au
obligatia de a implica colectivitatea local n procesul de identificare a nevoilor comunittii si de
solutionare la nivel local a problemelor sociale care privesc copiii. n acest scop pot fi create
structuri comunitare consultative cuprinznd, dar fr a se limita, oameni de afaceri locali, preoti,
cadre didactice, medici, consilieri locali si politisti. Rolul acestor structuri este att de solutionare a
unor cazuri concrete, ct si de a rspunde nevoilor globale ale respectivei colectivitti.
Pe baza experientelor din anii trecuti si tinnd cont de practicile trilor dezvoltate, Romnia a
adoptat si a nceput s aplice din anul 2005 o legislatie care face trecerea de la un sistem axat pe
protectia copilului n dificultate la un sistem care vizeaz promovarea si respectarea drepturilor
tuturor copiilor.
n ceea ce priveste serviciile sociale, specialistii consider c acestea nu s-au dezvoltat
unitar, n perioada posterioar anului 1989, pentru toate sectoarele asistentei sociale. Cel mai mult
s-a realizat ns n domeniul protectiei copilului, sector n care s-a beneficiat att de sustinere
guvernamental major ct si de un interes deosebit din partea specialistilor. Legiuitorul romn a
adoptat Ordonana nr. 68 din 28 august 2003 privind serviciile sociale, act normativ care pune
bazele juridice ale acestei institutii. n acceptiunea dispozitiilor legale, serviciile sociale reprezint
ansamblul complex de msuri si actiuni realizate pentru a rspunde nevoilor sociale individuale,
familiale sau de grup, n vederea depsirii unor situatii de dificultate, pentru prezervarea
autonomiei si protectiei persoanei, pentru prevenirea marginalizrii si excluziunii sociale si
38
promovarea incluziunii sociale. Serviciile sociale sunt asigurate de ctre autorittile administratiei
publice locale, precum si de persoane fizice sau juridice publice sau private.
Au fost elaborate de asemenea, n concordant cu dispozitiile legale, standarde de calitate
pentru serviciile sociale din domeniul protectiei copilului cu ar fi de exemplu: Standardele minime
obligatorii pentru protectia copilului de tip rezidential, Standarde minime pentru centrul maternal,
Standarde minime obligatorii privind centrul de consiliere si sprijin pentru printi si copii,
Standarde minime obligatorii pentru asigurarea protectiei copilului la asistent maternal
profesionist, Standarde minime obligatorii din 19 mai 2004 privind centrul de pregtire si sprijinire
a reintegrrii si integrrii copilului n familie, Standarde minime obligatorii privind procedura
adoptiei interne, Standarde minime obligatorii pentru centrele de zi, Standarde minime obligatorii
privind centrele de zi pentru copiii cu dizabilitti.
n contextul elaborrii si aplicrii Legii cadru a sistemului de asisten social, programul de
guvernare 2004-2008 aduce n discutie redefinirea rolului statului n procesul de reconstructie
institutional a sistemului de servicii de asistent social si transferul partial al responsabilittii
furnizrii serviciilor ctre sectorul nonguvernamental. Astfel, Autoritatea National pentru
Protectia Drepturilor Copilului si-a propus ca pn la finalul acestuia s concesioneze
organizatiilor nonguvernamentale 40-45% din actualele servicii publice pentru protectia copilului
si a familiei. Transferul de servicii va facilita, conform ANPDC construirea unui sistem de
servicii, la nivel national, care s ajung pn la usa clientului. Principalii parteneri implicati n
ndeplinirea acestui scop vor fi autorittile locale si organizatiile nonguvernamentale.
Pornind de la aceast strategie de restructurare a sistemului de servicii de asistent social,
literatura de specialitate, a crei opinie o mprtsim, sustine ideea c directiile propuse sunt mai
degrab elementele unui experiment riscant att pentru sectorul guvernamental ct si pentru cel
public (Zamfir, C., Stoica, L., 2006, pp. 217-222).
Sunt reliefate punctele vulnerabile ale sectorului nonguvernamental precum: disparittile
regionale si pe medii ale distributiei ONG-urilor active (doar 15-17% din organizatiile active
furnizeaz servicii sau au activitti n mediul rural iar n zona de sud-est a Romniei numrul de
ONG-uri active este extrem de redus n comparatie cu celelalte zone), dependenta acestora de
finantrile externe (procentul proiectelor derulate doar pe cont propriu se ridic doar la 6%),
suportul redus de la bugetul de stat sau local ( n anul 2004 au fost sprijinite 69 de ONG-uri cu
aproape 1.000.000 de euro, valoare ce a acoperit doar 10% din bugetul anual al acestora),
conditiile restrictive de acces la finantri (aprobarea unei finantri este conditionat de asigurarea
unor contributii proprii n bani cuprinse ntre 10-20%, dificil de acoperit n conditiile unei
dependente de finantarea extern), nivel de profesionalizare redus si mobilitate ridicat a resursei
umane, capacitate redus de absorbtie a ONG-urilor pe termen scurt, cadrul legislativ inadecvat si
39
promovarea insuficient a actelor normative elaborate (n special faptul c legislatia din asistent
social nu a beneficiat de armonizri cu celelalte acte normative care pot sprijini efortul de
reconstructie institutional), sistem nefunctional de acreditare/ evaluare/monitorizare a furnizorilor
de servicii.
Pentru realizarea reformei institutionale n domeniul asistentei sociale si al politicilor
familiale, specialistii propun nfiintarea Colegiului pentru Coordonarea Politicilor de Asisten
Social, la nivelul Ministerului Muncii, Solidarittii Sociale si Familiei, care va avea menirea de a
asigura caracterul unitar al politicii generale n domeniul asistentei sociale, ct si n ceea ce
priveste politicile sectoriale (Gheorghe Barbu, Ministrul Muncii, Solidarittii Sociale si Familiei,
intervievat de Valentina Rujdu n lucrarea Direcii ale reformei sistemului de asisten social n
Romnia, aprut n Revista de Asisten Social, Nr. , 2005, p. 3-5).
Adoptarea la 8 martie 2006 a Legii nr. 47 privind sistemul naional de asisten social a
determinat abrogarea explicit a vechiului act normativ ce reglementa acest domeniul si anume
Legea 705 din 2001. Noul act normativ pune bazele juridice ale unor noi institutii. Se creeaz
astfel Observatorul Social, institutie public cu personalitate juridic, ce functioneaz ca organ de
specialitate n directa coordonare a Ministerului Muncii, Solidarittii Sociale si Familiei avnd ca
scop eficientizarea procesului de elaborare si implementare a politicilor sociale la nivel nationale.
De asemenea, Inspecia Social este organul de specialitate al administratiei publice centrale, cu
personalitate juridic, aflat tot n subordonarea Ministerului Muncii, Solidarittii Sociale si
Familiei si care are ca scop implementarea legislatiei n domeniu, precum si inspectarea activittii
institutiilor publice si private, responsabile cu furnizarea prestatiilor si serviciilor sociale. S-a
nfiintat si Agenia Naional pentru Prestaii Sociale, ca organ de specialitate cu personalitate
juridic, n subordinea aceluiasi minister, cu scopul crerii unui sistem unitar privind administrarea
procesului de acordare a prestatiilor sociale. Institutia nou creat si va desfsura activitatea prin
structuri organizate n fiecare municipiu, resedint de judet, precum si n municipiul Bucuresti.
Pentru asigurarea politicilor sociale n domeniul protectiei copilului si familiei, Legea
permite autorittilor administratiei publice locale nfiintarea si organizarea de servicii publice de
asisten social.
Putem concluziona c regimurile socialiste au promovat o politic de preferint pentru
institutionalizarea copiilor cu probleme si nu suportul familiilor acestora. Pentru perioada de dup
1989, caracteristic este dezinstitutionalizarea. n Romnia au avut loc importante progrese n
politicile de protectie a copilului abondonat, cresterea spijinului statului si a fondurilor alocate
acestui scop, ns fr a putea nu putem afirma rezolvarea problemei copiilor aflati n dificultate.
40
Summary
Protection of Child in Difficulty in Romania
This paper proposes a brief presentation of the child protection politics in the communist regime
and the development and progress of child welfare system after 1989 in Romania.
Key words: child protection politics, child welfare system, Romania
Bibliografie
Alexiu, M.,T., Clive, S., Asistena social n Marea Britanie i Romnia, UNICEF, Bucuresti,
2000;
Comnescu, I., Mihut, I., Petrescu, R., Ocrotirea familiei n dreptul socialist romn, Editura
Politic, Bucuresti, 1989;
Mihilescu, I., (coord.), Povara unui deceniu de tranziie. Situaia copilului i a familiei n
Romnia, UNICEF, Bucuresti, 2000;
Revista de Asisten Social, Nr. , Editura Polirom, Iasi, 2005: Gheorghe Barbu, Ministrul
Muncii, Solidarittii Sociale si Familiei, intervievat de Valentina Rujdu n lucrarea Direcii ale
reformei sistemului de asisten social n Romnia;
Roth-Szamoskzi, M., Protecia copilului. Dileme, concepii i metode, Editura Presa
Universitar Clujan, Cluj-Napoca, 1999;
Zamfir C., Zamfir, E., Politici sociale n Romnia n context european, Editura Alternative,
Bucuresti, 1995;
Zamfir, C. (coord.), Pentru o societate centrat pe copil, Editura Alternative, Bucuresti, 1997;
Zamfir, C., Stoica, L. (coord.), O nou provocare: dezvoltarea social, Editura Polirom, Iasi,
2006;
Acte normative interne i internaionale:
Convenia cu privire la Drepturile Copilului, adoptat de Adunarea General ONU la 20
noiembrie 1989, intrat n vigoare la 2 septembrie 1990 si ratificat de Romnia prin Legea
nr.18/1990 publicat n Monitorul Oficial nr.109 din 28 septembrie 1990;
H.G. nr.90/23 ianuarie 2003, publicat n Monitorul Oficial, Partea I, nr.81/7.02.2003;
H.G. nr. 679 din 12 iunie 2003 privind condiiile de obinere a atestatului, procedurile de
atestare i statutul asistentului maternal profesionist, publicat n Monitorul Oficial, nr.443 din 23
iunie 2003;
HG nr. 1217 din 6 septembrie 2006 a fost publicat n Monitorul Oficial nr. 808/26.IX 2006;
Legea nr.11 din 1990 privind ncuviinarea adopiei republicat n Monitorul Oficial nr.159 din
26 iulie 1991;
Legea nr. 47 din 1993 cu privire la declararea judectoreasc a abandonului de copii, publicat
n Monitorul Oficial al Romniei, Partea I, nr. 153 din 8.07.1993;
41
Legea nr.61 din 1993 privind alocaia de stat pentru copii republicat, publicat n Monitorul
Oficial nr.56/08.02.1999;
Legea 273/2004 privind regimul juridic al adopiei, publicat n Monitorul Oficial. nr. 557 din
23.06. 2004. Dispozitiile acestei legi, cu exceptia celor care permit crearea cadrului necesar
aplicrii sale, au intrat n vigoare la 1 ianuarie 2005;
Legea nr. 272 din 2004 privind protecia i promovarea drepturilor, publicat n Monitorul
Oficial, nr.557 din 23.06.2004;
Legea nr. 275 din 2004, pentru modificarea O.U.G. nr. 12 din 2001, privind nfiintarea
Autorittii Nationale pentru Protectia Copilului si Adoptie, publicat n Monitorul Oficial, nr. 557
din 23 iunie 2004;
Legea nr. 115 din 2006, de modificare si completare a Legii nr. 416 din 2001, publicat n
Monitorul Oficial, Partea I, nr. 401 din 2006;
Legea nr. 47 din 2006 privind sistemul naional de asisten social, publicat n Monitorul
Oficial nr. 239 din 16 martie 2006;
O.U.G nr.26 din 1997 privind protecia copilului n dificultate publicat n Monitorul Oficial
nr.120 din 1997, aprobat prin Legea nr. 108/1997 publicat n Monitorul Oficial nr. 205 din 1998;
O.U.G nr. 25 din 1997 privind regimul juridic al adopiei, publicat n Monitorul Oficial, nr.
120 din 12 iunie 1997;
Ordonana nr. 68 din 28 august 2003 privind serviciile sociale, publicat n Monitorul Oficial
nr. 619 din 30 august 2003;
Regulamentul-Cadru de organizare i funcionare a serviciului public de asisten social,
publicat n Monitorul Oficial nr.81/7.II.2003;
Strategia Naional de dezvoltare a sistemului de protecie a copilului a fost adoptat de
Guvernul Romniei n iulie 2000 prin HG nr.625/2000 ;
Standarde minime obligatorii din 26 februarie 2004 privind serviciile pentru protectia copilului
de tip rezidential, publicate n Monitorul Oficial, nr. 222 din 15 martie 2004;
Standarde minime din 16 iulie 2004 privind centrul maternal, publicate n Monitorul Oficial nr.
736 din 16 august 2004;
Standarde minime obligatorii privind centrul de consiliere si sprijin pentru printi si copii,
publicate n Monitorul Oficial nr. 726 din 12 august 2004;
Standarde minime obligatorii din 15 mai 2003 pentru asigurarea protectiei copilului la asistent
maternal profesionist, publicate n Monitorul Oficial nr.359 din 27 mai 2003;
Standarde minime obligatorii din 19 mai 2004 privind centrul de pregtire si sprijinire a
reintegrrii si integrrii copilului n familie, publicate n Monitorul Oficial nr. 497 din 2 iunie
2004;
Standarde minime obligatorii din 25 martie 2004 privind procedura adoptiei interne, publicate n
Monitorul Oficial nr. 306 din 7 aprilie 2004;
Standarde minime obligatorii din 4 martie 2004 pentru centrele de zi, publicate n Monitorul
Oficial nr. 247 din 22 martie 2004;
Standarde minime obligatorii din 9 martie 2004 privind centrele de zi pentru copiii cu
dizabilitti, publicate n Monitorul Oficial nr. 247 din 22 martie 2004.
Primit 12.11.2008
42
Altruismul
Butariu Alina Elena, Romnia
Una dintre cele mai frecvente imagini ale societtii contemporane, este aceea n care un om,
un semen de-al nostru are nevoie de ajutor. In lupta cu viata si uneori cu cei din jurul su, el omul de
lng noi, asteapt o mn ntins sau poate doar un cuvnt ncurajator pentru a putea depsi criza
n care se afl si a nu distruge tot ce a acumulat pn n acel moment.
Chiar daca cei mai multi oameni sunt aceia care consider c problema nu este a lor si prin
urmare nu au de ce s se implice, exist si persoane, destul de putine de altfel, care actioneaz si n
favoarea celorlalti sunt generosi, prietenosi, animati de dragoste dezinteresat fat de semeni,
punndu-si toate mijloacele la dispozitia celorlalti fr a viza vreun scop anume: altruitii.
Persoanele altruiste i consider pe cei din jurul lor scopuri, n sine si nu mijloace n vederea
realizrilor proprii, fiind narmati cu o moralitate desvrsit. Ajutorul acordat implic mult timp,
efort si sacrificii, ca si decizia de a ne asuma responsabilitatea (este mult mai simplu s asisti
indiferent dect s participi la rezolvarea conflictului).
Atta timp ct exist persoane, gata oricnd s se sacrifice pentru binele aproapelui, merit
s fie atras atentia asupra lor, astfel nct ceilalti s le urmeze exemplul si s-si perfectioneze
conduita.
Actiunile unor asemenea persoane ne fac s ne punem ntrebarea: "de ce doar unii dintre
noi prefer s se implice si ce anume i determin s o fac?" Se nasc asa sau se formeaz pe
parcursul vietii? Apare astfel ideea studierii unor aspecte ale comportamentului altruist la vrsta
prescolar. Chiar dac oamenii au primit ndemnul spre a face bine celorlalti, din cele mai vechi
timpuri "(Iubeste pe aproapele tu ca pe tine nsuti"- Matei, cap. 22, 23), nu toti se conformeaz si
nu actioneaz ca atare. De aceea este foarte important ca sentimentul dragostei pentru cellalt, al
ajutorului neconditionat s fie transmis de timpuriu, de la vrste ct mai fragede.
Multi cercettori consider c de fapt, altruism pur nici nu exist; c nimeni nu poate
ajunge s-si riste viata dac nu ar fi ndemnat de anumite motive.
Daniel Baston si colaboratorii si (1987), sunt de prere c exist multe ntrebri fr
rspuns n analiza altruismului. Ei argumenteaz c actele de ntrajutorare, unele, sunt altruiste.
Teoria lui porneste de la ncredere, considerat factorul principal n promovarea comportamentului
pozitiv; la rndul su, ncrederea, implic o experient emotional. Cnd oamenii au ncredere, se
simpatizeaz, sunt dispusi s ajute mai usor (Eisenberg si Miller, 1987). Dar ajutm doar pentru
reducerea disconfortului propriu sau al altora? Care este diferenta dintre motivele egoiste si cele
altruiste? Baston rspunde la asemenea ntrebri, specificnd ce se ntmpl cu noi, ce simtim cnd
43
vedem pe cineva aflat n dificultate? Dup teoria sa, experimentm propria suferint si preocupare
(ce include si compasiunea, tandretea, simpatia).
Motivele care stau la baza comportamentelor prosociale sunt multiple, dar nu se poate face
abstractie de cei care ntr-adevr actioneaz doar pentru binele celorlalti. Existenta acestor
persoane ne ndeamn s credem c lumea nu este alctuit numai din haos, c binele, adevrul si
dreptatea nc mai pot nvinge.
Definirea comportamentului prosocial. Altruismul
nainte de a prezenta definitiile date de diversi sociologi, psihologi, chiar filozofi, se impun
cteva precizri:
- trebuie fcut distinctia ntre ajutorul interesat bazat pe schimbul echitabil de bunuri
si servicii dintre persoane si conduita prosocial n care, beneficiile ofertantului de ajutor nu sunt
directe si previzibile. Varianta maxim a dezinteresului o reprezint altruismul adevrat, cnd sunt
vizate doar satisfactii spirituale pure si nu este cutat aprobarea celorlalti oameni. Exemplul
extrem, de altruism pur este ntlnit n Biblie, n Evanghelia dup Luca, 10, 25-37 - pilda Bunului
Samaritean -, situatiile reale fiind destul de rare.
- De asemenea, mentionm n acord cu S. Chelcea c "nu orice comportament cu
consecinte pozitive n plan axiologic poate fi caracterizat ca prosocial". El trebuie s fie intentionat,
realizat n mod constient, prezenta intentiei de sprijinire a valori sociale fiind asadar obligatorie.
Exemplu: dac o persoan se afl ntmpltor n fata unui magazin si prin aceasta mpiedic
un rufctor s sustrag de aici bunuri sau bani, nu nseamn c a realizat un comportament
prosocial, desi consecinta este pozitiv. Am putea vorbi despre un asemenea comportament dac
acea persoan si-ar fi propus (intentionat) s mpiedice prim prezenta sa comiterea infractiunii. In
plus, acea persoan ar fi trebuit s nu fie n exercitiul functiunii, si s nu urmreasc vre-o
satisfactie (felicitri, premii, medalii, etc.).
In anumite situatii, comportamentele sunt usor de identificat ca fiind prosociale. Altele
necesit analize subtile, iar includerea lor n aceast categorie rmne discutabil, de multe ori
discernmntul personal, fiind cel care poate s califice un comportament.
Dictionarul de psihologie social (Chelcea et. al. 1981) defineste comportamentul prosocial
ca fiind "comportamentul caracterizat prin orientare spre valorile sociale". Sociologul polonez
Janusz Rujkowski, unul dintre fondatorii noii orientri de studiu, adic cea din perspectiva teoriei
actiunilor, sustine c comportamentul prosocial se defineste prin aceea c este orientat spre
ajutorarea, protejarea, sprijinirea, dezvoltarea celorlalte persoane, fr a astepta recompense
externe. Alti autori consider c acest tip de comportament poate fi definit ca "actiunea ce nu aduce
beneficii dect celui ce primeste ajutor".
44
A. Baum, J. D. Fischer, J. E. Singer (1985) nteleg prin comportamente prosociale, acele
"acte intentionate care ar putea avea consecinte pozitive pentru altii" fr a se anticipa vre-o
rsplat.
Hans Werner Bierhoff (1987) mentioneaz cele 2 conditii necesare si suficiente, dup
opinia sa, pentru identificarea comportamentelor prosociale:
- intentia de a ajuta alte persoane;
- libertatea alegerii - de a acorda ajutorul n afara obligatiilor profesionale.
Acelasi autor face trimiteri la D. Bar-Tal, Sharabany si Ravin (1982) care adaug a 3-a
restrictie: n afara intentionalittii si a absentei obligatiilor de serviciu,
c) comportamentul prosocial s fie realizat fr a astepta recompense externe.
Toate aceste definitii indic notele esentiale ale conceptului, ns i confer un nteles prea
ngust reducndu-1 la sfera altruismului. Dup S. Chelcea altruismul nu constituie dect o subspecie
a comportamentului prosocial care trebuie nteles ca fiind acel comportament intentionat, realizat
n afara obligatiilor profesionale si orientat spre sustinerea, conservarea si promovarea valorilor
sociale.
Termenul de comportament prosocial dobndeste o mai mare extensie, cuprinznd
fenomene variate ca: ajutarea semenilor, aprarea propriettilor, jertfa de sine pentru dreptate,
independenta patriei. Ajutorarea, sprijinirea dezvoltrii celorlalti ocup o pozitie central n
sistemul comportamentelor prosociale, omul avnd valoarea social suprem.
Marele filozof francez A. Compte, ntemeietorul pozitivismului si creatorul termenului
"sociologie", este cel care a creat si termenul de "altruism" pentru a desemna grija dezinteresat
pentru binele semenului.
Acest tip de comportament nu aduce dup sine beneficii de ordin financiar, mpcarea cu
sine, faptul de a fi svrsit ceva bun sunt singurele, dar adevratele recompense.
Desigur granita dintre ajutorul interesat si ajutorul dezinteresat este adesea foarte greu de
stabilit, dar, cnd beneficiile celui care ajut nu sunt directe si previzibile, actiunile sunt n favoarea
celorlalti, iar comportamentul prosocial.
In cadrul acestora, altruismul adevrat ar fi varianta maxim a dezinteresului, deoarece aici
n afara recompensei de dup moarte sau a satisfactiei pure, lipsit de orice alt compensatie, alte
beneficii nu exist.
Chiar dac actele de altruism pur sunt probabil foarte putine, ele exist si trebuie insistat
asupra lor.
45
Teorii care explic altruismul
Deoarece, sfera comportamentului prosocial este foarte larg, dup cum se poate vedea si
din definitiile prezentate anterior, ne vom limita la studierea aprofundat a unuia dintre aspectele
sale, si anume altruismul.
Faptul c omul este o "fiint social", c convietuieste alturi de ceilalti de la nastere pn
la moarte, l face, indiscutabil, s se raporteze la cei din jur, ajutorul pe care acestia si-1 ofer fiind
de natura evidentei.
Perspectiva sociobiologic
Una dintre explicatii vine paradoxal din partea biologiei, deoarece suntem tentati s credem
c altruismul contravine legii biologice supreme - a supravietuirii individului si a speciei. Indivizii
biologici, ce se sacrific, nu ar trebui selectati natural, probabilitatea de a lsa urmasi fiind mic.
Introducnd ns ipoteza "Supravietuirii prin nrudire" (Wilson 1975), comportamentul altruist
capt noi ntelesuri: membrii unei familii au gene comune si ajutndu-i pe altii, nruditi, asigur
transmiterea mai departe a propriilor gene (exemplu: albina moare prin ntepare). Fiecare individ e
motivat nu numai s triasc mai mult pentru a ajunge capitalul su genetic la urmasi ci si s
contribuie la crearea unui avantaj reproductiv celor cu gene comune.
Sociobiologia sustine deci c exist o baz genetic a altruismului; ajutndu-i pe cei
apropiati genetic, indivizii se "ajut" pn la urm pe ei. Explicatiile sociologilor sunt legate de
fenomenul similarittii, care, pe lng aspectele de ordin psihologic si axiologic, presupune si
asemnri genetice.
Problema ntrajutorrii n cazul rudelor pare astfel explicat, dar exist situatii, n care
ajutorul este dat unor necunoscuti, care trebuie explicat. Astfel apropierea poate fi cultural,
atitudinal, comportamental, etc. si noi facem "mai mult sau mai putin transparent, logic, diferenta
c acestia sunt apropiati genetic", iar analistii comportamentului uman ncearc s-1 explice.
Ruston (1989) plecnd de la constatarea c statistic, atractivitatea, iubirea, cstoria si
actele de ajutorare se ntemeiaz ntr-o mare msur pe similaritate, chiar de trsturi exterioare,
presupune si o asemnare genetic. Studiind gemenii - el sugereaz c si atitudinile ar fi n parte
determinate genetic, artnd c alti factori fac ca ntre "similarittile de ordin psihic, axiologic si
cele genetice, s existe o corelatie, si anume, proximitatea spatial si selectivitatea rezultat din
prejudecti" I. Radu (1994) (n spet rasiale si etnice).
Dup prerea unora, aceast pozitie sociobiologist e putin convingtoare, mai ales n
explicatia comportamentului altruist dat altor persoane (strine).
Critica este c: omul, fiint rational, plaseaz conduitele lui sociale sub semnul calculului, al
raportului cost - beneficii, asupra cruia voi reveni mai amnuntit n alt sub-capitol.
46
Ideea esential a acestui tip de interpretare este aceea c altruismul, sacrificiul, este mai
pronuntat cu ct suntem mai apropiati genetic de semenii nostri.
Perspectiva psihosociologic
O serie de studii experimentale confirm faptul c la fel ca si multe alte tipuri de
comportamente, cel prosocial, altruist, este nvtat n timpul socializrii primare.
Invtarea social prin mecanismul direct al recompensei si pedepsei, pe lng cel al
ntririi, ct si prin observarea direct a consecintelor comportamentelor altor persoane ce
ntreprind actiuni prosociale (nvtarea direct prin modele), conduce la nsusirea conduitei
altruiste la copiii.
Evolutia societtii determin un mecanism al selectiei sociale prin care se retin elementele
socioculturale cu valoare adaptativ (exemplu: comportamentele prosociale, n cazul de fat,
altruismul) si reproductiv, afirm D. Campebel (1975) n replic la perspectiva sociobiologic.
Comportamentele prosociale n general, si altruismul n particular, aduc beneficii grupurilor
sociale si sunt drept urmare promovate si ntrite de societate. In acest sens, exist 3 norme sociale
care regleaz aceast selectie.
a) Norma responsabilitii sociale
Conform acestei norme ne simtim obligati s oferim / acordm ajutor nu pentru a fi
recompensati ci pentru a ne simti satisfcuti cnd atingem standarde morale interne (L. Berkovitz
1962). Cnd, din diferite cauze nu satisfacem
cerintele normei responsabilittii sociale, ne simtim vinovati si suntem coplesiti de tristete. Norma
pretinde ca oamenii s ajute pe cei ce depind de ei (printi, copii, profesor - elev, etc.) iar
experienta ne arat c acordm ajutor cu att mai mult cu ct beneficiarii sunt mai dependenti de
noi. Trebuie ns s existe convingerea c persoana respectiv depinde ntr-adevr de noi.
Se observ ns c norma responsabilittii sociale se aplic diferentiat: exist tendinta de a
ajuta n mod deosebit persoanele dependente de noi, despre care avem o prere bun (L. Berkovitz
1979), pe cele ajunse ntr-o situatie foarte critic fr a se face vinovate n vre-un fel (pe vecinul cu
casa ars datorit furtunii ce produce un scurt circuit, dect pe cel ce-si d foc singur casei
adormind cu tigara aprins n pat). Deci cei ce "si-o fac cu mna lor" sunt mai putin ajutati, chiar
dac depind de noi - exemplu: copiii care nu-si ascult printii si trec prin situatii dificile din
aceast cauz.
A. Baum, J. D. Fisher, J. E. Singer (1985) apreciau c n baza acestei norme, nu se pot face
dect slabe predictii comportamentale, intervenind o multime de factori de context care fac
prognoza foarte dificil.
47
Experimental s-a demonstrat c observarea de modele prosociale sporeste probabilitatea de
acordare a ajutorului (J. H. Brian, N. H. Waleck 1970), att la copii ct si n cazul adolescentului
sau adultului. Cercettorii afirm c expunerea la aceste modele confer proeminenta normei
responsabilittii sociale si observnd un model, reusim s descifrm mai usor situatia n care ne
aflm.
Pe de alt parte se constat c si observarea comportamentelor antisociale poate induce prin
reactie la acte de ntrajutorare. V. J. Konecni (1972) arat c dup bruscarea verbal a unei
persoane, n cadrul unui experiment, s-a manifestat o tendint mai accentuat de ajutor din partea
celorlalti. Chiar si modul de solicitare al ajutorului influenteaz realizarea efectiv a acestuia: cerut
prea insistent, ultimativ ajutorul ntrzie sau nu mai este dat deloc.
Experimental s-a artat c moderatia n solicitarea ajutorului este mai eficace dect
insistenta (I. A. Horowitz, 1968). Probabil c atunci cnd cererea este prea insistent, intervine
ceea ce J. W. Brehm (1966) numeste "reactanta psihic", apreciindu-se prin analogie cu fizica, c
procesele psihice se caracterizeaz printr-o anumit inertie, o rezistent indus. Cnd este limitat
libertatea de actiune, resimtim o stare emotional negativ ce declanseaz dorinta de actiune
conform optiunilor proprii. Insistenta care agreseaz persoana ce solicit ajutor, amenint libertatea
optiunii si de cele mai multe ori se evit acordarea sprijinului necesar, avnd loc un "efect
bumerang".
Colectivitatea dezvolt instante formale si informale ce vegheaz la buna functionare a
acestor norme, ca legi juridice, dar si religia si codul moral include n prescriptiile fundamentale
datoria de a-ti ajuta semenul.
Iubirea aproapelui - expresie superioar a prosocialului este valoarea central n crestinism.
b) Norma reciprocitii
(Gouldner, 1960) cere c dac ai primit ajutor din partea cuiva, trebuie s rspunzi n acelasi
fel, chiar dac n viitor nu vei mai avea beneficii din partea lor. Desi accentul se mut de pe asistenta
dezinteresat, plasndu-se n paradigma schimbului social avem de-a face totusi cu acte prosociale,
altruiste, deoarece schimbul nu este direct si imediat, nu se negociaz si ne trimite de la decentrarea
egoismului pur. Teoretic, ai putea fi ajutat, fr ca n timp s returnezi ajutorul - cazuri de acest
gen, existnd multiple.
Paremiologia - disciplin ce se ocup cu studiul proverbelor, afirm existenta la toate
popoarele a proverbelor ce exprim aceast norm "a plti cu aceeasi moned". II ajutm pe cel
care ne-a fcut un bine. Exist ns cazuri cnd dup bine, urmeaz lezarea intereselor noastre. L.
A. Seneca consider c datorm recunostint celui ce ne-a fcut un bine, chiar dac rul fcut mai
trziu este mai mare "rul e mai mare, dar binele e fcut mai nainte. Trebuie prin urmare s tinem
48
seama si de timp", (retrosecvent temporal: ajutorul dat atrage comportamentul altruist, chiar dac
ulterior binefctorul a provocat suferinte morale sau fizice) .
ndemnurile morale cu care venim n contact au valoare foarte mare, dar important este
ghidarea noastr n sensul ndeplinirii lor. Apoi, n orice societate exist norme sociale alternative
"Ajuta-ti prietenul la nevoie" dar si "cmasa este mai aproape de corp" si problema care se pune n
aceast situatie este pe care dintre cele 2 variante le preferm si pn unde, la ce nivel suntem
dispusi s ne jertfim interesele, ajutndu-1 pe cellalt. Toate aceste reflectii conduc la:
c) Norma justiiei sociale
Derivat din principiul echittii formulat de Adams Smith (1965) si care afirm c trebuie
s existe o distributie cinstit (just) a resurselor si beneficiilor ntre oameni si grupuri de oameni.
Analiza cost - beneficiu, derivat din aceast teorie se ntemeiaz pe urmtoarele teze:
- oamenii tind s mentin echitatea n relatiile interpersonale, deoarece relatiile
inechitabile produc discomfort psihic;
- gradul de inechitate n relatiile dintre dou persoane poate fi calculat din raportul:
Ceea ce d persoana A Ceea ce d persoana B
Ceea ce primeste persoana = Ceea ce primeste persoana B
deci ntre cei doi actori sociali trebuie s fie un raport de egalitate, echitate.
Dac am nota cu: "i" - investitiile
"c" - cstigurile
A, B, cele dou persoane
echitatea e prezent n formula Ai/Ac=Bi/Bc
Daca relatiile dintre cele dou rapoarte este perceput ca nonegal de ctre cei implicati,
avem o situatie de nonechitate si se ncearc restabilirea echittii. Aceasta se realizeaz fie prin
ajustri pe plan comportamental (mrirea sau micsorarea costurilor sau beneficiilor proprii sau ale
partenerului), fie n plan pur psihologic - rationalizri si justificri ca "el a fcut", "dac m gndesc
mai bine, eu beneficiez mai mult", etc. n cazurile extreme, relatia didactic se poate rupe, situatia
fiind considerat total inechitabil, iar modificrile nu sunt acceptate (exemplu: n cuplul
conjugal).
J. S. Adams ntr-un studiu privind inechitatea n schimburile sociale, publicat n 1965,
remarca urmtoarele:
- gradul de inechitate e cu att mai mare, cu ct e mai favorabil raportul primei
persoane fat de a doua;
49
- modul n care oamenii rspund la inechitate depinde de obisnuinta lor, de modul de
comparare;
- oamenii ncearc s elimine stresul negativ (distresul) provocat de inechitate,
stabilind echitatea. Chiar dac termenii de "cost" si "beneficiu" sunt improprii psihologiei ei sunt
folositi si desemneaz: cost = o gam larg de factori de natur material, financiar dar si ideal,
psihic; consumarea bunurilor materiale, cheltuirea unor sume de bani, ocuparea timpului liber,
oboseal psihic, depresie, tristete, primejduirea vietii.
Asemntor, beneficiul include att recompense externe (bani, stim, ajutor reciproc) ct si
recompense interne (sporirea stimei de sine, satisfactie, sentimentul competentei, etc.).
Analiza cost - beneficiu stipuleaz c i vom ajuta pe altii, dac apreciem c beneficiul va
depsi costul implicat. Bunul simt ne arat c omul e mai dispus la ajutor cnd nu i se pretinde prea
mult, deci nu sunt necesare eforturi deosebite pentru acordarea ajutorului.
J. Daley si D. Latane (1970) verific aceast ipotez printr-un experiment, artnd c
frecventa ajutorrii e invers proportionat cu costul comportamentului; cu ct costul e mai ridicat
(exemplu: "v rog s-mi dati 10 centi" - 34%) cu att frecventa e mai redus, (fat de exemplul:
"v rog s-mi spuneti ct e ceasul" - 85%).
Proportia acestor tipuri de comportamente prosociale depind de foarte multi factori,
dintre care sistemul sociocultural, n care s-a desfsurat experimentul, dar costul pare a fi
hotrtor: cu ct ni se cere mai mult, cu att suntem mai putin tentati s intervenim.
Trebuie fcut diferenta ntre costul real si cel antecalculat (perceput) al ajutorului, iar cea
care ne permite o evaluare corect a comportamentelor noastre este experienta cu astfel de situatii.
Experienta trecut ne permite s evalum costul real al comportamentelor noastre si s
anticipm costul actiunilor viitoare. Anumiti factori situationali sau de alt natur pot introduce
corectii serioase, astfel c uneori anticipm un cost disproportionat fat de cel real. In aceste
cazuri, tendinta de a-i ajuta pe cei suferinzi este redus. I. M. Piliavin si J. Rodin (1969) au
observat c oamenii sunt mai putin dispusi s-i ridice de pe trotuar pe cei doborti de butur, s-i
sprijine pe cei oribil mutilati pentru c si imagineaz un cost prea ridicat, adic diminuarea
prestigiului lor prin asocierea cu astfel de persoane. Asa se face c de multe ori tocmai cei care au
mai mult nevoie de ajutor sunt ocoliti.
In ncercarea de a-i ajuta pe ceilalti, putem esua ajungnd ntr-o situatie similar sau chiar
mai dificil, mai critic dect cea a victimei.
Exemplu: un nottor mediu va ezita n a se arunca n ap pentru acordarea ajutorului ntr-
un caz de nec.
In aceste situatii intervine competenta ce d un anumit control situatiei respective, deci
costul ajutorului aici este sczut si de aceea se intervine. M. Hoffman (1976), H. Schwartz si G.
50
Clausen (1970) apreciau c pentru o persoan competent, costul comportamentului altruist,
prosocial este sczut si competenta creste dac suntem familiarizati cu astfel de situatii.
Alte experimente evidentiaz importanta beneficiului n realizarea ajutorului, n sensul c
dac n trecut au fost rspltiti pentru gesturile lor, oamenii le vor face mai des si n continuare.
Paradigma costuri beneficii
In sens restrns, paradigma cost - beneficiu mizeaz exclusiv pe calculul utilitar al actorului
social.
Ca o prelungire a macroeconomiei n sectorul umanului, economistii au o satisfactie
deosebit n a explica comportamentele altruiste prin calculul rational ce slujeste egoismului.
Altruismul si alte comportamente prosociale sunt determinate de functia de utilitate pe care
receptorul acestor acte le are pentru c le emite. Explicatiile dup Lemennicier sunt:
- cele mai multe gesturi asa zise altruiste nu sunt dect un profund egoism mascat
(exemplu: invitatia la mas a unui coleg ascunde interese);
- motivatia actelor altruiste poate consta n nevoia egoist de reputatie;
- chiar conduitele zilnice ce par dezinteresate (banii dati cersetorilor) au la baz motive
egoiste.
Cea mai consistent explicatie a altruismului n termenii relatiei cost-beneficiu este aceea c
atunci cnd ncep interactiunea cu altii, comportamentele lor strict individuale si egoiste determin
pierderea utilittii pentru ei nsusi, sunt nclinati s ia n considerare efectele acestor comportamente
asupra celorlalti si dispusi s le nlocuiasc cu acte altruiste.
Teorema lui Becker 1991 privind altruismul n familie demonstreaz afirmatia de mai sus
n sensul c dac exist persoane altruiste, generoase n familie acestea incit alti membrii, chiar
egoisti la acte asemntoare. Teorema se mai numeste si Rotten Kid (copilul rutcios), deoarece
Becker o demonstreaz pe un exemplu cu un foarte rutcios copil, invidios pe sora sa, care primea
mai mult atentie de la tat. Altruismul tatlui induce altruismul biatului egoist care si d seama
c dac nu se poart bine cu sora sa, el va pierde cel mai mult.
Formele altruismului
Pentru c toate definitiile afirm c altruismul presupune sacrificii de sine, si orice sacrificiu,
rneste ntr-o oarecare msur ego-ul, pentru a fi sacrificiu de sine, ecuatia psihologic "altruism =
sociabilitate" rezult chiar din definitia altruismului. Astfel, nu face obiectul unei probleme puse n
termeni psihologici "adevratii altruisti" actioneaz dup Macauly si Berkowitz (1970) mpotriva
intereselor proprii. Altruismul ideal apare atunci asociat neplcerii dar si unei anumite irationalitti,
dac se actioneaz mpotriva intereselor proprii. Expresia "adevratii altruisti" naste controverse
51
si ne ridic ntrebarea dac exist persoane despre care nu putem afirma dac sunt altruiste.
Rspunsul l caut n continuare psihologii, ncercnd s stabileasc un "model coerent de diferente
ntre indivizi". S. Moscovici.
Rushton (1980), Futz si Cialdini (1980) au observat c:
- cellalt este ajutat n anumite situatii;
- aproape nimeni nu e dispus s ajute n alte conditii;
- aceeasi persoan ce l ajut pe unul n anumite situatii, nu l ajut n celelalte sau altele.
Nu putem afirma despre cineva c este altruist sau nu putem prezice c, deoarece s-a
comportat ntr-o manier altruist ntr-un context, se va purta la fel si n altul. Totul depinde de
loc, moment, timp, stare.
Altruismul participativ
Cea mai bun imagine pentru a ilustra ideea altruismului participativ se dovedeste a fi cea a
societtilor de furnici si albine. Acestea sunt considerate societti bine integrate, cu un nalt grad de
diviziune a muncii si un procent de altruism ce impune o intens cooperare. Aici ntlnim
angajamentul fiecrui membru n vederea supravietuirii ntregului ansamblu social.
Raportat la fiinta uman, un exemplu edificator de acest tip de altruism este sacrificiul
neconditionat al soldatilor, sau munca neobosit a muncitoarelor ce contribuie la siguranta,
bunstarea tuturor.
Totusi, dac se elimin aceste exemple, rmne elementul participrii intense la viata
comun, ce presupune sacrificarea timpului, energiei si mai rar, a vietii pentru ceilalti. Pe scurt, am
putea spune c este un altruism exersat n favoarea familiei, bisericii, patriei, sub o form extrem
sau una moderat.
Alte exemple sunt oferite de catastrofele naturale, srbtori sau manifestatii publice, cnd oamenii
fac sacrificii imprevizibile, pe care ntr-o situatie normal nu le-ar face. Se creeaz astfel
identificri ntre indivizi, cea mai remarcabil fiind aceea dintre printi si copii. Edificator n acest
sens este exemplul Anei Freud, din "Le Moi et le mecanismes de deferise", 1978, unde afirm c
exist cazuri n care printii, egoisti sau altruisti le ncredinteaz copiilor proiecte pe care ei nu le-
au putut realiza si astfel se vd pe ei mpliniti.
"Altruismul este o problem a societtilor unde ncrederea n sine este subiectul unei crize"
iar religiile si Biserica au nteles acest pericol, protejndu-se prin sacrificii.
Acest tip de altruism este considerat un altruism fr cellalt; el nu se adreseaz unui
individ anume ci ntregii comunitti, oricare ar fi participantii. Dac exist pentru fiecare un altul,
atunci "noi" este ceea ce i leag pe membrii familiei, fiii unei natiuni, credinciosii unei Biserici si
urmreste sustinerea unei legturi speciale care nu poate fi cu adevrat ntrerupt. A prsi aceast
52
relatie nseamn pn la urm a nceta s existi, cci att din punct de vedere psihic ct si cultural
este imposibil s-ti prsesti natiunea, familia, cercul de prieteni, etc.
Toate acestea confirm definirea altruismului participativ ca acel tip de altruism n care
sinele si cellalt nu sunt cu adevrat distincte ci se nlocuiesc unul pe cellalt, schimbndu-si n
mod constant pozitia. Este acel punct n care altruismul si dragostea nu se mai pot distinge ci se
confund, ceea ce se face pentru cellalt este de fapt, din dragoste pentru cellalt. Este o legtur
special si un simbol al acestei legturi.
Altruismul fiduciar
S. Moscovici (1980) este de prere c oamenii, atunci cnd stabilesc o relatie de
ntrajutorare, caut un "anumit grad de ncredere, cu att mai necesar cu ct oamenii sunt mai
strini unul de cellalt".
Dac ne-am referi la o persoan care face un sacrificiu n favoarea alteia, aceasta din urm
ar trebui mcar s-i multumeasc, s-si arate recunostinta. In sens contrar, persoana care ajut va
simti o stare de nemultumire, de disconfort, de deceptie.
ncrederea care se poate naste n cazul unor asemenea gesturi poate deci fi nsotit de
recunostint, simpatie, n sens pozitiv sau de deceptie, n sens negativ. In cazul transformrii
ncrederii ofertantului de ajutor n nencredere se instaureaz o stare de tensiune dinamic. Deci, n
cazul altruismului fiduciar, ceea ce este fcut n favoarea celuilalt depinde de gradul de ncredere
sau nencredere pe care indivizii l percep sau doresc s-1 stabileasc n relatia lor. Din punct de
vedere psihologic, consecinta acestor fapte este c interactiunile sunt abordate sub semnul
incertitudinii, totdeauna, pentru c nu stim cum va reactiona cellalt.
Un exemplu edificator n acest sens ar putea fi acela n care un vecin, si cheltuieste banii si
si risipeste timpul pentru a ajuta pe cineva bolnav, dar acesta, vindecndu-se l evit pn ntr-
acolo nct nici nu-i mai vorbeste. Este clar c vecinul a svrsit un gest altruist, iar faptul c
ncrederea i-a fost nselat nu are important dac ne gndim c altruismul este "de partea sa" si va
trebui s-si caute justificri n dialogul cu sine nsusi. Deceptionat, el va ntelege c alter-ul nu este
un alter ego, un dublu al sinelui ci o persoan care actioneaz, gndeste n mod diferit. Dintr-un
anume punct de vedere el poate fi dezamgit, cci demersul su nu a avut ecoul prognozat In
ncercarea de a oferi explicatii acestor acte, Krebs (1970) porneste de la ipoteza c dorim intens s
ajutm pe cineva apropiat, care ne atrage n vre-un fel. S-a observat c atunci cnd ne gsim n fata
unei persoane aflate n suferint, oamenii si manifest de obicei empatia: exemplu, un copil care
tip n mijlocul strzii. Cu ct strigtele sale sunt mai puternice, cu att exist mai multe sanse s
fie ajutat. (Palliavin si Palliavm, 1972)
53
Mai mult, Krebs (1975) a observat c studentii de la Harvard, ai cror reactii msurate prin
teste psihologice si mrturii, denotau mai mult suferint, ca rspuns la suferinta altora, erau si cei
care ar fi ajutat cel mai mult persoana n cauz.
Gestul altruist este deci asociat proximittii empatice, dar si cresterii respectului fat de sine.
In alt studiu privitor la donatorii de snge din Wisconsin, Pilliavin et al. (1981) afirmau c a
dona snge creeaz un sentiment de auto satisfactie si o stare de confort, deci, ne simtim bine cnd
facem un bine. In general empatia si sentimentul de suferint se conjug pentru a motiva altruismul
ntr-o situatie de criz, n care cutm apropierea de ceilalti.
Amato (1986), ntr-o anchet, a intervievat persoane care n 1983 au vzut la televizor cum
un incendiu dintr-o regiune secetoas a distrus mai multe case din apropiere de Melbourne. El s-a
ocupat de felul n care s-au fcut donatii n bani si produse, observnd c persoanele care si-au
exprimat indiferenta sau indignarea au donat mai putin dect cele marcate profund de acest
eveniment, manifestnd ngrijorare si simpatie pentru victime. Din multitudinea de exemple
asemntoare reiese c persoanele empatice, preocupate de binele celorlalti ajut chiar dac stiu (sau
presupun) c nimeni nu va remarca gestul lor.
Un exemplu elocvent de altruism fiduciar este ajutorul oferit de asociatiile umanitare
(exemplu: n Africa, Bosnia Hertegovina, etc). Alte studii au evidentiat faptul c sentimentele de
culpabilitate si de tristete amplific dorinta de a ajuta. Chiar propria nefericire ne face s fim mai
sensibili la nefericirea celorlalti.
In concluzie, putem afirma c altruismul fiduciar contribuie mai ales la satisfacerea ego-ului
nostru. Cnd o persoan se simte vinovat, deprimat sau ndurerat, faptul c poate ajuta pe
altcineva i permite depsirea strii psihice negative n care se afl. Asadar, pe de o parte exist un
climat afectiv, propice altruismului fiduciar, iar pe de alta, ajutorul acordat altora reprezint un mod
de ameliorare a strii sufletesti negative, "cnd druirea este voluntar". (Cialdini et al, 1981;
Weyant, 1978).
In acest caz ne putem pune ntrebarea: cine pe cine ajut? Bunul samaritean face un gest
caritabil si restabileste contactul cu ceilalti, dar care si restabileste ncrederea n posibilitatea unor
relatii viitoare (Kohn, 1990). Victima, joac si ea un rol de mediere, simbolic, cu lumea si cu sine
nssi. Suferinta victimei nu reprezint dect motivul ocazional care declanseaz actul altruist, acea
dorint de a iesi din sine pentru a colabora, a stabili un raport de bun credint cu ceilalti. Raportul
astfel creat reduce distantele dintre sine, ego si alter si atenueaz, prin empatie, violenta tuturor
sentimentelor care ne separ n mediul social n care toti convietuim. Altfel spus, acest tip de
altruism face posibil crearea unei lumi subiective, alimentnd nssi intersubiectivitatea.
54
Altruismul normativ
Dac n cazul celor dou forme de altruism, prezentate participativ si fiduciar se poate vorbi
de folosul dat ntregii comunitti (participativul), sau de sustinerea unor relatii ntre persoane si
reducerea distantelor dintre ele, bazate pe ncredere (fiduciarul), rmne neelucidat problema
actului altruist n care intervine alt factor: norma societtii si culturii. Este cazul actului altruist asa-
zis impersonal si n care intervine ca un al treilea actor aceast norm, de unde si denumirea de
normativ".
Acest tip de altruism este considerat de specialisti ca un altruism care nu este, verificabil",
pur, dar inevitabil n psihologia social. Exemplul relevant n acest sens este dat de ajutorul de
somaj reciproc, azilurile, asociatiile de ajutor reciproc, asigurrile sociale, deci de institutii ale
altruismului normativ. Ele sunt pe reprezentarea social a acestor comportamente, a clasificrilor
de ajutoare ce se acord sau a sacrificiilor ce trebuie consimtite. Reprezentarea se axeaz fie pe
responsabilitate fie pe solidaritate, care trebuie echilibrate pentru buna functionare a unei institutii.
Norma sociala" este cuvntul cheie n jurul cruia se dezvolt acest tip de altruism,
cercetrile efectuate demonstrnd c indivizii care si-au nsusit norma de responsabilitate, se
angajeaz ntr-o relatie altruist mai mult dect cei care au interiorizat-o mai putin (Rushton,
1980).
Intr-o ampl lucrare, Straub (1974), le-a dat studentilor s completeze o serie de scale ce
contineau msura responsabilittii sociale. Pe de alt parte, ntr-un test practic autorul le-a dat
ocazia de a-si oferi ajutorul ntr-o situatie de urgent, dup cteva sptmni de la completarea
chestionarelor. Rezultatele au fost foarte elocvente, toate indicnd o legtur strns ntre
adeziunea la norme si comportamentul de ajutorare.
Alte experiente demonstreaz c oamenii, n general, doresc s ajute victimele, chiar n
cazul gesturilor anonime, n absenta recompensei sociale.
Totusi n viata de zi cu zi, ei se supun normei responsabilittii sociale ca oricrei alte norme,
selectiv, acordnd prioritate victimelor a cror suferint are cauze impersonale, ghidndu-se dup
regula: "l ajut pe cel care merit ".
Dezastrele naturale sau moartea unei persoane apropiate sensibilizeaz repede aproapele
nostru, dar ajutorul este discutabil dac este suspectat de a-si fi cauzat nenorocirea prin lene sau
imprudent. Icks si Kidd (1979), ntr-o cercetare realizat la Universitatea din Wisconsin, au
studiat impactul unor astfel de interpretri date diferitelor situatii, n care ajutorul se oferea unor
persoane care, cteodat, "pur si simplu nu au chef " de munc. Si aceste rezultate arat c suntem
tentati s ajutm pe cineva cnd ne solicit, dar cu conditia s nu existe motive "de a-i respinge
greseala, eliberndu-ne astfel de orice responsabilitate fat de acesta "(Bercowitz si Lanterman ,
1986; Schwartz , 1977).
55
In aceste situatii, maxima "Ajut-te si cerul te va ajuta ", trebuie nteleas ca "Ajut-te si
ceilalti se vor simti obligati s te ajute". Trebuie s ne ajutm prietenii, vecinii si pe toti cei care
necesit o anumit interventie, pe cei aflati n pericol, iar aceste obligatii ne creeaz nou si
asteptri in ceea ce ne priveste.
Asteptrile, prescriu un comportament altruist, deosebindu-1 de cel care violeaz anumite norme.
Exist ns si preri dup care deosebim doar dou forme de altruism; astfel, D . Rosenhan
(1972), face delimitarea ntre altruismul normativ - dictat de procesul de conformare la normele
sociale si cel autonom, care indic dezvoltarea unei implicri internalizate n existenta altora.
Acelasi autor sugereaz c exist o baz cognitiv a trecerii de la altruismul normativ la cel
autonom, care implic unele din abilittile ce se reflect n judecata moral a copilului. Acest tip de
comportament se dezvolt dup o dinamic proprie, n timp, esential fiind variabila "vrst".
Altruismul egoist sau egoismul altruist
Majoritatea psihologilor descriu altruismul ca pe o virtute, o superioritate moral, vzndu-
1 n acest caz ca pe un antidot al egoismului si al lipsei de generozitate fat de suferinta semenilor.
Se pune ns problema existentei unui altruism pur, a atitudinii sau comportamentului motivat doar
prin el nsusi. Cei mai multi cercettori rspund afirmativ acestei incertitudini, considernd
altruismul ca fiind ntotdeauna "bun si intrinsec remunerator", eliberat de orice urm de egoism.
"Altruistii egoisti" sunt considerati a fi cei ce se druie sincer, fr
retineri, sau sentimente obscure, ai cror sacrificii sunt produsul motivelor
egoiste. Altruismul egoist este unul dintre cile inconstiente de exploatare fizic,
social a celuilalt iar adeptii si ar trebui s-si reconsidere punctul de vedere si
s-si explice adevratele motive n acordarea ajutorului.
Acest tip de comportament este cercetat de psihanaliz care observ n lipsa de egoism, n
devotamentul fat de ceilalti, teama, frica intens de a ne, nfrunta dorintele cele mai intime Ana
Freud (1978), prezint cazul unei nvttoare tinere, care nu astepta foarte multe de la viat, dar
care fcuse pasiune pentru viata amoroas a prietenelor ncercnd s le ndrume spre anumite
lucruri. Moda sau orice preocupare feminin, personal i erau indiferente, dar arta mult interes
pentru toaletele colegelor, consumndu-si toat energia pentru a le usura existenta acestor
"Cedarea propriilor emotii pulsionale n favoarea celuilalt este marcat de egoism, iar eforturile
fcute pentru satisfacerea dorintelor celuilalt, creeaz un comportament care ne forteaz s-1
calificm drept altruist ".A . Freud,-1978 .
Viata, evenimentele trite, ne-au oferit cu sigurant fiecruia dintre noi asemenea exemple,
cnd entuziasmul, generozitatea, empatia pentru suferinta celuilalt, duc la panic, fiind vorba despre
teama asumrii propriilor dorinte. Exemple de egoism altruist: mama care nu cheltuieste bani
56
pentru sine, dar satisface orice capriciu fiului sau fiicei sale; studentul care ezit s rspund
pentru a-i da timp colegului s-si pregteasc argumentele.
Cele dou forme mixte de altruism, ntlnite n cadrul relatiilor interpersonale,
demonstreaz posibilittile nenumrate de actiune si interpretare ale fiintei umane, fcndu-ne
constienti de complexitatea acesteia.
Summary
One of the most frequent images of the contemporary society is that in which a man, a
human begin just like us needs help. In the struggle with life and sometimes with the ones around
him, he, the man near us is waiting for a helping hand or maybe just an encouraging word to
manage to surpass the, crisis in which be lies and not to destroy all that be gathered up tot hat
moment.
Even if most people are those who consider that the problem is not their and consequently
they have no reason to get involved, there are also people otherwise quite few, who act also in
favor of the others, they are generous, friendly, actuated by a love with no interest towards the
other human beings, offering all their means to the others without a certain purpose: the
altruists/the unselfish.
BIBLIOGRAFIE
1. Badcock, S. R. (1986) - The problem of Altruism, Oxford, Basil Blackwell
2. Baron, R., Byme D. (1991) - Social Psychology. Boston, Allyn and Bacon.
3. Batson, C. D. (1997) - Prosocial motivation: s it ever altruistic? in L. Berkowiz, Editura Advances in
Experimental social psychology Orlando. Academic Press.
4. Brehm, S. S., Kassin, S. M. (1990) - Social Psychology. Boston, Houghton Mifflin Company.
5. Chelcea, S. (coordonator) (1990) - Psihologia cooperrii i ntrajutorrii umane. Bucuresti, Editura
Militar.
6. Golu, P. (2000) - Fundamentele psihologiei sociale. Constanta, Editura Ex Ponto.
7. Moscovici, S. (1998) - Psihologia social a relaiilor cu cellalt. Iasi, Editura Polirom.
8. Neculau, A. (1994) - Psihologie social - aspecte contemporane. Iasi,Editura Polirom.
9. Pavelcu, V. (1969) - Din viaa sentimentelor. Bucuresti, Editura Enciclopedic Romn.
10. Popescu, P. Neveanu (1978) - Dicionar de psihologie. Bucuresti, Editura Albatros.
11. Radu, L, Iliut, P. si Matei, L. (1993) - Metodologia psihologic i analiza datelor. Cluj- Napoca,
Editura Sincron.
12. Radu, L, Iliut, P. si Matei, L. (1994) - Psihologie social. Cluj-Napoca, Editura EXE.
Bucuresti, Editura Didactic si Pedagogic.
13.Rudic, T. (1979) - Eu i cellalt. De la poziia egocentric la poziia altruist. Iasi, Editura Junimea.
Primit 17.11.2008
57
MODALITI DE ADAPTARE LA STRES (COPING)
Lorena-Dorina RMUREANU, Romnia
1.1. Noiuni introductive
Confruntat frecvent cu situatii stresante, fiinta uman si-a dezvoltat de-a lungul
filogenezei o serie de mecanisme prin care face fat stresului. Ele actioneaz fie preventiv pentru
a modifica sau anihila prezumtivele efecte negative ale unei situatii viitoare, fie adaptiv, n
sensul reducerii distresului dac acesta a fost deja indus.
Urmrind etapele procesului declansat de agentii stresorii, Selye descrie aceste reactii sub
numele de sindrom general de adaptare (SGA). Stresul este suma rspunsurilor nespecifice la
orice solicitare a organismului. SGA evolueaz dup Selye n trei stadii: reactia de alarm (RA);
stadiul de rezistent (SR); stadiul de epuizare (SE) (Selyes guide to stress, 1983).
Pentru a circumscrie mai exact termenul de stres, Selye realizeaz o distinctie ntre distres
si eustres.
Eustresul desemneaz nivelul unei stimulri psihoneuroendocrine moderate optime care
mentine echilibrul si tonusul fizic si psihic al unei persoane, starea de sntate si induce o
adaptate pozitiv la mediu. Stresul ce depseste o intensitate critic a unei valori variaz n limite
largi de la individ la individ este desemnat sub numele de distres.
Mecanismele de preventie si adaptare la stres sunt cunoscute sub numele de coping.
Coping-ul vizeaz toate modalittile de gestionare a stresului. Mecanismele de coping pot fi
grupate n trei mari categorii (Miclea, Mecanisme psihice de autoreglare n condiii de stres,
1997): comportamentale, cognitive, biochimice. Finalitatea acestor mecanisme diferite este
aceeasi: reducerea stresului.
Cauza imediat sau cauza eficient, cum este numit n epistemologie, a reducerii
distresului poate fi un comportament vizibil, o mediere cognitiv sau o modificare biochimic.
La gestiunea stresului concur toti acesti factori. Ceea ce ne intereseaz este cauza imediat
si/sau cauza principal care optimizeaz interactiunea noastr cu mediul, reducnd consecintele
ei disruptive.
1.2.Copingul comportamental
Cuprinde toate comportamentele care au functia de a preveni sau reduce reactia de stres.
Numrul si varietatea acestora este extrem de mare. Aproape orice comportament, ntr-un anumit
context poate dobndi functie adaptiv sau profilactic.
58
Cnd costul controlului comportamental al stresului este mai ridicat dect beneficiile
nregistrate, copingul comportamental nu reduce ci intensific distresul.
Reactia de stres este influentat nu numai de caracteristicile inerente stresorului, nu numai
de controlul parametrilor acestora ci si de feed-back-ul dinspre rezultatele controlului si de
frecventa tentativelor de adaptare la stres.
Lungimea perioadei de asteptare (rstimpul dintre luarea la cunostint despre impactul unui
stresor si momentul efectiv al actiunii acestuia), este, prin ea nssi, un factor stresant.
Controlul preventiv al stresorului diminueaz reactia de stres doar n conditiile n care este
nsotit de o reducere a incertitudinii sau ambiguittii stimulului stresant.
Studiile de laborator au artat c copingul comportamental reduce stresul doar atunci cnd:
este urmat de un freed-back asupra eficientei comportamentale; costul realizrii lui nu depseste
beneficiile; reduce ambiguitatea si/sau incertitudinile legate de situatia stresant.
1.3. Modaliti cognitive de coping (coping cognitiv)
Acestea vizeaz medierea informational a situatiei stresante, modalitti de prelucrare a
informatiei. Copingul cognitiv cuprinde totalitatea mecanismelor de prelucrare a informatiei
care au functia de diminuare a reactiei de stres. Ele vizeaz nu stresul ci informatia despre acesta.
Organismul si reduce stresul opernd nu asupra situatiei stresante ci asupra modului cum ea este
perceput, prelucrat, stocat n memorie.
Medierea cognitiv a stresului se realizeaz printr-o evaluare primar si secundar, apoi
printr-un sir de evaluri si reevaluri. Copingul cognitiv vizeaz modularea procesrilor
cognitive astfel nct consecintele stresante s fie minime.
n conditiile n care controlul individului asupra mediului si a propriilor sale reactii
biologice este adesea extrem de limitat, sistemul cognitiv capt preponderent asupra modulrii
comportamentale a reactiei la stres.
Interventia mecanismelor de coping se face fie n chiar momentul evalurii situatiei stimul,
fie dup ce aceast evaluare a avut loc (ex.: represia sau intelectualizarea traumei). n acest din
urm caz el modific reevalurile ulterioare. Orice reevaluare a traumei cu consecinte benefice
are functie de coping.
Formele pe care le pot mbrca mecanismele de coping cognitiv sunt foarte variate, de la
corectarea evalurilor initiale sau reevaluarea resurselor proprii la planificarea rezolvrii
problemei, evaziunea n imaginar, gndire magic sau rationalizarea esecului.
1.4. Modaliti neurobiologice de coping
59
Reactia de stres are o evident component biologic, producnd mutatii semnificative n
special la nivel biochimic.
Mijloacele de optimizare a reactiei biochimice la stres snt extrem de variate. Ele sunt fie
generate spontan de organismul uman ca reactie de aprare (ex: secretia masiv de endofine,
proliferarea numrului de celule ucigase natural killers - care dezvolt sistemul imunitar)
fie sunt induse deliberat de subiectul nsusi (ex: consumul de medicamente, vitamine, alcool,
droguri etc.)
Mai relevante pentru psihologul practician sunt tehnicile de relaxare care pe lng efectele
lor psihocomportamentale optimizeaz si reactia biologic de stres: antrenamentul autogen,
biofeed-back-ul si hipnoza. Prin consecintele lor biochimice aceste tehnici modific reactia
biologic de stres. Toate aceste tehnici induc o reactie de relaxare opus reactiei de stres.
De cele mai multe ori, pentru a-si reduce distresul, omul recurge simultan la instrumentele
sale cognitive, biologice si comportamentale. Mai mult, utilizarea unui tip de mecanisme
antreneaz, n mai mic sau mare msur pe celelalte.
Stpnirea stresului este o reactie global n care predomin unul dintre mecanismele
comportamentale, cognitive sau biologice.
1.2. PREVENIREA I COMBATEREA STRESULUI
Abordarea preventiv n domeniul stresului recurge la trei modalitti principale:
identificarea factorilor stresanti ct si a indivizilor si grupelor vulnerabile la stres
(ex: handicapatii);
reducerea vulnerabilittii si mrirea rezistentei organismului (prin alimentatie, efort
fizic rational etc.);
protectia prin evitarea si eliminarea agentilor ambientali fizici sau psihosociali
nocivi (Derevenco, P.; Ion, A.; Bban, A, Sresul n sntate i boal, 1992).
Combaterea i moderarea stresului prin metode psihoterapeutice
Psihoterapia este definit ca ansamblul raporturilor individuale sau de grup prin care se
urmreste n mod explicit influentarea favorabil a suferintelor psihice sau fizice. Apelul la
psihoterapie se face att pentru prevenirea stresului ct si pentru combaterea efectelor sale.
a) Terapiile de relaxare
Tehnicile de relaxare prin autosugestie verbal si imaginativ constau n atingerea
subiectului la o participare activ si constient pentru obtinerea progresiv a controlului volitiv
asupra unor structuri si functii organice predominant vegetative.
60
Cele mai folosite tehnici de relaxare sunt antrenamentul autogen si relaxarea muscular
progresiv (Miclea, M., Stres i aprare psihic, 1997).
Antrenamentul autogen (trening autogen) elaborat de Schutz (1912) desemneaz o relaxare
activ, prin dirijarea constiintei spre sine si propriu corp, viznd autocunoasterea si autocontrolul
Eu-lui n situatii tensionale provocate de ambianta psihosocial.
Procedeul const ntr-o succesiune de sase exercitii, nvtate initial cu terapeutul
individual sau n grup ntr-o ncpere linistit si n semiobscuritate pentru a usura concentrarea
prin atenuarea stimulilor exteriori, iar apoi practicate la domiciliu, de 3-4 ori pe zi, o sedint
durnd aproximativ 5 minute.
Cele sase exercitii sunt: exercitiul greuttii, al cldurii, de reglare cardiac, de reglare
respiratorie, de reglare a viscerelor abdominale, exercitiul fruntii. Antrenamentul dureaz 2-3
luni.
Relaxarea progresiv muscular Jacobson
Are la baz ideea c reducerea intensittii reactiilor emotionale se realizeaz prin
intermediul detensionrii musculare.
Muschiul relaxant elibereaz creierul de surplusul de excitatie care mpiedic functionarea
eficient a atentiei si memoriei, a concentrrii, posibilittile de decizie si selectie.
Metoda const ntr-o reducere voluntar a tonusului muscular, terapeutul nvtndu-si
subiectul s-si dezvolte simtul kinestezic tensionnd (7-8 secunde) si relaxnd (15secunde)
fiecare grup muscular ntr-o manier progresiv si ntr-o anumit ordine: biceps, triceps, flexori,
etc.
Se realizeaz n 1-3 sedinte pe sptmn, timp de cteva luni, pn la un an.
b) Tehnica bio-feedbak (Kamyic si Miler)
Metoda const ntr-un proces de antrenare a organismului n scopul modificrii unor functii
fiziologice care n mod obisnuit sunt inconstiente, involuntare si automate.
Antrenamentul se realizeaz asistat de un aparat electronic (monitor) care msoar si
furnizeaz informatii asupra unor parametri fiziologici, n timp ce organismul exercit un control
voluntar asupra lor. Odat dobndit controlul voluntar asupra unor procese fiziologice autonome,
cu ajutorul monitorului, achizitiile se transfer n situatii cotidiene, n rspunsul organismului la
stres.
c) Psihoterapia comportamental (Skinner, Lazarus, Wolpe)
61
Terapia comportamental porneste de la urmtoarea ipotez: comportamentul neadecvat,
determinat de un anumit tip de conditionare poate fi eliminat si nlocuit cu o nou conduit prin
alte conditionri.
Terapia comportamental utilizat n combaterea stresului implic cinci faze:
o analiza comportamentului inadecvat (deficit, exces, circumstante);
o definirea simptomelor;
o precizarea tehnicii sau ansamblului de tehnici ce vor fi utilizate;
o nvtarea intraterapeutic si extraterapeutic;
o evaluarea rezultatelor si validarea lor experimental.
Cele mai folosite tehnici de terapie comportamental sunt:
Tehnica desensibilizrii sistemice (Wolpe)
Se bazeaz pe principiul inhibitiei reciproce care const din asocierea unui excitant
neconditionat (anxietatea) cu un excitant conditionat, incompatibil cu primul (stare de relaxare).
Desensibilizarea se realizeaz progresiv, parcurgnd urmtorii pasi:
identificarea stimulilor care produc amenintare si stres; alctuirea unei scri
ierarhice (10-20 situatii stresante);
antrenarea n una din metodele de relaxare; asocierea relaxrii cu imagini mentale
calme;
expunerea progresiv-imaginar la situatiile stresante timp de 5 secunde, dup care
20 de secunde se practic relaxarea.
O alt variant este desensibilizarea prin imersie (flooding) care const n confruntarea
si expunerea prelungit la stimulul anxiogen, fr relaxare, pn la disparitia angoasei, printr-un
proces de abreactie.
Rolul terapeutului const n prevenirea reactiei de evitare a subiectului n contact cu
stimulul stresant. Imersia se realizeaz mai nti imaginar si apoi n vivo.
Restructurarea cognitiv
Metodele cognitive de prevenire si combatere a stresului pornesc de la interpretarea
stresului ca fiind rezultatul unor distorsiuni cognitive care conduc la conceptii si viziuni negative
(Bban, A., Rolul mediatorilor psihologici n evaluarea i adaptarea la stres, 1997).
n general se folosesc sase tehnici de restructurri cognitive:
Terapia ratiune emotivitate, care pune n competitivitate ideile irationale cu cele
rationale;
62
Inducerea de stres n care subiectul este nvtat s fac fat situatiilor stresante prin
suprimarea iritabilittii si anxiettii;
Sensibilizarea intern subiectul si imagineaz scene angoasante urmate de scene
agreabile;
Autocontrolul dezvoltarea unei atitudini ce implic sentimentul de control asupra
propriei vieti;
Blocarea gndirii subiectul este nvtat s spun Nu sau STOP ruminatiei
negative;
Modificarea monologului interior dirijarea monologului interior cu caracter ostil,
depresiv, spre unul pozitiv, optimist.
nvtarea social (Bandura si Coll)
Se bazeaz pe sinteza metodelor comportamentale, integrndu-si totodat cea mai nou
achizitie a teoriilor nvtturii si anume teoria nvrii sociale.
Cele dou aspecte esentiale ale nvtrii sociale care au rol n autoreglarea
comportamentului sunt: procesele simbolice sau cognitive (gnduri, imagini mentale, convingeri)
influentate de realitatea extern si nvtarea social prin observatie si imitatie. Este subliniat
eficacitatea ntririi pozitive (recompensa).
a) Psihanaliza
Psihanaliza este folosit alturi de psihoterapie comportamental n reducerea
vulnerabilittii la stres. Pentru diminuarea rezonantei stresului, Cox propune psihoterapia de
orientare antropologic elaborat de Fromm si Horneiy. Aceast terapie preconizeaz
dezvoltarea capacittii individului de a purta un permanent dialog cu societatea, dialog care
debuteaz initial cu anxietate si cutarea securittii, dar apoi este orientat spre integrare si
cooperare.
e) Psihoterapia nondirectiv (centrat pe client)
Terapeutul porneste de la mai multe ipoteze :
1. Oamenii sunt buni si eficienti ;
2. Omul are capacitatea de a se autodirectiona ;
3. Omul are constiinta comportamentului si motivelor care-l genereaz ;
4. Terapeutul ajut omul s se cunoasc mai bine (Bban, A., Stres i personalitate, 1998).
n final subiectul ajunge la ideea caracterului relativ si variabil al valorilor, dezvoltndu-
si ncrederea c el este cel care d valoare fenomenelor si le ierarhizeaz.
63
Summary
The means of optimization of the reaction to stress are extremely varied. They are either
generated spontaneously by the human organism as a defence reaction or are induced
deliberately by the subject himself.
More relevant for the practitioner psychologist are the relaxation techniques which besides
their psychobehaviour effects perfect the biological reaction to stress: the autogenous training,
the biofeed-back and the hypnosis.
BIBLIOGRAFIE
1. BBAN, A. (1997), Rolul mediatorilor psihologici n evaluarea i adaptarea la
stres, Editura Polirom, Cluj-Napoca.
2. BBAN, A. (1998), Stres i personalitate, Editura Dacia, Cluj-Napoca.
3. SELYE, H. (1983), Selyes guide to stress, Penguin Books Harmondswork
Middlesex.
4. DEREVENCO, P.; ION, A.; BBAN, A. (1992), DEREVENCO, P.; ION, A.;
BBAN, A, Sresul n sntate i boal, Editura Dacia, Cluj-Napoca.
5. MICLEA, M. (1997), Mecanisme psihice de autoreglare n condiii de stres, Editura
Polirom, Cluj-Napoca.
6. MICLEA, M. (1997), Stres i aprare psihic, Editura Polirom, Cluj-Napoca
Primit 04.11.2008
64
Implicarea factorilor de personalitate n sistemul om - main - mediu
Larisa ru, Doctorand
Se pune ntrebarea Ce este personalitatea?. n opinia lui P. Fraisse istoria psihologiei, ntre
anumite limite, se confund cu istoria rspunsurilor la aceast ntrebare fundamental, nainte de a
defini personalitatea trebuie s definim persoana. Persoana nseamn individul uman concret.
Personalitatea, ns este o constructie teoretic elaborat de psihologie, n scopul ntelegerii si
explicrii modalittilor de fiintare si functionare ce caracterizeaz organismul psihofiziologic pe
care l numim persoan uman. n literatura de specialitate si nu numai, exist diferite definitii ale
personalittii, fiecare surprinznd cteva aspecte ale acestui concept att de vast. n Dictionar de
psihologie de Norbert Sillami personalitatea este definit astfel: Element stabil al conduitei unei
persoane; ceea ce o caracterizeaz si diferentiaz de o alt persoan [1]. Pentru sociologie
personalitatea este expresia sociocultural a individualittii umane Dictionar de Sociologie-
coord. C. Zamfir, L. Vlsceanu [2].ntre nenumratele definitii ale personalittii, G. A. Allport d
propria definitie n lucrarea Structura si dezvoltarea personalittii ncercnd cum spune nu s
definim obiectul n functie de metodele noastre imperfecte [3]. Personalitatea este organizarea
dinamic n cadrul individului a acelor sisteme psihofizice care determin gndirea si
comportamentul su caracteristic. Pentru a ntelege mai bine, vom explica conceptele din aceast
definitie, asa cum a fcut-o Allport: Organizarea dinamic: Problema central a psihologiei este
organizarea mental (formarea structurilor sau ierarhiilor de idei si deprinderi care ghideaz, n
mod dinamic activitatea). Integrarea si alte procese organizationale sunt necesare pentru a explica
structura si dezvoltarea personalittii. Termenul implic si procesul reciproc de dezorganizare, mai
ales la acele personalitti anormale care sunt marcate de o dezintegrare progresiv. n Dictionar
de Psihologie editura Babel 1997, coordonat de Ursula Schiopu, comportamentul si gndirea...
se refer la disponibilittile generale si caracteristice pe care le exprim o persoan (fat de altele)
si care contureaz identitatea ei specific [8]. Psihofizic: Acest termen ne aminteste c
personalitatea nu este nici exclusiv mental, nici exclusiv nervoas. Organizarea sa atrage dup
sine functionarea att a spiritului ct si a trupului ntr-o unitate inexplicabil.
Sisteme: Un sistem (orice sistem este un complex de elemente ntr-o interactiune reciproc.
deprindere este un sistem, la fel si un sentiment, o trstur un concept. Un stil de comportare.
Aceste sisteme exist n mod latent n organism chiar cnd nu actioneaz. Sistemele sunt
potentialul nostru de activitate. Determin: Personalitatea este ceva si face ceva. Sistemele
psihofizice latente motiveaz sau directioneaz o activitate si o gndire specific atunci cnd intr
n actiune. Toate sistemele care compun personalitatea trebuie considerate ca tendinte determinate.
65
Ele exercit o influent directoare asupra tuturor actelor adoptative si expresive prin care
personalitatea ajunge s fie cunoscut. De-a a lungul anilor numeroase teorii ale personalittii au
fost propuse si pot fi clasificate n cteva mari abordri, fiecare asumndu-si propriul model asupra
naturii umane. Psihologii care au studiat personalitatea subliniau n fiecare abordare aspecte
diferite ale personalittii, favorizau diferite metode de cercetare si utilizau diferite standarde pentru
a realiza diferite standarde pentru a realiza explicatii multumitoare (Petersen 1997). Abordrile
teoretice majore ale personalittii sunt apropiate marilor scoli care au dominat psihologia n prima
parte a secolului al XX-lea (Petersen 1997).
Interactiunea ntre personalitate si profesie poate fi realizat prin dou directii: influenta
persoanei asupra profesiei, modificarea metodelor de a realiza activitatea, modernizarea
instrumentelor de munc si influenta profesiei asupra personalittii care duc la schimbarea si
dezvoltarea ei. Aceast interactiune poate avea un caracter att pozitiv, ct si negativ. Complexul
consecintelor negative de interactiune a profesiei asupra personalittii n psihologie este denumit
deformare profesional. Dup prerea cercettorului E. B. Rudensky (1966) aceste consecinte pot
influenta negativ asupra personalittii n ntregime, scade capacitatea de adaptare si functionare
eficient a persoanei. Psihologul rus Newman arat c: Noi stim c stresul face parte din viata
zilnic si c la nivele mai mici el poate avea un impact pozitiv, pe de alt parte, nivele ridicate ale
stresului n ultimii ani pot avea consecinte negative asupra snttii pe termen lung, plecnd de la
oboseal pn la obezitate si afectiuni cardiovasculare.
Psihologia muncii, studiind activitatea psihic si comportamentul de munc al omului n
scopul compatibilizrii sau adaptrii reciproce om masin - mediu, a preluat cadrul de gndire
sistemic prin raportarea omului la echipamente cu care lucreaz, la continutul sarcinilor, la mediul
fizic si social n care acesta - si desfsoar activitatea.
Sistemul om - masin mediu este un ansamblu format din unul sau mai multi oameni si una
sau mai multe componente fizice (masini, echipamente) care interactioneaz pe baza unui circuit
informational n cadrul unei ambiante fizice si sociale n vederea realizrii unui scop comun
(Montmollin, apud Iosif, 2001). Aceast definitie care subliniaz componentele sistemului,
interactiunea dintre ele si scopul interactiunii dintre componente (motivul pentru care a fost creat:
s transporte, s produc, s transmit informatie, etc.) descrie un sistem elementar (deseori
descriind un post de munc) care poate avea structuri diferite.
Un om si o masin (de exemplu: un operator de calculator si calculatorul); Un om si mai multe
echipamente (de exemplu testoarea care lucreaz si mai multe rzboaie de tesut); Mai multi
oameni si o masin (de exemplu: echipajul unui avion). Sistemele cu mai multi oameni opernd pe
mai multe masini simultan sunt sisteme complexe si se numesc sisteme sociotehnice. Aceste sunt
66
ansambluri de sisteme elementare sau posturi de munc iar din mediul organizational aceste sunt
simplificate de compartimente, departamente, organizatii etc.
Fiabilitatea sistemului sau siguranta n functionare, poate fi msurat pe dou ci:
- Prin probabilitatea de a realiza cu succes o anumit performant, care se afl n opozitie cu
probabilitatea de apatie a unei erori sau disfunctionri (pan, incident, avarie);
- Prin timpul mediu pentru o eroare care are, la rndul su, mai mule variante: timpul pn la
o eroare sau timpul ntre erori, etc.
Componentele de baz a unui sistem om masin - mediu:
Subsistemul om este descris prin functiile de receptie, procesare a informatiilor si de luare a
deciziilor si functia de actiune prin care se actioneaz direct asupra masinii.
Subsistemul masin este format din urmtoarele elemente: dispozitive de afisare si semnalizare,
dispozitive de comand; ntre acestea dou masina realizeaz o serie de operatii.
Subsistemul mediu influenteaz functionarea sistemului prin componentele sale date de: zgomot,
temperatur, umiditate, noxele toxice, iluminat, etc.(Pitariu 2003).
Initial preocuprile de cercetare psihologic a muncii au fost cunoscute sub numele de
psihotehnic sau psihologie aplicat care si-a a concentrat eforturile n jurul a dou mari teme:
selectia uzinal si orientarea profesional. Ulterior studiile asupra psihologiei muncii au nceput s
se constituie ntr-un cmp autonom. Cercetrile de nceput au constat n msurarea diferitor
capacitti senzoriale si functii psihice n conditiile muncii industriale, urmrind adaptarea omului
la exigentele acestei activitti. K. Pearson (1903) a fost initiatorul calculelor de corelatie iar
E.Kraepelin a introdus n 1902 constructia curbei de munc. Lucrrile de nceput sunt datorate lui
H. Munsterberg n anii 1913- 1914 care a publicat dou lucrri: Psihologia si eficienta
industrial si Fundamente ale psihotehnicii. Pornind de la ideea, c diferite miscri actiuni,
operatii de munc prezint solicitri psihologice diferite pentru a stabili gradul de prezent si
dezvoltare a diferitelor aptitudini, au fost inventate si introduse o serie de teste, dispozitive si
aparate psihotehnice. Initiatorii acestei inovatii la ndemnul lui H. Munsterberg si J. M. Lahy, au
fost: F. Baumgarten, G. Binet, R. Burdon, Ebbinghaus, W.Moede, H. Pieron, etc.
Diferite activitti de munc si conditiile n care se desfsurau acestea au fost studiate,
cercetate si investigate, pe urmtoarele domenii: 1. Oboseala: A. Mosso,E. Kraepelin, Myers, A.
Gemen; 2. Rationalizarea timpului de munc: E. Kraepelin, F. Taylor, Myers, W.Moede; 3.
Monotonia muncii: O. Lipmann, H. Rupp, W. Zapt Frazer; 4. Adaptarea masinii la om: O.
Lipmann, J. M. Lahy, G. Guyon; 5. Factori psihici implicati n accidente: Marbe; 6. Munca celor
accidentati: W. Poppereuter. n 1925, Myers public lucrarea cu titlul Psihologie industrial,
urmat ulterior de mai multe lucrri legate de psihologia muncii. Termenul de psihologia muncii
este larg, cuprinznd diferite tipuri de activitti de munc: transport, agricultur, servicii
67
administrative. Ca urmare au aprut studii psihologice naintea de al doilea rzboi mondial,
avndu-i ca reprezentanti pe : E. Mayo-descrie importanta studiilor psihosociale pentru asigurarea
unui climat propice cresterii randamentului, Bonnard a pus la punct o baterie de teste de
aptitudini tehnice, J. M. Lahy, specialist francez care a utilizat teste n selectia profesional, este
cel care a nfiintat n anii 1930 n Romnia un laborator de psihotehnic.
Relaia organism-mediu. Procesul de adaptare la mediul ambiant implic un complex de
relatii socio-umane cu dezvoltare variabil n timp ce poate deveni un raport disfunctional ca o
reactie de respingere fat de mediul nconjurtor. Interrelatia om-mediu este n mod obisnuit,
progresiv semnalnd de multe ori caracterul tolerant al individului fat de agresiunile
ambientale, modificndu-si reactiile adaptative dup natura modificrilor de mediu. Elementele
de severitate si agresiune ale mediului sunt receptate diferit, deci individualizat, astfel nct nu
poate fi formulat o corelatie direct si definit ntre stresul de mediu si caracterele reactiei de
adaptare. n aceste conditii, n functie de vulnerabilitatea persoanei, procesul poate evalua fie ca
o stare de dezadaptare total, fie ca o adaptare fragil si imprecis, cu durat variabil, fat de
unele evenimente ce apartin particularittilor de mediu. Pe aceast cale pot fi ntelese si integrate
prezenta att a tulburrilor severe de adaptare, ct si a unor forme relativ usoare de dezadaptare.
Factorii stresanti ai mediului sunt de natur si de intensitate foarte diferit, au adesea aspect
unic sau multiplu, actioneaz o singur dat sau repetat, pot fi schimbtori ca manifestare n
functie de modul lor de actiune. Curent, acestia apar la anumite intervale de timp dar pot actiona
si continuu, persistent, interesnd un individ sau o colectivitate uman. Viata de fiecare zi este
marcat de numerosi factori de solicitare psihic si fizic, pornind de la dificulttile si
modalittile de adaptare care se proiecteaz negativ att direct asupra persoanelor, ct si asupra
relatiilor acestora cu comunitatea. n liniile sale definitorii adaptarea este procesul de interactiune
a omului cu mediul su ambiant (substantial, energetic, sociomoral, informational) care se
realizeaz dinamic prin echilibrri succesive. Fat de functionalitatea sa n sistemul psihic,
adaptarea este un proces bipolar. Pe de o parte, are loc asimilarea mediului de ctre om n urma
creia acesta confer o anumit semnificatie celor percepute sau concepute, iar pe de alt parte,
are loc acomodarea omului la mediu prin care omul interiorizeaz, constientizeaz informatiile
preluate de sistemul psihic si si modifica comportamentul astfel nct sa realizeze, n dinamic
echilibrul om-mediu (n actiune). Asimilarea si acomodarea se cer privite ca doua procese care se
interconditioneaz. Asa cum nu exist asimilare fr acomodare la fel nu exist acomodare fr
asimilare. Din aceast perspectiv adaptarea mai este definit si ca un echilibru ntre asimilare si
acomodare. Adaptarea ne permite sa ntelegem c omul nu copiaz mediul, ci interactioneaz cu
el, l modific si se modific pentru echilibrare. Ceea ce confer sistemului psihic dinamism este
68
tocmai aceast permanent cutare a echilibrului cu mediul (intern sau extern), adic nevoia de
adaptare.
Starea de echilibru se obtine progresiv, prin autoreglare. Viteza de adaptare, sensul si
continutul su pot fi corectate prin interventii, att asupra subiectului ct si asupra mediului. Prin
activitatea sa omul mbogteste realitatea, mediul, iar dezvoltarea psihic este posibil si prin
nvtare, prin prelucrare. O astfel de multime are cteva caracteristici care o definesc. n primul
rnd ntre membrii care o alctuiesc are loc o uniformizare a reactiilor(Legea uniformizrii
actiunilor). Membrii grupului au un sentiment de sigurant n interiorul maselor.
Masele dup cum spune Gustave Le Bon sunt impulsive si iritabile. Cu alte cuvinte masele
pot trece ntr-un moment de la o stare, o emotie la una total opus fr a avea vre-o explicatie
foarte pertinent pentru aceasta, iar prin faptul c sunt impulsive se poate explica si atitudinea lor
profund irascibil. De asemenea masele sunt foarte credule datorit faptului c anumite
sentimente le pot fi foarte usor induse. Aceast caracteristic este valabil att n cazul maselor
mari de oameni ct si n cazul celor alctuite dintr-un numr mai mic de indivizi, deoarece nu
este nevoie de un numr mare de oameni ntr-un grup pentru ca faptele reale s fie nlocuite n
constiinta grupului respectiv de halucinatii, reprezentri care s i se potriveasc cu sistemul
grupului. Sentimentele multimilor sunt foarte simple si nu de multe ori exagerate. Violenta unor
astfel de sentimente este de cele mai multe ori foarte mare din cauza lipsei de responsabilitate la
nivelul individual. Astfel grupul este intolerant autoritar si de cele mai multe ori conservator n
convingerile sale; autoritarismul si intoleranta avnd grade diferite in functie de ras, religie sex
etc. Nu n ultimul rnd moralitatea multimilor este n general redus. Cu toate acestea multimile
sunt capabile s fac si acte de sacrificiu, mai mari dect cele pe care le-ar putea face un individ
izolat, dar n general aceste acte nu sunt rezultatul unui proces evaluativ personal, ci a
impulsivittii si a sentimentului de sigurant pe care l d grupul. Din cele pe care le-am
mentionat anterior tragem concluzia , c din punct de vedere al lui Gustave Le Bon[7] masele
sunt o form de organizare social care suport foarte multe critici, iar pe cea mai mare si cea
mai important le-o aduce el nsusi. n momentul n care masele au puterea, intervine haosul din
cauza dezorganizrii interioare pe care ele nsele sunt cldite. Cu toate ca nu putem critica
punctul de vedere al acestui autor putem totusi s facem cteva observatii cu privire la cele pe
care le afirm. Trebuie s spunem in primul rnd, definitia pe care o d Gustave Le Bon
multimilor, este prea mult general si de aici se pot ivi multe probleme, pentru c o multime nu
poate fi constituit doar de indivizi care seamn n principal prin scopul comun pe care l au si
difer din punct de vedere al convingerilor politice, sex, ras, religie. De asemenea, este
discutabil punctul de vedere al autorului conform cruia un lider carismatic poate determina
masele s actioneze hipnotic, ignorndu-si astfel propriile convingeri. Este adevrat c din
69
variate motive ntr-o mas de oameni fiecare individ se comport diferit dect ar face-o n mod
izolat, dar este greu de crezut c un om poate fi manipulat fr ca el s fie rspunztor de
actiunile sale. Actiunile fiecrui om poart n permanent amprenta individualittii si a propriului
sistem de reprezentare, a convingerilor si a credintelor personale. O perspectiva diferit asupra
comportamentului social ne este oferit de ctre Herbert Blumer (1900 1972) care transform
contagiunea mental despre care vorbea Le Bon n contagiune comportamental. n acest sens el
propune o nou teorie: Teoria reactiilor circulare. Aplicnd modelul lui Blumer la realitatea
nconjurtoare putem oferi un caz pentru a exemplifica mai bine teoria autorului. S presupunem
c la un moment dat ntr-o rezerv de spital se gsesc mai multi pacienti internati, dintre acestia,
unul dintre ei urmeaz a suporta o interventie chirurgical peste un scurt timp. Acest pacient este
linistit n ceea ce priveste reusita operatiei pentru c medicul n cauz i inspira ncredere, cu
toate acestea el discut cu colegii de rezerv cu privire la practicile medicale. Unul dintre ceilalti
pacienti i mrturiseste c este nelinistit de faptul c medicii nu mai sunt atenti asa cum obisnuiau
s fie, oferindu-i cteva exemple de neatentie a cadrelor medicale. Din acest motiv pacientul care
urma s fie operat se impacienteaz si i comunic interlocutorului su nelinistea sa. Astfel ambii
si-au schimbat comportamentele unul n functie de cellalt. Extrapolnd, putem spune c acelasi
principiu intervin si schimbrile de comportament n cadrul unor, grupuri. Membrii grupurilor
interactioneaz i astfel si schimb permanent reactiile unul n functie de cellalt, odat fcut o
schimbare la nivelul comportamentului individual ea este observat de ctre ceilalti si pentru ca
interactiunea nu nceteaz la nivelul grupului ceilalti si vor adapta, la rndul lor
comportamentele. Deci, se poate trage concluzia c aceste fenomen de contagiune
comportamental este un fenomen ciclic. n aceste conditii putem afirma c ntr-un grup este
aproape imposibil s determinm cu exactitate comportamentele fiecrui individ ca urmare a
permanentelor schimbri la care se supun acesta. n Comportamentul colectiv [1969] Herbert
Blumer face o prim i important dihotomie ntre multime si miscri sociale, clasificndu-le pe
fiecare. Blumer gseste cinci feluri de multimi. n functie de alctuirea lor ele putnd fi:
ntmpltoare (spontane si cu grad de participare redus), active (participare numeroas cu
caracter activ ridicat) si protestatare (caracter conventionalizat si scop precis). La rndul lor
miscrile sociale sunt de mai multe tipuri: regresive (ntoarcerea la forma anterioar a societtii),
reformiste (propun o nou societate), revolutionare (schimbarea radical societtii) si utopice
(schimbarea radical a societtii, dar fr un plan clar). Aceast miscare a grupurilor ntre
multimi si miscri sociale este important prin diferentele care au loc ntre aceste dou. De pild
multimile au n centrul lor individul si relatiile pe care acesta le are cu semenii si din multime,
pe cnd ntr-o miscare social societatea este n centrul ecuatiei, iar indivizii sunt importanti prin
prisma relatiei lor cu acestea. Ca si Le Bon, Blumer nu reuseste s fac o descriere complet a
70
comportamentului colectiv, lsnd cteva aspecte ale problemei nelmurite. n primul rnd
autorul nu explic n mod clar ce i determin pe indivizi s se alture unii altora n comunitti
(fie ele multimi sau miscri sociale). De asemenea nu se acord important necesar liderului
grupului de grup ti calittilor sale care l propulseaz n aceast pozitie. O alt perspectiv, total
diferit, asupra comportamentului social este oferit de ctre Ralph Turner n lucrarea cu numele
Comportament colectiv [1957]. Exist dup prerea sa o continuitate ntre comportamentul de
grup si cel colectiv.
Stresul i participanii la trafic. Stresul reprezint un aspect normal si necesar al vietii,
aspect de care omul nu poate scpa. Stresul poate genera un disconfort temporar si, de asemenea,
poate induce consecinte pe termen lung. n timp ce prea mult stres poate altera att starea de
sntate a unui individ, ct si bunstarea acestuia, totusi, un anumit volum de stres este necesar
pentru supravietuire. Stresul se poate concretiza n diminuarea normalittii functiilor sau chiar n
aparitia bolilor, dar poate ajuta o persoana aflat ntr-o stare de pericol prin ajustarea
mecanismelor de copping. Simptomele cele mai frecvente ale stresului anuntate de cei
intervievati n acest raport sunt:
La nivel fizic: oboseala, dureri de cap. deranjamente stomacale, tensiune muscular, modificarea
apetitului, modificarea dorintelor sexuale, stare de ameteal.
La nivel psihic: iritabilitate sau furie, stare de nervozitate, moleseal, predispozitie la plns,
probleme la adormire si somn agitat.
Pe lng stimulii interni, legati de personalitatea si judecata fiecrui individ, coexistenta n
grup genereaz o serie de factori externi care pot influenta comportamentul uman. Acesti factori
externi pot fi numiti generic de stres. Stresul se regseste variate forme, ns nu toate au tangent
cu traficul rutier. Principalele forme de stres care afecteaz participantii la trafic, att
conductorii auto, ct si pietonii, sunt urmtoarele:
Stresul ambiental este de tip fizic si este generat de zgomot, cldur, frig, vibratii, poluarea
aerului. Se manifest prin multiple efecte neurofiziologie vegetative, metabolice si
comportamentale, inclusiv prin deteriorarea performantelor;
Stresul urban este de tip att fizic, ct si psihosocial si este generat de poluarea sonor,
aglomeratie, problemele sociale, poluarea chimic. Se manifest prin dificultti de adaptare la un
anumit mediu, mai ales a celor nou veniti sau aflati n tranzit.
Din punctul de vedere al participantului la traficul rutier, stresul are efecte negative
asupra personalittii, prin cresterea agresivittii, a nervozittii si conduce la o autoevaluare
negativ n diferite situatii. Din punct de vedere al efectelor cognitive, se constat o incapacitate
de a lua decizii si o lips de concentrare poate fi fatal uneori. Din punct de vedere
comportamental, stresul favorizeaz dependenta de alcool si fumat, genereaz un compartiment
71
impulsiv care are efecte negative n trafic si asupra celorlalti participanti la trafic. Conducerea
sub aspectul aptitudinilor psihologice necesit o bun stare senzorial deoarece, mai ales la
viteze peste cele moderate, omului i trebuie prompte a datelor reale din trafic, o apreciere
prompt si rapid. A conduce un vehicul, implic un act de judecat facil, o decizie prompta si
util. Mai mult, conducerea implic o atentie permanent sustinut si un echilibru psihologic
pentru evitarea imprudentelor legate de trafic, avnd n vedere faptul c utilizarea drumului
public este n primul rnd o problem de integritate a sentimentelor moral-sociale, a
responsabilittii si a prudentei. Pentru a putea stabili o legtur ntre stres si trafic este necesar de
a defini traficul rutier, ca un sistem cu trei componente, care au o relatie biunivoc ntre ele.
Aceste elemente sunt urmtoarele:
Omul ca cel mai important element, prin care nu se ntelege numai conductorul auto ci si
constructorul de autovehicule, respectiv constructorul de drumuri. Aceste are o actiune
definitorie asupra celorlalte componente ale sistemului;
Drumul ca suport al sistemului; este legat de drum att sistematizarea rutier, care va fi tratat
ntotdeauna solidar cu elementul drum, ct si conceptul de trafic rutier;
Vehiculul ca parte mobil a sistemului; un caz particular este constituit de ctre om prin
participarea la trafic n postur de pieton.
Vulnerabilitatea la stres. Lazarus consider c efectul agentilor stresori depind nu doar de
propriile lor caracteristici, dar si de dou atribute nscrise n sfera personalittii subiectului,
trsturile de responsabilitate care receptioneaz actiunile lor: calitatea si amplitudinea
rspunsurilor emotionale si strategiile de adaptare mobilizate n interactiunea creat. Cele 2
trsturi de personalitate constituie imaginea rezistentei(tolerantei) sau vulnerabilitatea
subiectului la actiunea agentului stresor. Vulnerabilitatea la stres se constituie pe parcursul
biografiei subiectului analizat, n functie de traumele psiho- afective, experientele ale unor
stresuri psihice majore, inclusiv de modul cum a reusit s le domine. O important deosebit o au
si interactiunile subiectului cu o serie de factori de mediu social(familial, profesional,
institutional). Vulnerabilitatea la stres constituie o important premis pentru aparitia nevrozelor,
psihozelor reactive si a bolilor psiho somatice(acestea din urm necesitnd si coexistenta unui
teren organic predispozant). Stresul psihic las n urm 2 posibile modificri ale strii ntregului
organism:1. Cresterea rezistentei, faza solicitrii identice sau similare cu aceea care l-a generat,
n caz c subiectul a dominat, desi stresat situatia inductoare a stresului psihic.2. Aparitia unei
vulnerabilitti fat de stres, ce reprezint o capacitate a subiectului de a intra n stres mult
mai usor la actiunea acelorasi agenti stresori ce au produs stresul psihic initial n cazul n
care,acesta s-a soldat cu un esec adaptativ.
72
Nimeni nu reactioneaz n acelasi mod la situatiile stresante. Reactia depinde de subiect si de
atitudinile sale naturale si dobndite. Cu ct emotivitatea este mai mic, cu att sensibilitatea la
factorul de stres este mai pronuntat. Un anumit stil de viat numit comportament de tip A, joac
un rol important n instalarea stresului, fapt evidentiat n 1959 de Fridman si Rosenman, numit
de ei lupt mpotriva timpului si mpotriva celorlalti, cu scopul de a pstra controlul asupra
situatiilor. Comportamentul de tip A este marcat de sentimentul urgentei si de iritabilitate.
Persoanele ce reprezint un risc minimal la bolile cardio-vasculare, manifest o hiperactivitate,
tendint spre agresivitate, iritabilitate sau nerbdare, tensiune muscular permanent(cadre de
comert, sefi de ntreprinderi). Comportamentul de tip B este invers: subiectul este calm si relaxat,
fr sentimentul urgentei sau de ostilitate. Principalele trsturi de personalitate ce confer
vulnerabilitate la stres sunt: tendinte interpretative pe un fond de susceptibilitate crescut,
rigiditate, ncptnare, tendinte pronuntate egocentriste, autoconfirmare, impulsivitate, anxietate
agresivitate. De mentionat, c anxietatea(scala Taylor) se ntlneste la toti bolnavii cu boli psiho-
somatica ti este recunoscut ca un element favorizant pentru instalarea stresului psihic fiind la
rndul ei crescut, consecutiv experientei stresante. Analiznd diferite dimensiuni ale
personalittii, autorii au descris tipologii predispuse la stresul psihic cum sunt: cei cu un grad
nalt la introversiune sau neuroticism (Eysenck), cei cu rigiditate psihic(Kahu), cei cu tolerant
la frustrare sczut(Rocenzweing) ca si cei a cror motivatie de afirmare intelectual sau de
afiliere este ndrgit de factori psiho - sociali diversi(Woggle).
Am mentionat deja legtura existent ntre personalitate si profesie n sensul c persoana prin
trsturile sale caracteriale poate influenta metodele de realizare a activittii profesionale.
Persoana -ti exercit rolul profesional ntr-o manier unic si irepetabil.
Rezistenta la stres se analizeaz n aceast lucrare ca fiind o variabil global, care cuprinde n
sine si alte variabile(cele mentionate mai sus ti pe care le-am studiat). Rezistenta la stres, modul
de reactie la stres este determinat pe de o parte de caracteristicile agentului stresogen, iar pe de
alt parte de particularittile de personalitate care reactioneaz ntr-un anumit mod la actiunea
agentului stresogen. Anumite aspecte ale personalittii soferului implicate n managementul
stresului au devenit tinta atentiei noastre n cercetarea dat.
Statisticile mondiale evidentiaz, n 80% din accidentele de trafic, participarea semnificativ a
factorului uman, care constituie deci elementul cel mai important n determinismul lor. Chiar dac
aparent accidentele se consider datorate nerespectrii regulilor de circulatie, cum ar fi mai ales:
viteza excesiv, depsirea excesiv, depsirea neregulamentar si altele se constat de fapt c
starea de sntate sau comportamentul persoanei, echilibrul bio-psiho-social, influenteaz n mod
negativ sau pozitiv conducere n conditii de securitate rutier, sau, dimpotriv expun la accidente.
Particularittile structurii psihice, exprimate n comportamentul celor ce utilizeaz drumul public,
73
sunt considerate factorii primordiali n geneza unui accident, datorit solicitrilor pe care le
implic, ca o conditie ce favorizeaz relevarea unor factori psihologici dizarmonici.
Obiectul cercetrii l-a constituit particularittile de personalitate a conductorului auto cu
nivele diferite a rezistentei la stres.
Scopul cercetrii a constat n determinarea particularittilor personalittii conductorilor
auto cu nivel diferit al rezistentei la stres precum si n elaborarea si implementarea unui program
de dezvoltare a rezistentei la stres, implicit si a trsturilor de personalitate care contribuie la
aceasta si sunt adecvate unui comportament de sigurant rutier.
Unele dintre obiectivele operaionale naintate au fost:
Analiza literaturii stiintifice; elaborarea strategiei de organizare si realizare a investigatiei;
metodologiei de desfsurare a experimentului; selectarea esantionului; Cercetarea pe cale
experimental a particularittilor de personalitate ale soferilor cu rezistent nalt si sczut la
stres; Selectia instrumentarului metodic; Identificarea si descrierea rolului factorilor de
personalitate n manifestarea rezistentei la stres.
Metodologia utilizat de noi s-a bazat pe ideea complementarittii metodelor si tehnicilor de
culegere a datelor. Am utilizat metoda testrii n form scris, care a presupus efectuarea testelor
de ctre subiecti: Metodica Holms si Raghe pentru diagnosticul nivelului de rezistent si
adaptare la stres; Inventarul de personalitate Cattell, Chestionarul de personalitate Eysenck,
Testul K. Thomas pentru diagnosticul comportamentului n situatie de conflict; Testul K.
Leonhard pentru determinarea accenturilor de caracter.
Rezultatele cptate dovedesc c conductorii de transport auto necesit cunoasterea
propriului potential, aprecierea adecvat a propriilor capacitti si posibilitti, suport psihologic si
cunoasterea unor tehnici pentru a depsi situatiile de trafic existentiale deoarece reactia depinde
de subiect si de aptitudinile sale naturale si dobndite, de trsturile de personalitate.
Am constatat si am confirmat n lucrarea noastr c sensibilitatea la factorul de stres este mai
pronuntat cu ct emotivitatea este mai mare, cu ct e mai mare irascibilitatea, rigiditatea
psihic, anxietatea, nencrederea n sine, conflictele interioare, cerintele exagerate, cu ct e mai
putin echilibrat sistemul nervos, si redus capacitatea de autoreglare.
n urma unor activitti special organizate de tip training orientat spre dezvoltarea rezistentei
la stres, a echilibrului emotional au putut fi obtinute rezultatele scontate. Astfel n urma
activittilor de dezvoltare participantii au devenit mai putin anxiosi, cu mai putine temeri,
ngrijorri; si-au dezvoltat un mai bun echilibru emotional, fluctuatiile de dispozitie au devenit
mai putin intense, au dobndit o stabilitate emotional mai mare, au devenit mai toleranti la
frustrare, a sczut anxietatea, au devenit mai calmi, cu mai mult ncredere n fortele proprii, a
sczut tensiunea si ncordarea interioar.
74
Summary
The process of adaptation at environment involves a complex of socio-human relations with
variable development in time that can become a dysfunctional report as a reaction of rejection at
the environment. The interrelation human - environment is usually progressive pointed often out
persons tolerant character toward the environmental aggression. Therefore after environment
modification is modified the adaptive reaction. The environments elements of severity and
aggression are comprehended in different ways, individually, that is why it cant be formulated a
direct and definite correlation between environmental stress and reactions character of adaptation.
In these conditions in accordance with persons vulnerability, the process can perform or like a
case of total disadaptation or like a fragile and imprecise adaptation with variable duration
therefore some events that belong environments particularities. The state of balance is progressive
obtained through self-regulation. Through self activity the people enrich the reality, the
environment. But psychical development is also possible through study and processing.
The particularities of psychic structure, expressed in persons behavior that uses public way are
considered the primordial factors in genesis of some accident. These things are happened thanks of
application as a condition that favor appearance of some disharmonic psychological factors.
Bibliografie
1. Dictionar de Psihologie de Norbert Sillamy, Bucuresti 1997.
2.. Dictionar de Sociologie - coord. C. Zamfir, L. Vlasceanu, Bucuresti 1997.
3. G. W. Allport- Structura si dezvoltarea personalittii, Bucuresti 1981.
4. Darabont,A.,s.a., Combaterea polurii sonore si a vibratiilor, Bucuresti, Ed.Tehnic 1975.
5. Transportul terestru, mediul si sntatea. GRTD, Bucuresti, 1997.
6. Bogathy, Z.- Introducere n psihologia muncii, Tipografia Universittii de Vest, Timisoara
(2002).
7. Gustave Le Bon, Psihologia multimilor, Filipesti, Editura Ante XX Pres ,1996.
8. Ursula Schiopu, Dictionar de psihologie, Editura Babel, 1997.
Primit 12.11.2008
75
CLIMAT SCOLAIRE CENTRE SUR LEVALUATION
1
Elena COCORAD, Marcela Rodica LUCA, Aurel Ion CLINCIU & Mariela
PAVALACHE-ILIE
2
Rsum
Le rle dcisif de lvaluation sur les relations enseignants-lves, sur leurs sentiments (dquit,
de scurit, dappartenance ou mme dautoefficacit), les multiples fonctions et facettes de
lvaluation nous ont dtermin proposer un nouveau concept <climat scolaire de lvaluation>.
Le climat de lvaluation est un noyau du climat, avec un grand impact sur la vie scolaire.
Notre tude se propose de mesurer le climat scolaire centr sur lvaluation et la comprhension de
ses composantes. Les sujets de ltude ont t des lves de la IXe, Xe et XIe anne et linstrument
a t pass en deux situations contrastantes aux lyces reconnus pour leur climat trs bon et aux
lyces de lautre ple. Ltude a utilis un questionnaire avec des questions fermes, cr par les
auteurs.
Pour les deux types de lyce, theoriques et techniques, notre hypothse est valide, les deux
climats entant en contraste: les diffrences entre les coles sont plus grandes que celles rsult du
genre. Les reprsentations des lves de la mme clase et de la mme cole ont une bonne
cohrence interne, donc le climat du niveau mezzo peut tre mesure par les investigations au
niveau micro. Le niveau dtudes et le genre des sujets influencent aussi les phnomnes connexes
aux valuations. Les mcontentements, la colre, la vengeance des lves face aux erreurs
techniques ou thiques des profs augmentent vers la fin du lyce et aux garcons.
La possibilit dexprimer le climat scolaire de lvaluation par un indice est confirme. Le facteur
F1 qui mesure mieux la grandeur de microviolence lie lvaluation est diffrent dune cole
lautre et donne de corrlations indirectes avec les performances scolaires. En conclusion, loutil
labor perme de diffrencier les climats scolaires dune cole par des enqutes au niveau de la
classe.
Mots-cls: le climat scolaire, valuation, genre.
1. Cadre thorique
Le climat scolaire est une construction cognitive qui permet aux sujets dattribuer une signification
densemble aux lments issus de lanalyse perceptive de lenvironnement ducationnel (Janosz,
Georges & Parent, 1998) en donnant du sens aux situations vcues et en utilisant les connaissances
1
Ltude a t ralise dans le cadre du projet de recherche <valuation et micro violence dans le milieu
scolaire. Relations, prvention et intervention> CNCSIS Roumanie no. 4GR/20.05.2007, thme 16/943 et a t
present au 20eme Colloque de l'ADMEE-Europe, Evaluation en tension, 9-11 janvier, Geneve.
2
Chaire de Psychologie, Universit Transilvania de Brasov, Romanie
76
stockes en mmoire et les donnes issues du milieu. Par limpact sur les performances, sur le
bien-tre des acteurs, le climat scolaire devient le point du dbut pour des multiples interventions.
Les dfinitions du climat scolaire sont varies: milieu scolaire, milieu dapprentissage ou systme
social des normes et des attentes (dsirs) partages (Brookover et al., 1978), la perception des
lves sur la personnalit de lcole ou la sant de lorganisation (Freiberg, 1999). Parfois le
climat scolaire est confondu avec la culture scolaire et autre fois la culture scolaire est subordonne
au climat scolaire. Ashforth (1985) essaye de raliser la distinction entre la culture scolaire et le
climat scolaire en expliquant que pendant que la culture consiste en valeurs, convictions, opinions
partages, le climat scolaire aurait comme cible les perceptions sur des comportements.
Le climat scolaire reprsente une caractristique relativement stable qui est peru par les
participants, affecte leur comportement, ayant comme principal lment les perceptions collectives
sur le comportement dans lcole (Hoy, Tarter & Hoy, 2006). Dans un des premiers ouvrages sur
le climat scolaire, Halpin et Croft (1963) considrent le climat comme personnalit de lcole,
un ethos, une atmosphre de lcole, plac sur un continuum partant douvert vers ferm (cit par
Hoy & Sweetland, 2001).
Le climat scolaire a t considr comme une composante importante de l'cole, ainsi quun
lment prdictive du succs scolaire. Parmi les enqutes pilot qui poursuivent la russite scolaire,
on trouve celle de Coleman et al. (1966). Ses rsultats prouvent que le plus grand poids dans
lexplication des diffrences de russite ducationnelle appartiennent aux variables du milieu
familial, surtout le niveau dinstruction des parents, pendant que les variables intra scolaires
(curriculum, les dotations, la qualification des enseignants et le niveau de salarisation) ne
dmontrent pas un gros poids dans lexplication des diffrences de la russite ducationnelle.
Rutter a repris le dmarche de Coleman pour la Grande Bretagne, mettant en vidence le rle qui
revient la qualit de la relation enseignants-lves, la prparation et l'organisation des activits,
la coopration (cit par Giddens, 2000).
Le volume de la population scolaire et le type de la communaut influencent le climat scolaire:
pendant que la population scolaire saccrot, le climat devient de plus en plus ngatif, les coles
rurales ont dun climat plus positif que les coles urbaines et les coles primaires bnficient dun
climat plus positif que les secondaires. La discipline et les attitudes des lves influencent le climat
et la prsence du directeur dans et autour du campus scolaire est corrle avec lamlioration du
climat scolaire, avec la diminution des problmes scolaires (Keesor, 2005) et avec lamlioration
de la communication lves-professeurs (Waters et al., 2004, cit par Gentilucci & Muto, 2007).
Une telle approche ainsi que les assistances frquentes, actives et de longues dures aux leons
prouvent aux lves que les directeurs sont intresss de leurs problmes et russites
77
ducationnelles, les mobilise fournir plus defforts pour obtenir des succs (Gentilucci et Muto,
2007).
Hoy & Hannum (1997), dans leurs recherches sur la sant du climat scolaire en New Jersey,
trouvent des corrlations entre le climat scolaire et la russite scolaire sans tenir compte de statut
socio-conomique des lves. Cependant, d'autres tudes ne soutiennent pas la corrlation entre le
climat scolaire et la russite scolaire (Mok & McDonald, 1994). Hoy & Hannum (1997)
soutiennent la prvalence du climat scolaire par rapport au style managrial: le climat scolaire
exprim par lengagement des professeurs, laccent mis sur le succs scolaire, lappui des
professeurs aux lves sont des mdiateurs des effets du style managrial et facilitent le succs.
Le milieu de lcole ou de la classe a un effet profond sur la satisfaction des lves, ce qui
contribue d'une manire indirecte la russite scolaire. Les coles bnficiant dun climat positif
sont celles o respire la confiance, le respect, lassistance mutuelle, celles o on encourage
lapprentissage, ainsi que le soin pour lautre (Samdal, Nutbeam, Wold & Kannas, 1998) .
Lexistence dun habitus de la russite scolaire domine les coles efficientes (Hoy, 2002) qui sont
caractrises aussi par: une direction ferme, attentes leves des professeurs par rapport au succs
des lves, linsistance sur les comptences de base, milieu disciplin et une valuation
systmatique des lves. Les coles qui sont efficientes et agrables/ attractives possdent un
climat d'apprentissage positif et une direction qui appuie linstitution et le maintien dun tel climat
(Edmonds, 1979).
Certains chercheurs trouvent une corrlation positive entre larchitecture de lcole, comme
lment du climat scolaire et la russite scolaire (Deal & Peterson, 1999, cits par Holt & Smith,
2002): larchitecture de nos jours dessine un milieu plus intime, propice lapprentissage et la
motivation des lves et des professeurs. Dans les coles modernes, les rsultats des testes sont
meilleurs; de plus, larchitecture de lcole influence la discipline: les coles modernes bnficient
dun climat plus disciplin (Bowers & Burkett, 1989).
Peu de recherches ont t ddies en Roumanie ce problme. Celles effectues par lInstitut des
Sciences de lEducation ont identifi les blocages induits par une culture de la routine dans la
voie de la reforme: a) le professeur est vu comme employ et llve - subordonn; b) on exacerbe
les valeurs du contrle; c) on vite les discutions sur les conflits sans solutions; d) on communique
surtout verticalement (Iosifescu, 1998). Les conclusions sont confirmes dans une autre etude qui
constate le caractre bureaucratique excessif de la culture organisationnelle de lcole roumaine, en
identifiant le manque dinitiative, le centrage excessif sur le fournisseur dducation et non sur le
client, le sentiment du provisoire, labme entre gnrations, le sentiment de linefficience et/ou de
linutilit de lcole, la clture de lcole par rapport la communaut (Miroiu, A., 1998). Par la
suite, des analyses de la relation entre la culture organisationnelle et les projets de coopration
78
internationales mettent en vidence certaines particularits de la culture scolaire: la distance envers
le pouvoir, lvitement de lincertitude et lordre comme valeur fondamentale (Iosifescu, 2004).
La Troisime Etude Internationale concernant les Maths et les Sciences (TIMSS, 2000) a identifi
parmi les plus importantes problmes dans les coles roumaines: lcole buissonnire,
labsentisme, les prjudices physiques entre les lves, lintimidation ou labus verbal sur les
lves, les professeurs et sur le personnel de service, la mise en retard la classe et le vandalisme.
Les pourcentages sont plus lves que la moyenne internationale lexception du vandalisme.
Malgr tout cela, une premire stratgie du Ministre de lEducation, de la Recherche et de la
Jeunesse concernant la diminution du phnomne de violence scolaire dans les units
denseignement secondaire vient de paratre peine dans lanne 2007.
Le Rapport de la Commission prsidentielle, analysant la position de l'enseignement roumain
envers les indices Lisbonne et les rsultats aux valuations internationales PISA, TIMSS, PIRLS,
prouve linefficacit de lducation et du climat organisationnel: la majorit des coles de
Roumanie ont une architecture qui corresponde une conception du fin de XIXe sicle, la
ressource humaine vieillisse d'une faon inquitante et seulement une petite partie du personnel
didactique (18%) a suivi un stage pour lutilisation de linformatique. Le management des units
scolaires a t politis excessivement, en entravant laccumulation du know-how. La qualit de la
prestation didactique est apreci comme mdiocre par 74.3% des lves de la 8e classe (Miclea,
2007).
Le rle dcisif de lvaluation sur les relations enseignants-lves, sur leurs sentiments (dquit,
de scurit, dappartenance ou mme dauto efficacit), les multiples fonctions, facettes et
dimensions de lvaluation nous ont dtermin proposer le nouveau concept <climat scolaire de
lvaluation>. Ce climat scolaire de lvaluation est, en notre vision, un noyau du climat, avec un
grand impact sur la vie scolaire. Les moments d'valuation scolaire comportent des enjeux qui
produisent parfois des confrontations entre les enseignants et les lves. Les perceptions des
enseignants et des lves sur la clart des rgles, la justesse des valuations diffrent et c'est,
probablement, la source des rapports tendus et d'un climat ngatif de l'valuation.
2. Dmarche
Lobjectif de notre tude vise la diagnose du climat scolaire centr sur lvaluation et la
comprhension de ses composantes. Les 370 participants, 173 filles et 197 garons, sont des lves
de la 9e et 11e anne dans deux types d'coles: deux lyces rputs pour leur bon climat (51 et 105
lves) et autre deux lyces (100 et 82 lves) et une cole professionnelle situs, de ce point de
vue, au ple ngatif (30 lves).
Hypothses sont les suivantes:
79
H 1. Le climat scolaire varie en dpendance du type du lyce.
H 2. Les reprsentations des lves sont diffrentes en dpendance de leur niveau des tudes (IXe
et XIe anne).
H 3. Le genre dtermine des diffrences significatives entre les reprsentations comprises dans le
climat.
Pour la diagnose du climat scolaire de lvaluation, nous avons utilis un instrument original,
compos de 28 questions fermes, qui groupent 131 items items, presque galement distribus en
cinq dimensions climat relationnel, climat ducatif, climat dquit, climat de scurit, pratiques
valuatives). Pour chaque question il y a ditems minium 3, maximum 9 qui prsentent une
gradation naturelle du phnomne dcrit; chaque item a une chelle de Likert en 3-5 points pour
mesurer lintensit, la dure ou la frquence des attitudes et des comportements ngatives
investigus. Le questionnaire a t valide et a dmontr de bonnes qualits mtriques.
- Le facteur "F1Climat relationnel total", compos de "Frustrations/ hostilit" + "Atmosphre
scolaire" + "Climat relationnel",
- Le facteur "F2Climat ducatif total", compos de "Critres de notation", "Climat ducatif",
"Respect/ politesse",
- Le facteur "Climat scolaire total" compose de "F1"+"F2" (Cocorad, Clinciu, Pavalache-Ilie,
Luca, 2008).
3. Rsultats et discussions
3.1 Le climat scolaire varie en dpendance du type du lyce
Il est gnralement admis que dans les coles de bonne rputation on a un bon climat, on
promeuve les rgles statues, les lves estiment que les connaissances et lintelligence sont
valoriss par les notes, pas par des facteurs externes a lapprentissage. Mais quant aux coles de
rputation modeste on parle toujours d'un climat dfavorable aussi. Par exemple, Janosz et al.
(1998) affirmaient qu'un bon climat favorise les apprentissages scolaires et sociaux et que les
rsultats scolaires peuvent tre considrs comme des indicateurs du climat.
Dans notre recherche, la premire catgorie d'tablissements, considrs par les parents et les
lves comme des coles dsirables, attirent par le prestige, par les procdures de slection dans le
secondaire suprieur ( base des rsultats dans le secondaire infrieur), les meilleurs lves de
chaque contingent. Les coles rputes sont des lyces de la filire thorique et celles moins
rputes sont des lyces de filire technologique et des coles professionnelles (coles des arts et
80
mtiers)
3
les coles de la deuxime catgorie, surtout l'cole professionnelle, etant considres
comme des coles de la dernire chance.
En mme temps. le niveau intellectuel et socio-ducatif des lves peut intervenir comme variable
mdiatrice ou modratrice du climat. Une analyse des donns dmographiques de la population de
la recherche soutient l'ide: la proportion du milieu urbain de rsidence est la plus leve pour les
lves des lyces thoriques et la moins leve pour les lves des coles des arts et mtiers. Les
trois groupes diffrent de la mme manire en ce qui concerne le niveau d'ducation des parents.
De plus, les lves des coles des arts et mtiers proviennent des familles plus nombreuses que
ceux des autres coles. Tous les tests de signification pour la diffrence des moyennes des
variables mentionnes en haut sont significatifs.
Une premire image de la relation entre le climat et rsultats scolaires (notes moyennes) est
prsente dans le Tableau 1. Entre les deux types de variables il y a des corrlations significatives
au seuil de ,000 pour chaque facteur et pour le climat scolaire total.
Tableau 1 Corrlations entre les facteurs du climat scolaire et les rsultats des valuations
Disciplines
F1- Climat relati-
onnel
F2- Climat duca-
tif
Climat scolaire
total
Pearson Correla-
tion
-,395(**) -,340(**) -,398(**)
Sig. (2-tailed) ,000 ,000 ,000
Moyenne
Langue
Roumaine
N 271 289 260
Pearson Correla-
tion
-,256(**) -,190(**) -,249(**)
Sig. (2-tailed) ,000 ,001 ,000
Moyenne
Mathmatiques
N 271 290 260
Pearson Correla-
tion
-,405(**) -,325(**) -,407(**)
Sig. (2-tailed) ,000 ,000 ,000
Moyenne
Gnrale
N 260 276 250
Les diffrences des rsultats scolaires entre les coles rputs et non rputs sont assez videntes
(Tableau 2). Les rsultats du test F de ANOVA montrent que entre les trois types d'coles il y a des
diffrences significatives pour tous les rsultats scolaires considrs comme importants.
Tableau 2 - Test F de ANOVA pour les diffrences de notes moyenne entre les 3 types d'cole:
lyces thoriques, technologiques et coles des arts et mtiers
3
Dix-huit ans de dtresse de l'industrie dans l'conomie roumaine ont affaiblit considrablement l'enseignement technologique (lyces
technologiques et coles des arts et mtiers). C'est ainsi que les spcialisations qui mnent vers l'industrie ont devenu des options de secours, pas
les options de premire main pour les lves.
81
Variables
Lyces
thoriques
Lyces
technologiques
Ecoles des
arts et mtiers
F Sig.
Note moyenne Langue
roumaine
9,10 7,14 6,64
160,066 ,000
Note moyenne
Mathmatiques
8,69 6,25 6,01
190,057 ,000
Note moyenne gnrale 9,44 8,06 7,50 278,537 ,000
C'est galement difficile d'attribuer le niveau des rsultats seulement aux particularits socio-
conomiques des lves ou aux particularits du climat. Peut-tre que les relations entre climat,
rsultats scolaires et autres variables individuelles sont plus complexes qu'une simple relation de
covariance.
Tableau 3 - Test F de ANOVA pour les diffrences inter-groupes entre 3 types d'cole: lyces
thoriques, lyces technologiques et coles des arts et mtiers concernant les dimensions du climat
Dimensions
Ecoles des
arts et mtiers
Lyces
technologiques
Lyces
thoriques
F Sig.
Climat ducatif 23,69 25,11 23,47 6,282 ,002
Climat relationnel 26,54 28,52 23,81 14,268 ,000
Frustration/ hostilit 23,86 23,75 18,51 20,974 ,000
Atmosphre scolaire 27,83 28,96 24,94 11,423 ,000
Critres de notation 24,26 24,44 20,98 9,365 ,000
Respect/ politesse 6,78 7,35 6,89 2,329 ,099
Les diffrences entre les trois groupes, concernant les dimensions du climat scolaire, sont
significatives (p= ,002 ou mieux) pour 5des 6 dimensions, l'exception de "Respect /politesse"
(voir Tableau 3). Les scores les plus levs, indiquant un climat ngatif, on t enregistrs dans les
coles moins rputes (coles des arts et mtiers et lyces technologiques), mais mme entre eux il
y a des diffrences significatives. On peut parler ainsi d'une diffrenciation du climat entre les trois
types d'cole. Selon les donnes prsentes dans le Tableau 3, le climat ducatif, le climat
relationnel, l'atmosphre scolaire sont les plus dtendus dans les lyces thoriques le plus tendus
dans les lyces technologiques. De mme, les critres de notation sont perus comme incorrects et
les lves se plaignent du manque de respect de la part des profs. Les lves des coles des arts et
mtiers sont les plus frustrs des trois groupes.
En dpit des diffrences significatives, c'est impossible de ne pas remarquer le fait que les lves
des coles moins rputes peroivent le climat scolaire d'une manire similaire, par contraste avec
ceux des lyces thoriques. L'analyse ANOVA post-hoc (Bonferroni) montre que les diffrences
hautement significatives se trouvent parmi les lyces thoriques d'un part et les lyces
82
technologiques et les coles des arts et mtiers d'autre part. Il n'y pas des diffrences de climat de
mme ampleur entre les deux derniers types, ce qui concorde avec leurs rputations respectives.
Les lves des coles moins rputs ont des ractions ngatives plus frquentes face aux notes
reues, ils se trouvent toujours en guerre avec leurs profs. Les attitudes protestataires,
revendicatives, le sentiment de la rupture entre les deux catgories de valeur (valeurs des
enseignants et valeur des lves) forment les notes dfinitoires du climat valuatif des lyces
techniques et des coles des arts et mtiers.
Quant aux diffrences pour les scores composites, issues la suite de l'analyse factorielle, les
diffrences se maintiennent dans la mme direction (voir Tableau 4) et au mme niveau de
signification:
- Le facteur "F1Climat relationnel total" a le score le plus levs dans pour les lyces
technologiques et le plus bas (climat positif, dtendu) pour les lyces thoriques. Les diffrences
intergroupes sont trs significatives,
- Le facteur "F2Climat ducatif total" suit la mme tendance.
Le facteur "Climat scolaire total" (F1+F2) peut ainsi indiquer la diffrenciation nette entre les trois
types d'coles. On peut ainsi exprimer le climat scolaire de lvaluation par un indice/ score
synthtique caractristique pour chaque type d'cole (voir Tableau 4) qui pourrait servir comme
indicateur tmoin pour les effets des interventions d'amlioration ventuelles.
Tableau 4 - Test F de ANOVA pour les diffrences entre 3 types d'cole: lyces thoriques,
technologiques et coles des arts et mtiers concernant les facteurs synthtiques du climat
Facteurs
Ecoles des
arts et mtiers
Lyces
technologiques
Lyces
thoriques
F Sig.
F1-Climat relationnel
total
78,44 80,92 67,39 17,898 ,000
F2-Climat ducatif total 55,00 57,05 51,36 9,551 ,000
Climat scolaire total
(F1+F2)
134,07 138,76 118,74 16,951 ,000
Il faut ajouter, quil y a ici une ventuelle variable confondue - le genre: les filles forment une
majorit aux lyces thoriques (75%) et une minorit aux lyces techniques et coles des arts et
mtiers (26%). Malgr ce constat, les diffrences entre les coles sont plus grandes que celles qui
rsultent du genre, validant lhypothse. Les reprsentations des lves de la mme classe et de la
mme cole ont une bonne cohrence interne, donc le climat du niveau mezzo peut tre mesure par
les enqutes au niveau micro.
83
3.2 Les reprsentations des lves sont diffrentes en dpendance de leur ge/ niveau des
tudes
L'ge/ niveau des tudes influence les phnomnes ngatifs connexes aux valuations. La colre, la
vengeance des lves face aux erreurs techniques ou thiques des profs, la perception du manque
de valorisation de llve en chec devrait diminuer en faveur dun climat positif vers la fin des
tudes. Les rsultats de notre recherche montrent que la situation est diffrente. Trois des six
dimensions du climat scolaire centr sur l'valuation sont "aggraves" vers la fin des tudes (voir
Tableau 5): le climat ducatif et relationnel deviennent de plus en plus tendus et la politesse et le
respect diminuent d'une manire significative. Pour les indicateurs synthtiques du climat scolaire,
les diffrences significatives se maintiennent dans la mme direction.
Tableau 5 - Test t pour les diffrences entre 2 groupes d'age/ classes concernant les dimensions
et les facteurs synthtiques du climat
Dimensions Classe N Moyenne t df Sig. (2-tailed)
IXe 180 23.5278
Climat ducatif
XIe 151 24.4901
-2.420 329 .016
IXe 175 24.9429
Climat relationnel
XIe 152 26.7895
-2.381 325 .018
IXe 180 6.6611
Respect/politesse
XIe 153 7.3595
-3.405 330.995 .001
IXe 172 52.6860 F2 - Climat ducatif
total XIe 144 55.1389
-2.131 314 .034
IXe 153 124.2484
Climat scolaire total
XIe 129 131.1938
-2.130 280 .034
L'explication de cette escalade de l'animosit rside dans l'accumulation des frustrations, au cours
des annes et dans les diffrences de perspective sur l'valuation, la manque de la confience, la
perception de l'insecurit, des sentiments identifis aussi dans des etudes interculturelles (Samdal,
Nutbeam, Wold & Kannas, 1998). Il est possible que vers la fin des tudes, le climat devient plus
tendu cause des enjeux de l'valuation: les notes deviennent de plus en plus lies la
classification scolaire et par consquence l'accs aux chelons suprieurs de l'enseignement ou de
la professionnalisation. Les tensions entranes par des moments successifs d'valuation affectent
le climat. Au niveau des indicateurs synthtiques, les plus affects sont le climat ducatif total et le
climat scolaire total. On peut parler d'une dtrioration du climat de l'valuation, pour notre
population, vers la fin des tudes.
84
3.2 Le genre dtermine des diffrences significatives entre les reprsentations comprises dans
le climat
Lhypothse de la diffrence de genre est confirme pour 3 des 6 dimensions. Les garons ont des
scores plus levs pour toutes les dimensions, mais les diffrences sont significatives seulement
pour le climat relationnel, la frustration/ hostilit et les critres de notation (voir le Tableau 6).
Les filles sont plus attires par la qualit de lvaluation, dsirent que les rgles concernant les
fraudes scolaires soient strictement appliques, elles sont presque toujours daccord avec les
attitudes svres des enseignants. Les garons sont plus rebelles, suspicieux, mcontents et
contestataires des rgles. Les filles se sentent rarement menaces, se sentent rarement victimes des
valuations injustes et gnrent aussi peu de microviolences en situation dvaluation. Souvent,
elles sont contentes de notes reues, estiment que la rapidit du feed-back est satisfaisante. Les
garons sont l'origine de la de la plupart des actes de microviolence contre les enseignants, mais
aussi des victimes. Probablement le conformisme plus accentu des femmes, leur besoin dtre
accepts influencent ces diffrences de genre au niveau des comportements et des perceptions.
Tableau 6 - Test t pour les diffrences de genre concernant les dimensions t les facteurs
synthtiques du climat
Dimensions Genre N Moyenne t df
Sig.
(2-tailed)
Masculin 172 26.7733 Climat relationnel
Fminin 155 24.7226
2.653 325 .008
Masculin 159 22.7799 Frustration/ hostilit
Fminin 155 19.6000
3.739 312 .000
Masculin 171 23.5146 Critres de notation
Fminin 155 21.9419
1.980 324 .049
Masculin 138 132.0507 Climat scolaire total
Fminin 144 122.9931
2.804 280 .005
Masculin 147 76.4354 F1- Climat relationnel -
total
Fminin 146 70.4726
2.753 291 .006
Il faut remarquer que ces diffrences sont troitement lies des donnes objectives. Les filles ont
des notes meilleures que les garons pour les mats, la langue roumaine et la moyenne gnrale (et
85
la diffrence est significative au seuil de ,000) c'est--dire les rsultats scolaires qui comptent
pour le futur!
4. Conclusions
Letude permet de diffrencier les climats scolaires dune cole par des enqutes au niveau de la
classe. La sensibilit de loutil a t prouve pour la diffrenciation d'age/ classe et de genre. Le
questionnaire est sensible des diffrences entre les coles, et une investigation au niveau micro
permet le diagnostic des dimensions du climat ainsi que le niveau des variables indiquant un climat
favorable ou dfavorable de l'valuation. On peut ainsi tablir un profile du climat de l'valuation
pour une classe et pour une cole et saisir les vulnrabilits pour pouvoir projeter des
interventions.
Rfrences
4. Ashforth, S. J. (1985). Climate formations: Issues and extensions. Academy of Management
Review, 25, 837-847.
5. Bowers, J. H. & Burkett, C. (1989). Effects of physical and school environment on students
and faculty. The educational facility planner, 27(1), 28-29
6. Brookover, W. B., Schweitzer, J. H., Schneider, J. M., Beady, C. H., Flood, P. K. &
Wisenbaker, J. M. (1978). Elementary school social climate and school achievement. American
Educational Research Journal, 15, 301-318
7. Cocorad, E. Clinciu, A. I., Pavalache-Ilie, M., Luca, M. R. (2008). Instrument de mesure pour
le climat scolaire centre sur levaluation. Le 20e colloque de l'ADMEE-Europe, Evaluation en
tension, 9-11 janvier, Genve, 2008.
8. Coleman, J. S., Campbell E. Q., Hobson, I. J. McPartland, J., Mood, A. M., Weinfeld, F. D. &
York, R. L. (1966). Equality of educational opportunity. Washington, D.C.: U.S. Government
Printing Office.
9. Edmons, R. (1979). Some schools work and more can. Social Policy, 9, 28-32.
10. Freiberg, H. J. (1999). School climate: Measuring, improving and sustaining healthy learning
environment. Philadelphia: Falmer Press.
11. Gentilucci, J. L. & Muto, C. C. (2007). Principals' influence on academic achievement. The
student perspective. NASSP Bulletin, 21, 219-238.
12. Giddens, A. (2000). Sociologie. Bucuresti : Ed.All.
13. Holt, C. R. & Smith, R. M. (2002). The Relationship between school climate and student
success. Arkansas Educational Research & Policy Studies Journal, 2, 52-64.
86
14. Hoy, W. K. & Hannum, J. W. (1997). Middle school climate: An empirical assessment of
organizational health and student achievement. Educational Administration Quarterly, 33(3), 290-
311.
15. Hoy, W. K. & Sweetland, S. R. (2000). School characteristics and educational outcomes:
Toward an organizational model of student achievement in middle schools. Educational
Administration Quarterly, 36, 703-714.
16. Hoy, W. K. (2002). Faculty trust: A key to student achievement. Journal of school public
relations, 23, 88-103.
17. Hoy, W. K., Tarter, C. J. & Hoy, A. W. (2006). Academic optimism of schools: A force for
student achievement. American Educational Research, 43(3), 425-446.
18. Iosifescu, S. (1998). Cultura organizaional a colii romneti. Bucuresti: ISE.
19. Iosifescu, S. (2004). Relaia dintre cultura organizaionala i proiectele de cooperare
internaional. Bucuresti: Agentia Nationala Socrates.
20. Janosz, M., Georges, P. & Parent, S. (1998). L'environnement socioducatif l'cole
secondaire: un modle thorique pour guider l'valuation du milieu. Revue Canadienne de Psycho-
ducation, 27(2), 285-306.
21. Keesor, C. A. (2005). Administrative visibility and its effect on classroom behavior. NASSP
Bulletin, 89(634), 64-73.
22. Miclea, M. (2007). Romnia educaiei, Romnia cercetrii. (Raportul comisiei prezidentiale
pentru analiza si elaborarea politicilor din domeniile educatiei si cercetrii), Bucuresti.
www.edu.ro
23. Miroiu, A. (1998). nvmntul romnesc azi. Studiu de diagnoz. Iasi: Polirom.
24. Mok, M. M. C. & McDonald, R. P. (1994). Quality of school life: A scale to measure student
experience or school climate? Educational and Psychological Measurement, 54, 483-495.
25. Samdal, O., Nutbeam, D., Wold, B. & Kannas, L. (1998). Achieving health and educational
goals through schools - a study of the importance of the school climate and the students'
satisfaction with school. Health Education Research, Vol. 13 (3), 383-397.
26. TIMSS International Study Center, IEA (2000). School Background with Science Achievement-
Main Survey. Chestnut Hill, MA: TIMSS International Study Center, Boston College.
Primit 20.11.2008.
87
Implicaiile bolii asupra autodeterminrii adolescenilor bolnavi de cancer
Elena Losi, conf.univ., dr.n psihologie.
n sufletul fiecruia dintre noi, mai mult sau mai putin constientizate, sunt prezente teama de
suferint, teama de boal, teama de moarte. Perspectiva mortii, mai ales n cazul unei persoane
tinere, este paralizant. n mod firesc, aflarea diagnosticului de cancer provoac emotii precum
tristetea, mnia, teama, frustrarea, sentimentul lipsei de control asupra propriei vieti. Acestea sunt
sentimente umane normale si care odat ce au aprut, caut s se exprime. Tabloul clinic al bolii
oncologice nu rezuma doar din simptoame ce reflect actiunea propriului factor patogen, dar
include si atitudinea vizibil sau ascuns a adolescentului bolnav ctre propria boal. Aceasta ne
permite s spunem c la adolescentii bolnavi de cancer suferinta somatic se combin cu reactia
personalittii.
Etapele reactiilor psihogene se pot deosebi nu doar la bolnavi diferiti, dar si n functie de etapa
contactului cu boala oncologic acelorasi pacienti. Starea psihologic a adolescentului care pentru
prima data aude de la lucrtorii medicali c el, posibil, are o boal oncologic este descris n
lucrrile E.Cobler-Ross. Ea a demonstrat c majoritatea bolnavilor trec prin cinci etape de baz de
reactii psihologice :
1. Negativism sau oc. Persoana nu crede c sufer de o boal cu sfrsit letal. Ea ncepe s se
adreseze la diferiti specialisti, verific rezultatele primite, face analize n clinici diferite. n reactia
de soc nu-l intereseaz nimic si nu se mai adreseaz la nici o clinic.
88
2. Indignare. Se caracterizeaz prin exprimarea reactiilor emotionale, adresat medicilor,
societtii, rudelor si destinului.
3. Comerul este ncercarea de a comercializa ct mai multe zile de trai de la diferite instante. De
exemplu dac voi folosi tinctur de plante voi tri nc trei ani; dac voi tine post si voi merge
regulat la biseric, voi termina liceul cu bine .
4. Depresia. Persoana a nteles gravitatea situatiei sale. El a lsat minile n jos si a ncetat s mai
lupte. Fuge de prietenii lui permanenti. Nu se ocup cu lucrurile care-l interesau mai nainte. Se
nchide singur n cas si si plnge destinul : Iesire din situatie nu exist, lsati-m n pace !.
5. Acceptarea. Este o reactie psihologic mai rational, dar pn la ea nu toti ajung. Bolnavii mor
pna a ajunge la stadiul patru. Da! asta s-a ntmplat cu mine, dar nu este totul pierdut . Trebuie
de luptat chiar dac mai am de trit jumatate de an, sa-l triesc rational pentru mine si pentru cei
care m iubesc.
Adolescentii bolnavi de cancer sufer schimbri de ordin ambiental si rational cu impact
major asupra strii psihice. Adolescentii internati sau retinuti la domiciliu sufer o veritabil
schimbare de decor, ncepnd cu prsirea mediului habitual a ambiantei familiare a locului de
studiu ori a peisajelor din micro- universul lor si nlocuirea acestor repere n timp cu : atmosfera
grav, sever a spitalului, cu lumea lui de oameni n halate albe, nu ntotdeauna atenti la
frmntrile de ordin adaptativ ale celor internati. Pentru cei rmasi n cas, orizontul acestui
mediu, privit ntotdeauna ca plin de cldur si dttor de liniste interioar, devine prea strmt si
apstor n cazul unei sederi prelungite. O situatie special o prezint bolnavii ambulatori care
ncep s perceap cele dou medii fundamentale ale existentei ca pe niste posibile pierderi, n
perspectiva evolutiei nefavorabile a bolii, ei fiind stresati la gndul unor astfel de schimbri ale
modului lor de viat. Modificrile de tip comportamental induse de boal sunt: egocentrismul -
restrngerea orizontului, dependenta, predominanta unor procese emotionale de tipul afectelor de
agresivitatea, anxietatea, depresia. Evident c toate aceste schimbri implic modificri si n
autodeterminarea adolescentilor.
Adolescenta reprezint acea faz a dezvoltrii umane marcat prin diferentiere si
individualizare si care se exprim mai intens dect oricare alt perioad din viat printr-un
comportament proiectiv, mai mult sau mai putin structurat. Descoperirea propriei individualitti,
construirea unor valori personale raportate la sistemul de valori al adultilor, socializarea conduitei
individuale reflect, deseori, nevoia profund a adolescentului de a se integra ntr-o lume care s
corespund aspiratiilor sale. Dup N. Sillamy, functia adolescentei este definit prin capacitatea de
a recunoaste, n desfsurarea tuturor virtualittilor, posibilittile care permit alegerea unei ci spre
vrsta adult si a stabili noi relatii ntre El si Altii. Este vrsta afirmrii intereselor att profesionale
ct si sociale, a dorintei de libertate si autonomie fat de apartintori, ct si printr-o generoas
89
sensibilitate ideo-afectiv; vrst a marilor idealuri, dar si a tririlor dureroase, uneori cu urmri
dezadaptive, care necesit o ntelegere si o ndrumare afectuoas si clar - vztoare n acelasi timp.
Specificul perioadei adolescentine const n faptul c anume n aceasta perioad la individ se
formeaz acele calitti fundamentale, care ulterior perpetueaz toat viata. Evident c viziunea si
conceptia despre lume a individului se schimb pe parcursul vietii, dar anume n adolescent
individul este mai supus influentelor sociale si se transform foarte activ si intr-un termen foarte
scurt. Este temeinic presupunerea c, dac n adolescent individul nu si-a format deprinderi de
autoanaliz, mai trziu acest lucru devine putin probabil. Iar ca rezultat, persoana acord putin
atentie cunoasterii sinelui, si formeaz o imagine distorsionat despre propria persoan si despre
interactiunea sa cu lumea. Cu toate c n psihologie exist diferite abordri a problemei
autodeterminrii totusi comun pentru toate este determinarea factorilor si conditiilor ce
influenteaz procesul de autodeterminare.
n aceast ordine de idei prezint interes modul cum se efectueaz autodeterminarea
personal la adolescentii bolnavi de cancer. Aceasta si ne-a determinat s ntreprindem un studiu
experimental. n procesul de cercetare experimental a autodeterminrii adolescentilor bolnavi de
cancer au fost investigate 2 esantioane de subiecti selectati aliator n numr de 40 cu vrsta
cuprins ntre 16-18 ani, dintre care adolescentii sntosi - 20 subiecti si 20 adolescentii bolnavi
din sectia Oncopediatrie si Hematologie N 2, Spitalul Oncologic. Asupra acestui esantion am
aplicat urmtoarele metode si tehnici: Testul de determinare a autoaprecierii, Dembo-Rubenstein
(n modificarea lui A. M. Prihojan); Autoaprecierea imaginii de sine; Metoda de diagnosticare a
adaptrii socio-psihologice (K. Rogers si R. Daimond), adaptat de Sneghiriova T.V; Testul
ncrederea n sine.
Rezultatele obtinute sunt urmtoarele. Starea snttii afecteaz autoaprecierea si nivelul de
aspiratii a adolescentilor bolnavi de cancer. Subiectii bolnavi de cancer au obtinut urmtoarele
rezultate: E-ul Real -37,40 %- nivel mediu, E-ul Ideal - 83,40% - nivel nalt. Nivelul mediu
obtinut la E-ul Real- 37,40 % la subiectii bolnavi de cancer. Astfel, datele obtinute de
adolescentii sntosi n urma aplicrii metodei Dembo- Rubinstein, denot c ei au atins nivel nalt
si la E-ul Real si la E-ul Ideal. Analiznd aceste date am efectuat analiza procentual a acestora
pe care am reflectat-o n Fig.1
76,05
37,40
94,45
83,40
0,00
10,00
20,00
30,00
40,00
50,00
60,00
70,00
80,00
90,00
100,00
Rubinshtein E/R Rubinshtein E/I
subiecti sanatosi
bolnavi de cancer
90
Fig. 1 Distributia datelor autoaprecierii si aspiratiei sinelui (dup Dembo Rubenstein)
Analiznd rezultatele obtinute n urma aplicrii metodei ncrederea n sine am nregistrat
urmtoarele rezultate: Adolescentii sntosi au obtinut 49,95 %, - nivel nalt, care confer omului
urmtoarele consecinte :
permite luarea n stpnire a propriei persoane;
controleaz comportamentul, ratiunea si elanul;
determin recunoasterea valorii si autorittii personale, care inspir semenilor o atitudine de
respect si pretuire;
acord Eu-lui propriu prestigiu, echilibru psihic si psihosocial.
Adolescentii bolnavi de cancer au obtinut 33,35 % - nivelul ncrederii n sine determin nu
numai randamente sczute, ci si o stare de deprimare, apatie si chiar de suferint. Nencrederea n
sine cunoaste grade variate de manifestare sau de stpnire a Eu-lui, starea snttii afectat se
manifest prin stri de neliniste, pna la stri de ndoial obsesional, nevrotic. Datele analizate
sunt reflectate n Fig. 2
49,95
33,35
0,00
10,00
20,00
30,00
40,00
50,00
Increderea in sine
subiecti sanatosi
bolnavi de cancer
Fig. 2 Distributia datelor privind ncrederea n sine la subiectii sntosi si la cei bolnavi de cancer
Autoaprecierea imaginii de sine la adolescentii bolnavi de cancer, n urma rezultatelor
obtinute au nregistrat un procentaj mic 14,90 %, n comparatie cu 23,50 % la adolescentii
sntosi. Datele sistematizate sunt reflectate n Fig.3
23,50
14,90
0,00
5,00
10,00
15,00
20,00
25,00
Autoaprecierea imaginii de sine
subiecti sanatosi
bolnavi de cancer
Fig. 3 Distributia datelor privind autoaprecierea imaginii de sine la subiectii sntosi si cei
bolnavi de cancer
Aici la fel putem mentiona existenta unui profil sters al imaginii de sine la adolescentii
bolnavi de cancer care probabil rezult din nemultumirea fat de sine si care se datoreaz n cea
mai mare msur strii de sntate.
91
Metoda de diagnosticare a adaptrii socio psihologice elaborat de K. Rogers si R. Daimond,
modificat de Snegheriova T.V, permite cercetarea mecanismelor de adaptare, autoacceptare,
acceptarea si neacceptarea celorlalti, nivelul confortului emotional, control interior, tendinta de a
domina. Cele mai mari valori la bolnavii de cancer s-au obtinut la scala Dezadaptare (123,95),
Discomfort emotional (25,10) si scala Neacceptarea celor din jur (25,15); valori mici s-au obtinut
la urmtoarele scale: Acceptarea sinelui (24,80); Acceptarea celor din jur (17,45); Controlul
exterior si interior (27,55 23,95). Factorii importanti si determinanti ai autodeterminrii
personale sunt autoacceptarea si acceptarea celorlalti. Adolescentii bolnavi nu pun multe ntrebri
precum copii mai mici, ei sunt n stare s nteleag situatia si cauza bolii, dar concomitent pot fi
dominati de disconfort emotional si neacceptarea sa. Pe ei i deranjeaz faptul c colegii lor nu-i
vor primi adecvat deoarece sunt bolnavi. n special i nelinisteste faptul c lipsesc mult de la
scoal sau de exteriorul lor foarte schimbat cderea prului, repede au slbit sau ngrsat. Analiza
rezultatelor obtinute la testul de diagnosticare a adaptrii social psihologice nu permite s facem
urmtoarele concluzii:
Adolescentii bolnavi au un nivel redus al autodeterminrii personale care este n strns
legtura cu insuficienta emotiilor pozitive si nivel redus al confortului emotional.
Autodeterminarea personal devine posibil datorit mecanismelor de comunicare n grup si
acceptarea celorlalti, precum si tendintei de a-si asuma totalmente responsabilitatea pentru
propriile actiuni, succese si insuccese. Pe cnd adolescentii bolnavi de cancer uneori sunt
bucurosi s lase toat responsabilitatea pe cei maturi si nu doresc din timp s cunoasc despre
procedurile care urmeaz.
Rezultatele obtinute ne conduc spre ideea c autodeterminarea adolescentilor este
conditionat de autoapreciere, adaptare si nivelul de respect de sine. Formarea autodeterminrii
personale adecvate a adolescentilor bolnavi de cancer poate fi influentat prin dezvoltarea
autoaprecierii , respectului de sine. Boala afecteaz grav stare psihic a adolescentilor si sprijinul
apropiatilor este crucial. Pe lng o comunicare real si permanent cu sine si cu cei dragi, alte
moduri utile de exprimare a emotiilor negative pot fi ntretinerea unui jurnal, desenul, pictura,
alctuirea de colaje, sculptura, olritul, cititul, rugciunea, meditatia.
Summary
Personal determination is a key problem in personality forming. Teenagers are special
because during this period fundamental qualities for entire life are forming. Cancer makes changes
in self-determination, influence level of self-appreciation, socio-psychological adaptation and level
of self-respect. These are demonstrated in this article, with results obtained from experimental
research performed.
Bibliografie selectiv:
1. Apamona, I. C., Bospacrnax ncnxonornx, Exarepnnypr, 1999
2. Iemeso, M. B., Iepacnmona, B. C., Iopenona, I. I., Opnona, H. M., Bospacrnax
ncnxonornx: or monoocrn o crapocrn, Mocxna, 1999
92
3. Manxnna-Htx, H. I., Bospacrnte xpnsnct, Mocxna, 2004
4. Bnxn, I., Bospacrnte xpnsnct. Crynenn nnunocrnoro pocra, CH, 1999
5. Innsypr M.P. Hnunocrnoe camoonpeenenne xax ncnxonornuecxax nponema /
Bonpoct ncnxonornn, 1988, N2
6. Kon H.C. B noncxax cex, nnunocrt n camocosnanne. M., 1984
7. Ca]nn B. u. Bonpoct camoonpeenenne nnunocrn n ee axrnnnocrn. V]a, 1985
8. Peannnrannx onxonornuecxoro ontnoro /Ho pe. H. H. Hananxona. H.:
Henynpnsar, 1979. C. 6263, 7273.
9. Pyxonocrno no mennnne. narnocrnxa n repannx: B 2 r. / Hep. c anrn.; Ho pe.
P. Fepxoy, 3. uneruepa. T. 2., M.: Mnp, 1997. C. 37; 6166, 7376.
10. Pyxonocrno no npo]nnaxrnuecxo mennnne. Pexomenannn no ncnxnuecxo nomomn
onxoontntm / Hep. c anrn. H. B. Henanoncxoro. M.: Mennnna, 1995. C. 4955.
11. Camonron K., Camonron C. Hcnxorepannx paxa. Canxr-Herepypr: Hnrep, 2001
288 c.
12. emnn, B.H.Conepmencrnonanne meroon peannnrannn onxonornuecxnx ontntx. -
H., 1978. - C.30-31.
13. Amnpacnanon A.T. n p. Peannnrannx onxonornuecxnx ontntx. M.: Mennnna.
1988. 272 c.
Primit 25.11.2008
Premisele teoretice ale abordrii jocului ca modalitate de nvare i educare
Monica Tnsoiu, Romnia, doctorand UPS Ion Creang
Forma de manifestare cea mai important a copilului este jocul. Lucian Blaga afirma pe
bun dreptate si cu mult inspiratie c ntelepciunea si iubirea copilului este jocul.
Jocul este o actiune specific, ncadrat n sensuri si tensiuni, ntotdeauna desfsurat dup
reguli acceptate de bunvoie si n afara sferei utilittii sau necesittii materiale, nsotite de
simtminte de nltare si de ncordare, de voiosie si destindere. Jocul ca modalitate de relatie ntre
eu (subiect) si lumea obiectelor reprezint formula primar a actiunii umane, el este una din
activittile prin care copilul nvat s cunoasc lumea real.
Modul n care a fost si este nteles jocul prezint, n general, anumite particularitti la
diferite popoare si n diferite timpuri. Astfel la vechii greci, cuvntul ,,joc desemna actiuni proprii
copiilor, exprimnd, n principal, ceva ce noi spunem acum ,,a face copilrii. La evrei, cuvntul
,,joc corespunde notiunii de glum si haz. La romani, ,,ludo desemna veselia, plcerea. n limba
sanscrit, ,,haleada nseamn bucurie.
Ulterior, n toate limbile europene, semnificatia cuvntului ,,joc a nceput s se extind
asupra unor largi sfere de actiuni umane, care pe de o parte nu presupun o munc grea, iar pe de
alt parte, ofer oamenilor veselie si satisfactie (Elkonin, 1980).
Dac nu ne-am juca, realitatea ar fi mai greu de suportat. Pentru c, nu doar copiii se joac,
ci toti oamenii, chiar si animalele! Putem juca asa cum vrem noi o situatie, putem stabili regulile
93
jocului, l putem opri atunci cnd dorim. ,,Piua ! este cuvntul magic, care opreste jocul. Jocul
produce satisfactie prin el nsusi si nu prin rezultatele lui (Chateau, 1985).
Jocul, departe de a fi o simpl actiune gratuit, distractiv, recreativ, menit s tempereze
excesul de energie, caracteriznd biologia infantil, reprezint, n esent, o treab ct se poate de
serioas. Psihologii au stabilit c jocul scoate la suprafat aptitudini si vocatii de tot felul (Piaget &
Inhelder, 2005).
Copiii de pe toate meridianele lumii se joac, n linii mari, cam la fel. Expresia ,,hai s ne
jucm reprezint, astfel, sloganul universal si obsedant al copilriei.
n literatura de specialitate se poart numeroase discutii contradictorii privind esenta
psihologic a jocului, dat fiind faptul c au aprut numeroase teorii ce ncearc s se explice jocul
si functiile sale n viata noastr de la nceput pn la sfrsitul ei.
n continuare ne vom referi la cele mai reprezentative teorii ale jocului si vom stabili
impactul lor asupra dezvoltrii cunoasterii stiintifice a jocului ca activitate concret, vie si care
corespunde primei etape a procesului de cunoastere, caracterizat prin instruirea lumii pe calea
simturilor, mijlocind cunoasterea direct a lumii, activnd deprinderi, trsturi complexe de
caracter, convingeri si puternice trsturi morale (Bruner, 1983).
Teoriile despre joc, n esenta lor, au pus n evident un aspect sau altul, fr a releva
preponderent implicatiile intelectuale, fr a considera jocul ca o actiune de cunoastere, de
organizare a cunoasterii.
Toate aceste teorii au abordat jocul din diverse perspective psihopedagogice, considernd
jocul ca o activitate autotelic opus muncii (J.M.Baldwin), ca o activitate care nsuseste si
absoarbe surplusul de energie al copilului (Herbert Spencer), ca o reproducere a unor actiuni
inutile n prezent, dar care n istoria umanittii erau considerate drept munc (Stanley Hall), ca o
activitate autotelic ce pregteste copilul pentru munc (Karl Gross), ca un mijloc de realizare de
sine (Eduard Claparde), ca o activitate care declanseaz si exerseaz o functie oarecare fr un
scop intentionat (Ch. Buhler), ca un instrument de formare si autoafirmare a eu-lui (Jean Chateau)
etc.
H. Wallon (1975) afirma c dac aceste teorii nu dau o explicatie satisfctoare jocului, nu
este din cauza contradictiilor, ci din cauza premiselor contestabile, a sistematizrilor prea
fragmentate care decurg din aceste teorii
Unii psihologi, ca de exemplu P.P. Blonski, considerau c nici nu se poate vorbi de o teorie
a jocului, atta vreme ct termenul de ,,joc este folosit pentru variate genuri de activitate (jocuri
de fictiune, de constructie, imitatie, dramatizare). Plecnd de la aceast premis, el propune chiar
renuntarea la termenul de ,,joc si nlocuirea lui cu cel de art a constructiei sau a dramatizrii
(Blonski, 1979).
94
Raportul dintre joc si nvtare constituie o problem abordat n contradictoriu, unde sunt
opinii care pur si simplu exclud jocul din contextul nvtrii sau consider c jocul si educatia se
exclud reciproc, fiind dou actiuni, functional si structural, autonome, fiecare cu specificul su.
Pe pozitii diametral opuse se situeaz opiniile clasicilor psihopedagogiei speciale (J.Itard,
E. Seguin, O. Decroly, M. Montessori), ale psihanalistilor A. Freud, M. Mannoni, ale psihologilor
E. Claparde, J. Piaget, J. Brunner, A.N. Leontiev, H. Wallon si a.
Clasicii psihopedagogiei speciale au acordat jocului un rol central n procesul educational-
terapeutic, un simptom discriminativ n prezentarea diagnosticului. Ed. Seguin afirma c idiotul
care se joac nu mai este idiot si c idiotul care se joac merit un alt nume.
Eduard Claparde este de prere c jocul reprezint o adevrat munc pentru copil, fiind
un mijloc cu ajutorul cruia el si poate dezvolta eu-l su, adic personalitatea. Claparde a
elaborat si a descris un ntreg sistem psiho-genetic cu trei stadii: 1) stadiul de achizitie si
experimentare; 2) stadiul de organizare si evaluare; 3) stadiul de productie si munc (Claparde,
1946).
A.N. Leontiev defineste jocul ca o activitate fundamental ce are un rol hotrtor n evolutia
copilului ce const n reflectarea si reproducerea vietii reale. Este o activitate biopsihosocial
avnd originea legat de resorturile biologice. Jocul si are originea, n conceptia lui Leontiev, n
decalajul care exist ntre cerintele puse n fata copilului fat de mediul si posibilittile de care
dispune pentru a rspunde acestora (Leontiev, 1964).
n teoria atavismului jocurile se nftiseaz ca fiind reflectarea unei nsusiri mostenite,
copilul fiind considerat o recapitulare a filogeniei.
Teoria catartic se ntemeiaz pe ideea c jocul constituie un mijloc de nnobilare a unor
instincte nnscute. Prin jocurile de fictiune, de achizitie, de constructie copilul va anticipa
viitoarea sa viat de adult, folosind mijloacele de care dispune si n limitele impuse de mediu.
Jocurile copiilor si, ulterior, ale adultilor contribuie la formarea si dezvoltarea personalittii. Jocul
nu exclude efortul, oboseala, caracterul serios. Un copil care nu se joac nu este un copil normal,
iar viata sa ulterioar, de adult, va avea de suferit. Dimpotriv a folosi jocul, adaptat formelor sale
exterioare la scopuri educative precise, nseamn a canaliza n scopuri benefice una din energiile
cele mai mari si profunde ale copilriei.
Activitatea ludic constituie o bun parte, dac nu totalitatea activittii diurne a copilului.
Jocul reprezint o fort puternic, o form spontan de pregtire pentru viata matur si fixeaz
multe achizitii pe care le creeaz. El este, astfel, folosit ca un factor educativ, iar utilizarea jocului
n scopuri educative o fcea nc Platon n celebra sa academie. Ulterior, educatia bazat pe joc va
fi sustinut de Viltorino De Feltre, de Rabelais, Fenelon, Basedow. n epoca contemporan, jocul
95
este pus sistematic n serviciul scolii nu numai ca mijloc de practicare a exercitiilor fizice, dar si
pentru educatie intelectual si instructia propriu-zis.
Din teoria piagetian retinem coordonata genetic a actiunii ludice. Jocul se constituie ca
un schimb simpatic cu obiectul, persoana sau situatia chiar n primele luni de existent, actiunea
ludic fiind considerat ca o actiune primar. Aparitia extrem de timpurie si n conexiune cu
structura afectiv face ca actiunea ludic s contribuie fundamental la structurarea eu-lui afectiv,
motivational, cognitiv si social (Piaget & Inhelder, 2005).
J. Piaget sublinia c functia esential a tuturor formelor de joc este aceea c, ,,transform
realul printr-o asimilare mai mult sau mai putin supus la trebuintele eu-lui. Astfel jocul este
considerat ca o activitate de asimilare, care functioneaz pentru ea nssi, nensotit ns de un
efort de acomodare (Piaget, 2008).
Primul dintre efectele jocului este cel de transformare a realittii pe baza unei actiuni
specifice si complexe, care antreneaz structurile fundamentale ale persoanei. Aceast operatie de
transformare duce la o asimilare a realului de ctre subiect, iar aceast asimilare este organizat de
ctre joc. Jocul apare ca o actiune organizat cu scopul asimilator-integrator.
A doua coordonat a teoriei piagetiene despre joc este diversitatea actiunii ludice ca o
consecint direct a sensurilor genetice ale jocului. Triada ludic piagetian: jocul-exercitiu, jocul-
simbolic si jocul-cu reguli, este structurat pe scara evolutiv a inteligentei, fiecare tip de joc
reprezentnd o anumit etap de dezvoltare.
Principalul mesaj ce-l degaj teoria piagetian[ asupra jocului este ca viata social reprezint
o conditie necesar dezvoltrii individului n nssi natura sa, fcndu-l s treac de la starea
autist la starea de personalitate. El vede cooperarea ca un proces generator de ratiune desi
diferentele dintre indivizi au legtur cu ereditatea biologic n sensul c niciodat nu a putut ridica
gradul de inteligent al unui individ marcat de debilitate. Piaget atribuie o functie important
coordonrilor si reglrilor sociale preciznd c inteligenta uman se dezvolt la individ n functie
de interactiunile sociale, n general prea neglijate (Piaget & Inhelder, 2005, Piaget, 2008).
Perspectiva piagetian poate fi caracterizat prin trei trsturi dominante: 1) dimensiunea
biologic, 2) interactionismul factorilor subiect-mediu, 3) constructivismul psiho-genetic.
Piaget calific epistemologia sa genetic drept naturalist, fr a fi pozitivist si
consider conduitele cognitive ca un produs al unui organism nzestrat cu structuri ce se manifest
prin puterea de asimilare si acomodare.
Constructivismul psiho-genetic consider secventele dezvoltrii ca fiind reglate de niste
mecanisme de echilibrare de origine endogen, dar fr a fi predeterminate de factorii ereditrii n
ceea ce priveste continutul sau finalizarea structurilor de echilibrare.
96
Teoria genetic a pus n lumin un factor cruia anumite conceptii despre nvtare nu-i
acordaser nicio atentie, acela al mecanismelor de auto-reglare sau de echilibrare.
Reprosul fundamental adus conceptiei psiho-genetice si sistemul stadial al lui Piaget,
dincolo de varietatea formulrii, pare a fi aceasta: ncrederea prea mare n natura uman pe fondul
unei indiferente vizibile fat de puterea educatiei.
Pe lng psihologia genetic piagetian, trebuie s lum n considerare si o a doua mare
teorie contemporan si anume: taxonomia lui B.S. Bloom.
Placnd de la obiectivele stabilite de taxonomia lui B.S. Bloom si a obiectivelor stabilite de
R. Dogbeh si de Diaye pentru jocuri, cercettorii din cadrul UNESCO au stabilit corelatia dintre
acestea sintetizndu-le n urmtoarele obiective:
1. Nivelul de cunostinte simple: ntiprirea si retinerea informatiilor;
2. Nivelul de ntelegere: transpunerea unei forme de limbaj n altul, interpretarea datelor,
explorarea lor.
3. Nivelul de aplicatie: capacitatea de a aplica principiile, regulile n situatii noi.
4. Nivelul de analiz: a analiza un ansamblu complex de elemente, de relatii sau principii.
5. Nivelul de sintez: structura (rezumatul, planul, schema) elementelor provenite din
surse diferite.
6. Nivelul de inventie, de creatie: transferul achizitiilor n operatii creatoare (Bloom &
Krathwohr,1970).
Dup cercettorii amintiti jocul rspunde la aceste obiective din considerentele c diversele
categorii de jocuri valorific:
1. Toate activittile perceptive: contactul senzorial cu obiectele;
2. Activitti senzorio-motorii: alergatul, sritura n nltime, lungime, aruncarea;
3. Activitti verbale; de la antrenamentul verbal pn la comunicarea prin cuvinte,
propozitii, fraze;
4. Domeniile afective: atragerea, repulsia, identificarea, reprezentarea diferitelor roluri si
statute familiale, scolare si sociale.
5. Domeniile intelectuale: observatia, descrierea, compararea, clasificarea, adic procesele
de rationament corect bazate pe date concrete.
6. Activitti de constructie care mobilizeaz energia fizic, capacittile intelectuale si
afective.
7. Activittile de expresie corporal si estetic: gimnastica, dansul, teatrul, muzica,
modelajul, decupajul, colajul, desenul.
Indiferent de genul de joc se pot ndeplini obiectivele operationale din paradigma lui Bloom
si cea a lui Piaget care stabileste c o anumit categorie de jocuri corespunde unei anumite etape de
97
dezvoltare, cu o succesiune temporal, iar structurile superioare se intersecteaz cu cele
precedente, fr a le suprima, important fiind depsirea etapei si nu vrsta cronologic la care se
ajunge la o anumit etap de dezvoltare.
Marele geniu al psihologiei L. Vigotski n lucrarea Preistoria limbajului scris preciza c
pentru copil, n joc, unele obiecte semnific cu usurint alte obiecte pe care le nlocuiesc devenind
semnele lor. Se stie de asemenea c similitudinea dintre jucrie si obiectul pe care l reprezint nu
are important; important este numai utilizarea ei functional, posibilitatea de a realiza cu ajutorul
ei gestul imaginat (Vgotski, 1972).
Teoreticienii postmodernisti ai educatiei au preluat din opera lui Vigotski ideea simulrii
cognitive prin intermediul relatiilor dintre copii, tineri si adulti, relatii menite s ofere oportunitti
pentru scopul de a avea contact direct cu oamenii si procesele din mediul lor.
O abordare extrem de interesant si original a jocului infantil o ofer un alt compatriot al
lui Vgotski M.I. Basov (1975). El a acreditat ideea conform creia originalitatea procesului de joc
se sprijin pe particularittile interrelatiei dintre individ si mediu, interrelatie pe solul cruia apare.
Aceast tez transfer centrul de greutate al problemei de la individ la conditiile obiective ale
existentei sale.
Analiza a demonstrat c de-a lungul perioadei prescolare-scolare mici de dezvoltare se
produc mutatii esentiale n caracterul stimulrii proceselor de joc, ct si n caracterul organizrii
sau al formelor structurale.
Lui M.I. Basov i apartine introducerea n psihologie a notiunii de tip general de activitate,
ce caracterizeaz atitudinea copilului si faptul c renunt la teoriile pur naturaliste despre joc care
plasau izvoarele acestuia n interiorul individului si nu n sistemul de relatii dintre copil si mediul
nconjurtor (Basov, 1975).
Dezvoltarea activittii ca joc este strns legat de ntregul curs al dezvoltrii copilului.
Despre aparitia jocului se poate vorbi numai dup formarea principalelor coordonri
senzoriomotorii ce creeaz posibilitatea manipulrii, a operrii cu obiectele. Fr deprinderea de a
o tine obiectul n mn, nu este posibil nici o operatie cu el si, deci, nicio operatie de joc.
Prima jumtate a primului an de viat revine formrii sistemelor senzoriale.
Jocul cu roluri apare la hotarul dintre prima copilrie si vrst prescolar, se dezvolt intens
si atinge un nivel superior n a doua jumtate a vrstei prescolare.
Jocul, structura lui cunoaste mari transformri: de la jocurile fr subiect, compuse dintr-un
sir de episoade adesea nelegate ntre ele, ajungndu-se n cazul copiilor de 3-4 ani, la jocurile cu un
subiect determinat si cu o desfsurare din ce n ce mai complex si mai sistematic.
98
n practica scolar putem constata jocuri folosite la citire, scriere, matematic, dezvoltarea
vorbirii, cunoasterea mediului, desen, muzic, educatie fizic (Banceanu, 2006, Enache &
Munteanu, 1998).
Contributia jocului didactic pentru stimularea si dezvoltarea capacittilor cognitive ale
scolarului mic, ndeosebi a creativittii gndirii lui, la educarea nsusirilor de personalitate ale
acestuia si la nfptuirea obiectivelor de cunoastere ale procesului de predare-nvtare, este
evident.
Jocul didactic rmne pentru scolarul mic forma permanent a procesului de nvtare
(Banceanu, 2006).
Prin jocul didactic elevul si angajeaz ntregul potential psihic, si ascute observatia, si
cultiv imaginatia, inventivitatea, flexibilitatea gndirii, si dezvolt spiritul de cooperare, de
echip.
Prin folosirea jocului ca form de organizare si ca metod, activitatea didactic devine mai
plcut, elevii asimileaz cunostintele mai temeinic (Enache & Munteanu, 1998).
n clasa I, jocul didactic se poate organiza cu succes la toate disciplinele scolare, n orice
moment al lectiei, ntr-o anumit etap a ei, sau ntreaga activitate se poate desfsura pe baza lui,
urmrindu-se fie dobndirea noilor cunostinte, priceperi si deprinderi, fie fixarea si consolidarea
acestora, fie verificarea si aprecierea nivelului de pregtire a elevilor cu conditia ca n cadrul lui s
primeze obiectivele instructiv-educative.
Jocurile didactice sunt mijloace active de nvtare, iar prin crearea unor situatii probleme,
ele dezvolt la scolarii mici spiritul de observatie, de analiz, de judecat, nltur monotonia si
rutina, stereotipia, antreneaz elevii s ia atitudini, s-si corecteze colegii, oferind prilejul de a afla
mai usor cum gndesc elevii mici.
Merit s amintim c, pe lng functia instructiv-formativ, jocurile didactice au si o
functie terapeutic. Folosirea jocurilor didactice n toat varietatea lor, constituie prima etap n
realizarea nvtmntului formativ (Enache & Munteanu, 1998).
Prin joc, se dobndeste un admirabil mijloc de nvtare, deoarece scolarul mic este n rolul
de actor si nu de spectator, el se gseste n angrenajul a ceea ce nvat, nu n afar, fapt ce i
prilejuieste o nvtare de calitate (Banceanu, 2006).
Psihologii romni, printre care si Ursula Schiopu, au clasificat jocurile n 1) jocuri de
creatie si 2) jocuri cu reguli.
Jocurile de creatie se pot desfsura ca o creatie cu materiale si obiecte (culori, nisip,
plasticon), fie ca o creatie prin rol, adic jocurile cu subiecte alese din viata cotidian sau din
povesti.
99
Jocurile cu reguli sunt cele de miscare, sportive sau de antrenare a gndirii, atentiei,
memoriei (Schiopu & Verza, 1981).
Tranzitia de la vrsta prescolar la cea scolar, n esent, nseamn tranzitia de la activitatea
de joc, de la jocul simplu fr reguli, la jocul didactic si implicit la activitatea de nvtare ca
activitate dominant.
Studiile contemporane sunt centrate pe implicatiile intelectuale, jocul fiind o actiune de
cunoastere, de organizare a cunoasterii. n aceast viziune, orice situatie de joc trebuie
transformat ntr-o situatie de nvtare, a unor modele cognitive, comportamentale sau de alt
natur (Banceanu, 2006, Enache & Munteanu, 1998).
Noua viziune a jocului nvtare are repercusiuni asupra ntregii metodologii de nvtare,
cu implicatii directe n dispunerea piramidal a principalelor metode de nvtare destinate elevului
mic si obisnuirea acestuia cu scoala ntr-un mod progresiv.
Summary
The most important form of childrens manifestation is the play. Lucian Blaga states
inspirationally that the play is the childs wisdom and love.
The goal set by the author in this article refers to the analysis of the psychological theories
that try to explain the play and its functions in our life from its beginning until the end. Atavistic
theories present the play as a reflection of an inherited trait, the child being a recapitulation of
the phylogeny. Cathartic theories are based on the idea that the play is a means of elevation of
some innate instincts.
The conclusion the author subscribes to is that the child who does not play is not normal
and their subsequent adult life will be severely prejudiced. Using play by ingeniously adapting
them to accurate educational goals means to beneficially canalize one of the most profound
energies of the childhood. This is the main research problem launched in this paper.
BIBLIOGRAFIE
Banceanu, T. (2006). Jocul didactic-- mijloc de evideniere si stimulare a capacitii
creatoare n nvarea matematicii. Invtmnt primar, Nr. 3.
Basov, M. Ya. (1975). Izbrannye psihologiceskie proizvedenia. Moskva.
Blonski, P.P. (1979). Izbranne pedagogiceskie i psihologiceskie proizvedenia. Moskva:
Pedagogika.
Bloom, B. & Krathwohr, D.R. (1970). Taxonomie des objectifs pdagogiques: domain
affectif. Montreal: Ed. Education Nouvelle.
Bruner, J. (1983). Le dveloppement de lenfant: savoir faire, savoir dire. Paris: P.U.F.
Chateau, J. (1985). Copilul i jocul. Bucuresti: Editura Didactic si Pedagogic.
100
Claparde, Ed. (1946). Psychologie de l'enfant et pdagogie exprimentale. Paris:
Delachaux et Niestl.
Elkonin, D.B. (1980). Psihologia jocului. Bucuresti: Editura Didactic si Pedagogic.
Enache, M. & Munteanu,M. (1998). Jocuri didactice. Galati: Editura PortoFranco.
Leontiev, A. N. (1964). Probleme ale dezvoltrii psihicului. Bucureti: Editura
Stiintific.
Piaget, J. (2008). Psihologia inteligenei. Chisinu: Cartier.
Piaget, J. & Inhelder, B. (2005). Psihologia copilului. Chisinu: Cartier.
Schiopu, U. & Verza, E. (1981). Psihologia vrstelor. Bucuresti: Editura Didactic si
Pedagogic.
Vgotski, L. S. (1972). Opere psihologice, vol. I-II. Bucuresti: Editura Didactic si
Pedagogic.
Wallon, H. (1975). Evoluia psihologic a copilului. Bucuresti: Editura Didactic si
Pedagogic.
Primit 25.11.2008
Diferenele gender n manifestarea agresivitii.
S. Sanduleac, doctorand, UPS I.Creang
Studiile diferentei de gen sunt actualmente n vizorul cercettorilor din mai multe domenii:
ncepnd cu literatura feminist si pn la cele mai recente publicatii academice. n literatura de
specialitate se pun mai frecvent n discutie temele ce tin de influenta rolurilor sociale si a
normativittii a schemelor cognitive si a stereotipului de gen: (R. D. Ashmore S. Basov S.
Bem V. J. Binion Sh. Burn L. L. Carli A. H. Eagli J. A.Hall C. L. Martin D. Myers J. M.
ONeil etc). n ultimii ani problematica genurilor a cptat popularitate si n spatiul postsocialist.
n psihologia rus pot fi mentionate cercetrile realizate de J. Jerebkina E. P. Iliin I. S. Kletina
I. N. Kon L. N. Ojigova P. V. Rumeanteva O. A. Voronina etc.
Problema diferentelor de gen a existat permanent, dar cel mai acut acest fapt s-a resimtit la
sfrsitul secolului XX cnd au nceput a se forma organizatii feministe orientate spre emancipare
si drepturi egale. Acest fapt a servit drept impuls spre noi cercetri n domeniul psihologiei
genurilor.
Odat cu aparitia boomului dezbaterilor pe tema diferentelor de gen s-au ntetit cazurile de
manifestri agresive n trile occidentale, ce a condus la fel spre cercetri n domeniul
agresivittii.
101
Agresivitatea ct si diferentele de gen sunt domenii destul de actuale, care sunt studiate
minutios, dar totusi nu pn la capt. Agresivitatea att n rndul tinerilor ct si n rndul celor
adulti provoac mari probleme. Tot odat exist un stereotip uman ca agresivitatea este
caracteristic mai mult brbatilor si n favoarea acestui argument se aduc numeroase dovezi care
sunt expuse n cercetrile lui Maccoby, Jacklin, 1978. Cercetrile anterioare inter culturale
efectuate au artat c stereotipurile de gen servesc drept factor social ce influenteaz
agresivitatea, stereotipurile de gen servesc drept surs de dezvoltare si ntretinere a agresivittii
la brbati.
Recent a fost realizat un studiu care a demonstrat faptul c a stereotipurile de gen sufer o
schimbare si c femeile sunt la fel de agresive ca si brbatii, ba chiar pot fi mai agresive dect
brbatii, doar c agresivitatea femeilor se deosebeste prin continut si form de cea a brbatilor,
adic preia forme latente, camuflate sau alte dect cea direct pe care o manifest brbatii si are
alt continut.
Studiul efectuat Diferente de gen n manifestarea agresivittii s-a desfsurat pe parcursul
anilor 2007-2008, cuprinznd 3 etape. n timpul primei etape, a fost analizat, generalizat si
sistematizat literatura stiintific privind problema abordat n cercetare, a fost selectat
inventarul psihodiagnostic. La a doua etap, au fost selectati subiectii pentru experimentul de
constatare; a fost efectuat experimentul la care au participat subiecti de la Scoala medie de
cultur general nr. 84 din municipiul Chisinu, UPS Ion Creang, Liceul Sportiv.
n cercetarea experimental au fost aplicate testul la personalitate FPI si testul Bass-Darky.
Rezultatele au fost prelucrate n modul urmtor:
S-a efectuat corelatia ntre variabila independent agresivitate si variabilele dependente
pentru a vedea veridicitatea testelor efectuate si pentru a vedea dac exist relatie ntre
variabilele dependente.
Pentru a fi siguri de rezultatele obtinute s-a efectuat o diagram scatter (norul de puncte)
care a confirmat veridicitatea corelatiei efectuate.
n conformitate cu scopul cercetrii au fost calculate diferentele ntre variabila independent
si variabilele dependente cu ajutorul testului T-student pentru esantioane independente care este
utilizat pentru a calcula dac mediile pentru dou seturi de variabile sunt diferite semnificativ
una fat de cealalt. Rezultatele obtinute au permis evidentierea posibilelor cauze ale agresivittii
feminine si conturarea a dou profiluri ale agresivittii feminine si masculine.
n cea de a doua succesiune experimental s-au ales doi subiecti de gen feminin a cror
agresivitate depsea limitele normalului conform testelor efectuate, dar care aveau situatii sociale
diferite. S-au implementat dou studii de caz n baza observaiilor efectuate timp de un an scolar,
102
asupra acestor subiecti, si interviurilor aprofundate ce au fost nregistrate cu ajutorul mijloacelor
video.
Esantionul experimental a fost constituit din doua sute de subiecti 50% din respondenti au
fost de gen masculin si au constituit primul lot experimental si 50% de gen feminin ce au
constituit al doilea lot experimental. Subiectii au fost selectati n mod stratificat n functie de gen,
nu s-a tinut cont de apartenenta social, reusita scolar, incidenta comportamentelor deviante.
Vrsta medie a subiectilor a fost de 20 ani.
Statistica Descriptiv
200 42.81 9.561 -.472 .172
200 6.63 2.184 -.877 .172
200
Nivelul agresivitatii
generale din inventarul
ostilitatii de Bass-Darky
Agresivitate spontana FPI
Valid N (listwise)
Statistic Statistic Statistic Statistic Std. Error
N Mean
Std.
Deviation
Skewness
n tabelul de mai sus este prezentat corelatia dintre variabilele independente din testul Buss-
Darky si testul FPI care s-a efectuat pentru a verifica validitatea rezultatelor testelor si care a
artat ct de veridice si stabile sunt testele care au fost efectuate. La variabila agresivitate
general din testul Bass Darky s-a obtinut un coeficient de asimetrie (-0,472) cu eroarea
standard (0,172), la variabila agresivitate spontan din testul FPI s-a obtinut un coeficient de
asimetrie
(-0,877) cu eroarea standard (0,172). Rezultatele analizei descriptive a datelor pot fi privite n
tabelul de mai jos.
1 .328**
.000
200 200
.328** 1
.000
200 200
Pearson
Correlation
Sig. (2-tailed)
N
Pearson
Correlation
Sig. (2-tailed)
N
Nivelul agresivitatii
generale din inventarul
ostilitatii de Bass-Darky
Agresivitate spontana
FPI
Nivelul
agresivitatii
generale din
inventarul
ostilitatii de
Bass-Darky
Agresivitate
spontana FPI
Corelatia este semnificativ la pragul (p 0.01) (2-tailed bivariat).
**.
n urma analizei corelationale a variabilelor agresivitate general si agresivitate spontan s-a
obtinut un coeficient de corelatie n valoare de (r=0,328) la un prag de semnificatie (p=0,01).
Ceea ce a permis constatarea unei legturi de trie medie ntre variabilele agresivitate general si
agresivitate spontan. Valorile relatiei pot fi privite n tabelul de mai jos. Trebuie de mentionat
c s-a efectuat diagrama scatter ce a confirmat nc odat veridicitatea rezultatelor obtinute.
103
Testul T student a scos n evident urmtoarele rezultate, n tabelul de mai jos au fost
prezentate doar diferentele semnificative si variabilele ce au prezentat interes deosebit pentru
argumentarea ipotezei de cercetare.
Testul Levene pentru
egalitatea variantelor T-test pentru egalitatea Mediilor
F Sig. t
df (grade
de
libertate)
Diferenta
mediilor
Ostilitate verbala
subscala de la inventarul
ostilitatii de Bass-Darky
Variante egale
5,723 0,018 0,361
198
0,130
Variante inegale
0,361 0,590 0,130
Iritabilitate subscala de
la inventarul ostilitatii de
Bass-Darky
Variante egale
0,393 0,532 -2,456 0,590 -0,820
Variante inegale
-2,456 1,050 -0,820
Sentimentul de vina
subscala din inventarul
ostilitatii de Bass-Darky
Variante egale
0,522 0,471 -1,413 1,050 -0,380
Variante inegale
-1,413 0,130 -0,380
Cota agresivitatii Variante egale
18,580 0,000 -1,792 0,130 -1,874
Variante inegale
-1,792 -0,330 -1,874
Cota ostilitatii Variante egale
7,284 0,008 -7,208 -0,330 -4,360
Variante inegale
-7,208 0,120 -4,360
Nivelul agresivitatii
generale din inventarul
ostilitatii de Bass-Darky
Variante egale
11,283 0,001 -1,997 0,120 -2,680
Variante inegale
-1,997 -0,820 -2,680
Masculinitate-Feminitate
FPI
Variante egale
6,160 0,014 1,623 -0,820 0,510
Variante inegale
1,623 -1,000 0,510
Deci analiza statistic realizat a permis identificarea unor diferente semnificative la
variabilele atentat, iritabilitate, suspiciune, resentiment, cota ostilitii, nivelul agresivitii
generale la cele dou grupe de subiecti, sau altfel spus subiectii de gen masculin sunt tentati mai
mult s aplice forta fizic dect subiectii de gen feminin t(198) =3,85 pentru (p_ 0,001).
Subiectii din primul lot experimental sunt mai putin iritabili, nu manifest nemultumiri
acute, nu explodeaz la orice moment si sunt mai putin suspiciosi, nu proiecteaz ostilitatea
supra altor persoane n comparatie cu cei din lotul experimental numrul doi . De asemeni s-a
104
constatat c subiectii din primul grup experimental, fapt de asemeni relevat de sensul diferentei
t(198)=3,38 pentru (p=0,001).
Subiectii de gen masculin din primul lot experimental s-au dovedit a fi mai putin supusi
sentimentului de suprare sau necjiti fat de lume t(198)=5,00 pentru (p=0,001).
Subiectii din al doilea lot experimental sau dovedit a fi mai ostili dup cum ne arat
rezultatele t(198)=7,20 pentru (p=0,001).
Nivelul agresivittii n general la subiectii de gen masculin este mai mic dect la subiectii de gen
feminin t(198)=1,99 pentru (p=0,04).
n histograma de mai jos sun prezentate diferentele privind agresivitatea dintre primul si al
doilea lot experimental. Studiul realizat ne-a permis s ne convingem de faptul c subiectii din al
doilea lot experimental sunt la fel de agresivi si chiar exceleaz n unele forme ale agresivittii n
comparatie cu subiectii din primul lot experimental.
Concluzia la care s-a ajuns e c exist diferente semnificative la variabilele atentat,
iritabilitate, suspiciune, resentiment, cota ostilittii, nivelul agresivittii generale la cele dou
grupe de subiecti, sau altfel spus subiectii de gen masculin sunt tentati mai mult s aplice forta
fizic dect subiectii de gen feminin. Subiectii din lotul experimental numrul doi au demonstrat
mai mult ostilitate.
5.57
6.62
8.33
8.46
5.53
5.2
3.16
3.28
6.7
5.88
6.64
5.64
5.58
4.34
6.98
6.6
15.04
13.17
11.87
7.51
6.71
6.54
7.27
7.37
44.15
41.47
A
t
e
n
t
a
t
O
s
t
i
l
i
t
a
t
e
i
n
d
i
r
e
c
t
O
s
t
i
l
i
t
a
t
e
v
e
r
b
a
l
N
e
g
a
t
i
v
i
s
m
I
r
i
t
a
b
i
l
i
t
a
t
e
S
u
s
p
i
c
i
u
n
e
R
e
s
e
n
t
i
m
e
n
t
S
e
n
t
i
m
e
n
t
u
l
d
e
v
i
n
C
o
t
a
a
g
r
e
s
i
v
i
t
i
i
C
o
t
a
o
s
t
i
l
i
t
i
i
A
g
r
e
s
i
v
i
t
a
t
e
s
p
o
n
t
a
n
A
g
r
e
s
i
v
i
t
a
t
e
r
e
a
c
t
i
v
(
D
o
m
i
n
a
r
e
)
N
i
v
e
l
u
l
a
g
r
e
s
i
v
i
t
a
i
i
g
e
n
e
r
a
l
e
Manifestri ale agresivitii
Diferene privind agresivitatea feminin i cea masculin
feminin
masculin
Figura nr. 1. Diferente privind agresivitatea feminin si cea masculin
Cei din primul lot experimental s-au dovedit a fi mai putin iritabili, mai putin suspiciosi nu
manifest nemultumiri acute, nu explodeaz la orice moment, proiecteaz ostilitatea supra altor
105
persoane n comparatie cu lotul al doilea. Tot primul lot s-a dovedit a fi mai putin supus
sentimentului de suprare, necjiti fat de lume. Acest lucru prezint o demonstratie direct c
brbatii sunt mai putin agresivi dect femeile. Agresivitatea este caracteristic ambelor genuri si
dup cum arat rezultatele cercetrii, n unele manifestri exceleaz brbatii, n altele femeile, nu
putem trece ns cu vederea faptul c totusi femeile exceleaz n mai multe manifestri dect
brbatii.
Exist probabilitatea ca drept cauz a agresivittii feminine s fie predominarea tot mai mare
a masculinittii la femei. n urma studiului am constat de asemenea c subiectii de gen masculin
sunt predispusi mai putin inhibitiei dect subiectii de gen feminin.
Summary
The theoretical experimental study presented in this article offers solution to two
psychological problems of maximum significance and actuality consisting in the existence of a
stereotype that men are more aggressive than women. This stereotype dominates most human
conduct, behavior and imposes certain forms of inappropriate behavior and bad attitudes. What
are the specific gender differences in aggressiveness. These differences between genders should
not be understood in terms of deficit or superiority of a gender versus another. Differences
represent different skills and behavioral types that are social constructed. In our case is the
stereotype as a social construction. The purpose of research consists in defining the overall
picture of male and female aggression and dismantling existing stereotype.
Methodological bases of the research are Kons, Eaglys, Stepanencos and Ashmores theories.
As a result of psychological experiment accomplished on two samples of subject of adult age
(200 persons) there were revealed the specific manifestation of male, female aggression. Female
and male aggression differs through content, form and intensity. Female aggression takes
dormant form, hidden or other than direct aggression that is shown by men and has other
content.
The results of the present research can be applied in the education like a support for promotion of
gender equality. It may serve as a basis for changing the existing stereotypes.
Key words: female aggression, male aggression, gender, social stereotype.
Bibliografie
Ashmore 1990: Ashmore R. D. Sex Gender and the Individual. In: Handbook of Personality
Theory and Research (1990).
Bem 1983: Bem S. Gender Schema Theory and Its Implications for Child Development In:
Journal of Women in Culture and Society v. 8 nr. 4 (1983) 598-615.
Basov S. Gender Stereotypes and Roles. Cole Publ. Company (Brooks 1992).
106
Buss. A., (1961), The psychology of aggresion, N.Y.
Bercowitz. I., (1974), Some determinants of impulsive aggresion, N.Y.
Brown J. (2000) Gender and policing. Great Britain. Ed. By Macmillan LTD
Robinson V. (1993-1997). Women's studies. Second edition. Ed Palgrave
Halperin, D., F., (1992) Sex Differences in Cognitive Abilities, Lawrence Erlbaum
Associates, Publisher.
Bodrug V. (2001). Gender si educatie. Chisinu. Editura stiintific si didactic.
Bourhis Richard J. (1997). Stereotipuri, discriminare si relatii intergrupuri. Iasi. Polirom
Mitrofan Iolanda (1997). Psihologia relatiilor dintre sexe. Bucuresti. Editura Alternative
Laurentiu Soitu, Cornel Hovrneanu., (2001) Agresivitatea n scoal Iasi. monografie
Eibl Eibesfeldt., (1995), Agresivitatea uman. Studiu etologic, Bucuresti
Bercowitz. I., (1974), Some determinants of impulsive aggresion, N.Y
F+pon, (1996), Arpeccnx, Canxr Herepypr
Primit 25.11.2008
Comparison: med students vs. nursing students vs. first aid students the processes of
making decisions in handling a medical emergency
By: Tarabeih Mahdi, Victoria Gona, Carolina Perjan
This study focuses on the differences between first aid students and nursing students and
between med students regarding the process of solving problems while facing emergency
situations (1,2).
For the purpose of these studies experts and beginners differ from one another by the number
of years of experience they have accumulated in one field of expertise. In our case we wish to
compare between students of the same field but from different trainings while being required to
solve an identical medical problem. The three groups differ in the way they have received their
training with which they are familiar when approaching the solution of a problem rather than the
number years of experience they have accumulated. In both fields of training the learners are
intended to treat patients and save lives. While doctors are supposed to face a wide variety of
medical problems and treat them, first aid students and nurses are trained to stabilize the condition
of patients, or injured in the field, and transfer them as quickly as possible to a hospital for a
continuation of treatment. In the course of studies they learn and develop themselves the ability to
107
make decisions and use strategies to solve problems, which enable them to implement tremendous
amounts of theoretical knowledge to the medical situations facing them ( 2,3). The thinking
process doctors are taught is cognitive reorganization or operation of knowledge, both from the
external environment and from that kept in memory (4).On the other hand, the emphasis put in the
paramedics curriculum is on training the learners and developing their skills to act quickly and
implement the proper treatment at the right time during emergency situations. The thinking
process among paramedics and nurses is organization of the studied material, creation, operation
and acquisition of symbols and ideas in the process of solving problems and making decisions,
which is more defined and target-aimed (5). In order to understand the differences between
paramedics and doctors, they could be compared to the differences between declared
knowledge (or: knowing what) and practical knowledge (or: knowing how). Declared
knowledge means knowing about a certain subject only on the declarative level, which is an
aspect of supportive knowledge. Procedural knowledge, on the other hand, means knowing how
and it relates to the ability to carry out skill activities such as riding a bike or playing a piano, or
inserting airway transfusion, intraosseous transfusion, etc (2, 3, 4, 5).
The foundation of all professions is based on declarative knowledge and procedural knowledge,
but we understand that different professions differ in the amount and dosage of declarative
knowledge and procedural knowledge involved in them (e.g. engineers vs. technicians). While
medical studies put a stress on acquiring declarative knowledge while memorizing a lot of
theoretical material of health-related subjects, the paramedical profession emphasizes learning
procedures and training the required skills which will enable implementation of the procedures
(6,7).
For the purpose of this research we have defined the doctors curriculum as having a declarative
emphasis and the curriculum of paramedics and nurses as having a procedural emphasis.
Procedural knowledge is especially effective when dealing with well-defined situations. In such
situations the problem solver can identify a clear target, is capable of understanding the primary
conditions and the constraints and knows exactly what to use in order to solve the problem.
Handling emergency situations requires the skill of rational clinical judgment regarding the
severity of the problem and the quick implementation by a qualified and skilled team. Fortunately,
emergency situations such as an attack of acute asthma or myocardial infraction are considered
well-defined problems. In other words, a person qualified to provide treatment can immediately
identify the medical problem, know what treatment is required and what is not, and quickly
implement the correct procedure in order to save a life. This demonstrates the importance of
procedural knowledge and acquiring the required skills in order to operate effectively in
108
emergency situations. We believe that both doctors and paramedics and nurses should be trained
how to effectively handle emergency situations (7,8,9,10).
In the current research we compare and examine the performances of doctors who have completed
training with an emphasis on declarative knowledge vs. the performances of paramedics and
nurses who have completed a training program with an emphasis on procedural knowledge
regarding an intervention in a well defined medical situation of an acute asthma attack in a child.
In order to examine this target we will observe the following things: (a) are there differences
between doctors, nurses and paramedics in identifying the severity of the problem presented to
them? (b) Are there differences between the medical interventions applied by the three groups?
(c) Are there differences in the students knowledge regarding the constraints of interventions
they decide to implement, and which actions are redundant or should be avoided? (d) Are there
differences among the three groups in the order of procedures?
The research approach is qualitative and has been chosen in order to enable the participants to
exhibit their skills and in order to make use of the actions of the participants as data.
Participants: the participants in this research were:
(a) 50 graduate students who completed their sixth final year at the med school prior to going into
internship. In the course of their studies the students have gained experience in working with real
patients. During the fifth and sixth years the students work in rotations at the hospitals different
wards. In addition, during the sixth year they gain experience at the emergency medicine wards.
(b) 25 students who are graduates of the second and last year of the paramedic course. The studies
include a 15-week rotation at different hospital wards as well as 80 eight-hour units in an
ambulance.
(c) 30 student nurses, graduates of the fourth year, with 4-month intensive care training.
Procedure:
The participants were presented with a case of a 6-year old boy who suffers from an acute asthma
attack and does not respond to an initial bronchidultors treatment at home, and were given a 15-
minute time limit to treat the case. The location of the event included the following things: (1)
prior to entering the emergency room the students received an initial written description which
included a short background review of the patient, the location (the hospitals emergency room)
and the medical problem. (2) A boy with an arrhythmia simulator was put in an emergency room
bed. (3) Vital emergency equipment including oxygen, monitor, suction, medicines and life
support equipment. (4) Only at the doctors station a nurse was present in order to supply
medicines and equipment at the students request. The purpose here was to imitate a real situation
109
where the doctor is assisted by an additional team, compared to paramedics who function by
themselves. (5) A doctor was present on the spot to provide additional medical information at the
students request, to operate the simulator and to respond to the therapeutic means taken by the
student. Every case developed according to the steps taken by the participant: if the correct
treatment was given at a reasonable time frame and according to the required order of steps, the
childs condition improved. If incorrect measures were taken and vital steps were left out, the
childs condition deteriorated to hypoxemia, respiratory failure and finally apnea and CPR. (6) An
observation of every student and the steps he took was carried out by a registered nurse who
specializes in intensive care, who kept record of all the actions whether relevant or not on a
suitable form according to the sequence of events.
The events were documented word for word and an analysis of inductions was carried out where
behavior modes, motives and actions were taken from the records. The analysis process was based
on:
1. All texts were read and reread individually in order to create some sort of understanding
and make meaningful claims about the students and their knowledge regarding the actions taken
by them.
2. On additional readings an attempt was made to find confirmation or negation to the
temporary claims we reached.
3. After reading the texts individually and making temporary claims, the first author and the
third author read the texts as a group for the purpose of making a contextual analysis. The reading
was interrupted every time one of the authors thought that a meaningful event had taken place and
then all the texts were checked again, when necessary, so that every claim would be examined
thoroughly by the researchers. In the course of this process of constant comparison as part of the
confirmation method the initial claims raised were corrected.
4. When temporary claims were raised, the texts were examined in order to find additional
operators which support or negate these claims and that led to corrected claims.
Results:
a. Interventions which were used:
1) All paramedics and nurses implemented most of the necessary procedures whereas
only 53% of the doctors did so.
2) All paramedics and nurses gave oxygen as required whereas one third of the
doctors did not. In addition, the paramedics and nurses knew the proper dosages/oxygen flow they
should give whereas 40% of the doctors giving oxygen did not know.
110
3) All the paramedics and nurses, except one, measured oxygen stortions in order to
evaluate the childs condition and match the treatment whereas only 60% of the doctors did so.
4) 100% of the paramedics and nurses gave inhalations compared to 80% of the doctors.
5) 76% of the paramedics and nurses gave hypodermic adrenaline after oxygen and
inhalations. On the other hand 53% of the doctors gave IM and 47% hypodermic. Moreover,
whereas all the paramedics except one gave adrenaline as required due to acute asthma attack,
47% of the doctors did it incorrectly. They chose intravenous injection instead of hypodermic.
They also gave the medicine incorrectly, as it should be given intravenously.
6) 48% of the doctors decided to intubate the child almost immediately. This step was
completely unjustified according to the initial clinical symptoms, and they should have used it
later on as a last resort. Unlike the doctors, the paramedics and nurses did not consider
intubating the child.
b. Proceedings in emergency situations:
1) Whereas the paramedics and nurses started immediately with giving oxygen and
inhalations, many doctors started the intervention by asking diagnostic and family history
questions.
2) The paramedics and nurses reacted quicker than the doctors. While the average
response time among the doctors was 19.3 minutes, the average time among the paramedics stood
at 7.1 minutes, and among nurses 7.6 minutes.
3) The number and scope of questions: the paramedics tended to ask fewer questions
the average number of their questions stood at 5.56, compared to 18.9 by doctors and 5.61 by
nurses. The number of questions asked by paramedics ranged between 0-13, compared to 0-36 by
doctors and 0-12 by nurses. Doctors tended to be more diagnostic in nature (e.g. does anyone
else at home suffer from asthma? Is he sensitive to any chemical substance, medicine, food,
dust?), compared to the paramedics whose queries were aimed at clarifying the physical state of
the child (e.g. has the condition of the child improved after giving inhalation? How does the child
seem to you now has his condition become worse, the same or better?).
4) The paramedics function was identical whereas that of the doctors differed from
one another. The following table demonstrates an example of the observation on three students.
Observation A shows a typical paramedic. Observation B1 and B2 demonstrates an example of
two doctors and observation C demonstrates a nurse. It demonstrates how the student was asking
consecutive questions prior to performing any medical action. An observation on student A1
shows the medical functioning of another student. It can be seen that the students questions and
the actions taken by him were carried out one after the other both medical actions, diagnostic
111
questions, actions again and diagnostic questions again. Student B2 starts with asking diagnostic
questions, giving treatment and back to asking questions for the purpose of receiving anamnesis.
Here it can be seen that regarding the two students, B1 and B2 there is no order in treating the
emergency situation and no reference according to ABC. This example demonstrates the different
approach of the two groups of students. The two students in the examples tended to ask thorough
questions, compared to the paramedic and the nurse who took action. The only question the latter
asked was meant to clarify the condition of the boy after the intervention.
Table 1
Med student B2 Med student B1 Paramedic A
1. Did he receive
inhalations with Bricalin
at home?
2. Giving oxygen,
stortion check,
examining vital signs.
3. Stortion 93%.
4. Pulse 120 per minute.
5. Number of breathings
46 per minute.
6. Listens to the lungs.
7. Blown breathing
sounds.
8. Installs inhalation
with Ventolin.
9. How many attacks a
year does he have?
10. How many?
11. Does he take
steroids at home? No.
12. Does he have attacks
at night?
13. Not lately.
14. When did he arrive
at the emergency room?
1. Does he breath: yes.
2. Did he receive
medicines at home?
3. Yes. Inhalations.
4. Did he receive steroids?
5. Yes, Budicort.
6. Did you try to give him
something at home?
7. Yes, none helped.
8. Has he made any
physical effort lately: No.
9. Is there anyone else at
home who is sick?
10. Did he have an attack
in the past?
11. Yes, he was
hospitalized twice.
12. Has he had an attack
recently?
13. This is the first attack
in the recent period.
14. Did he receive
medication through the
infusion? No.
15. Has he been ventilated
1. Giving 5lit oxygen.
2. Checking vital
signs.
3. Preparing infusion.
4. Listens to chest
lungs, listens to back
lungs.
5. Giving inhalation
with 0.5cc adrenaline.
6. Solumedrol
infusion, giving
steroids intravenously.
7. What is the
condition of the boy?
8. Considers giving
adrenaline.
9. Stortion falls below
80%.
10. The boy develops
bradicardia.
11. The paramedic
ventilates him with
mask and ambo.
12. Examines the
boys condition.
112
We have just arrived.
Listens to the lungs
again.
15. Prepares infusion.
16. Gives steroids in
infusion.
17. Gives adrenaline.
18. What is his
condition?
19. Does he suffer from
allergy? Unknown.
20. Does he suffer from
allergy-causing
medicines? Unknown.
21. Pulse 49.
22. Breathing difficulty.
23. Considers
intubation.
24. Asks for help when
required.
25. The condition is
stabilized.
26. Since when has the
boy been suffering from
asthma?
27. Does anyone at
home have asthma
except mother?
28. Has he made any
strenuous physical effort
lately?
29. Has the boy
swallowed something?
30. What medicines is
in the past? No.
16. Is he allergic to
medicines? No.
17. Is he allergic to
chemical substances,
flowers? No.
18. How long has he been
suffering? Since the age of
2.
19. Does anyone else have
asthma in the family? Yes,
my wife.
20. Are there other
illnesses?
21. Does he have
difficulty breathing?
22. Oxygen tube is given
near the boys mouth of a
quantity of 1lit.
23. Adds inhalations with
Bricalin.
24. Examines breathing
52 per minute.
25. Examines pulse 127
per minute.
26. Examines blood
pressure 135/78.
27. Listens to the lungs
weak sounds, wheezes
during expiration.
28. Prepares infusion.
29. Gives adrenaline
through the muscle.
30. Gives steroids.
13. The boy is getting
better.
14. The paramedic
puts back the 5lit mask
for one minute.
15. The student has
completed the task.
Nurse C
------------
1. Is he conscious?
Yes.
2. How long has he
been suffering from
asthma? For a year.
3. When did he last
receive inhalation? 5
hours ago.
4. What does he
usually receive?
Ventolin inhalation.
5. The nurse gives 3lit
oxygen with a mask in
the mothers arms.
6. Listens to back and
chest lungs in the
mothers arms.
Wheezing and lengthy
expiration.
7. Will receive
Ventolin inhalation
every half hour.
8. Giving
Ethylchloride at the
113
he given at home?
31. The boy is instable,
reduced pulse, lips
turned blue, difficulty
breathing.
32. Giving 2lit oxygen
with a mask.
33. Giving Bricalin
inhalation.
34. Cardiopulmonary
arrest.
35. Ventilation with
ambo and mask.
31. Measures respiratory
rate.
32. The condition does not
improve but deteriorates.
33. Gets ready for
intubation.
34. Bradicardia (60),
shallow breathing.
35. Ventilation with ambo
and mask.
infusion insertion area
and opening peripheral
infusion (for pain
killing).
9. Giving Budicart
inhalation.
10. Giving Dexacorit
with the infusion.
11. Listening to the
lungs less and less
wheezing.
12. Measuring vital
signs: pulse (103), sat
(99%), blood pressure
(99/53).
The boy is panting
less, feels well.
The nurse has
completed the task.
Teaching during the clinical year and the fifth and sixth study years is based on
demonstrations and personal experience under supervision. It focuses on identifying the clinical
problems, their analysis and the construction of a clarification and treatment program. The student
is expected to be able to absorb anamnesis and examine a patient within a limited time frame, to
carry out special diagnostic operations (punctures and treatment of samples received as coloring
as well as microscopic examination) and treatment operations (stitching cuts, casting and draining
abscesses). In addition, he should be capable of starting advance life support and provide first aid
at a combat medical aidman level. The use of simulation methods and diagnostic means is
demonstrated such as x-ray, CT, echocardiograph, determining lung functioning, ultrasound
examination while comparing the findings to those of a physical examination. The student
exercises access to the common clinical emergency room situations such as fractures and bruises,
complex injuries, myocardial infraction, pulmonary edema, diarrhea, bronchial asthma and
intoxications.
For that purpose the students stay at the emergency room in groups of 1-2 students for one week
out of the 6-week internal medicine ward round during the sixth study year, or for a period of
114
voluntary 1-3 weeks out of the voluntary period. They are required to accept patients, collect
anamnesis, identify physical findings and problems, offer clarification and treatment methods.
The student is required to summarize the anamnesis data and the physical findings, to formulate
the patients list of problems and to briefly answer the questions: What have you found? What
in your opinion does the patient suffer from? and What do you suggest to do?
According to the workload at the emergency room a discussion is held about the differential
diagnosis, the means for clarification and initial treatment, as well as definition of the urgency of
clarification and treatment and the framework in which they were carried out. The student is
encouraged to do some reading and, when needed, literary references are presented. He
experiences, as much as possible, various activities and the use of medical instruments at the
emergency room, under control. The round of students from the internal medicine ward both
during the fourth and the fifth years enables to follow up, in the course of hospitalization, the
acute problem discovered at the emergency room. Throughout the period of staying at the
emergency room the student continues to participate in the teaching activity of the internal
medicine ward. Chosen chapters in the field of internal and urgent medicine are transferred with
the various diagnostic and treatment activities (diagnostic punctures, life support, treating a
simple injury) and students acquire the ability to work under time limitations and workload
conditions. Emphasis is put on individual thinking, clinical judgment and the development of
skills in building relationships with the patient and his family members. The interns stay at the
emergency room for about a month. The teaching pattern is similar to that given to sixth-year
students while permitting greater autonomy in the initial clarification of the patients situation
until he is presented to the doctor. The need to closely supervise the interns activities, and verify
his findings and training limits the number of interns trained at the emergency room to one per
each doctor.
References
1. Lakoff, G., & Turner, M. (1989). More than cool reason: the power of poetic metaphor.
Chicago: University of Chicago Press.
2. Newell, A., & Simon, H.A. (1972). Human problem solving. Englewood Cliffs, NJ:
Prentice-Hall.
3. Voss, J.F., & Post, T.A. (1988). On the solving of ill-structured problems. In M.T.H. Chi,
R. Glaser, & M.J. Farr (Eds.), The nature of expertise. Hillsdale, NJ: Lawrence Erlbaum
Associates.
4. Barrows, H.S., & Feltovich, P.J. (1987). The clinical reasoning process. Medical
Education, 21, 86-91.
115
5. Wass, V., Van der, Vleuten, C., Shatzer, J., & Jones, R. Assessment of clinical
competence. (2001). The Lancet. 357: 945-949.
6. Miller, G.E. The assessment of clinical skills, competence performance. (1990). Acad
Med. 65: S63-S67.
7. Arocha, J.F., Patel , V.L., & Patel, Y.C. (1993). Hypothesis generation and coordination of
theory and evidence in novice diagnostic reasoning. Medical Decision Making, 13, 198-211.
8. Barrows, H.S., & Feltovich, P.J. (1987). The clinical reasoning process. Medical
Education, 21, 86-91.
9. Bowen, G.M., Roth, W.M., & McGinn, M. K. (1999). Interpretation of graphs by
university biology students and practicing scientists: toward a social practice view of scientific
representation practices. Journal of Research in Science Teaching 36: 1020-1043.
10. Elstein, A.S., Shulman, L.S., & Sprafka, S.S. (1978). Medical Problem Solving: An
Analysis of Clinical Reasoning. Harvard University Press, Cambridge, MA.
Primit 25.11.2008
S-ar putea să vă placă și
- Asistenţa Socială A Copilului Abandonat 2Document41 paginiAsistenţa Socială A Copilului Abandonat 2cristins93% (27)
- Calitatea Vietii Copiilor Institutionalizati - DASCALEANUDocument30 paginiCalitatea Vietii Copiilor Institutionalizati - DASCALEANURoxana DascaleanuÎncă nu există evaluări
- Asistenta Sociala - Studiu de Caz (PDF)Document27 paginiAsistenta Sociala - Studiu de Caz (PDF)fliciu100% (7)
- Abandonul CopiluluiDocument13 paginiAbandonul CopiluluiAlex George100% (1)
- Studiu Privind Situatia Tinerilor Care Parasesc Sistemul de Protectie A Copilului (MMSSF) PDFDocument190 paginiStudiu Privind Situatia Tinerilor Care Parasesc Sistemul de Protectie A Copilului (MMSSF) PDFMagda V.100% (1)
- Integrarea Copiilor InstitutionalizatiDocument6 paginiIntegrarea Copiilor InstitutionalizatiBianca Mihaela Lupan100% (1)
- Grile Drept Penal - Partea GeneralaDocument91 paginiGrile Drept Penal - Partea GeneralakaseaÎncă nu există evaluări
- Ghidul Asistentului Social ComunitarDocument94 paginiGhidul Asistentului Social ComunitarDima BeznosÎncă nu există evaluări
- Asistenţa Socială A Copilului Abandonat 7Document11 paginiAsistenţa Socială A Copilului Abandonat 7cristins100% (3)
- Centrul MaternalDocument5 paginiCentrul MaternalIulia ChirilăÎncă nu există evaluări
- PlasamentulDocument7 paginiPlasamentulazareus123Încă nu există evaluări
- Asistenţa Maternală În RomâniaDocument48 paginiAsistenţa Maternală În RomâniaOana Duță100% (1)
- Statutul Copilului Aflat În DificultateDocument9 paginiStatutul Copilului Aflat În DificultateHoropan MarinelÎncă nu există evaluări
- Asistenta Sociala A Copilului in RomaniaDocument28 paginiAsistenta Sociala A Copilului in Romaniamiki1222Încă nu există evaluări
- Copiii Institutionalizati 1Document5 paginiCopiii Institutionalizati 1Adelina Eliza GrigoreÎncă nu există evaluări
- FENOMENUL ABUZULUI ŞI NEGLIJAREA COPIILOR - Studii de Caz: Copiii Cu Nevoi SpecialeDocument18 paginiFENOMENUL ABUZULUI ŞI NEGLIJAREA COPIILOR - Studii de Caz: Copiii Cu Nevoi SpecialeRuxiFuxiÎncă nu există evaluări
- Educatia in Casele de Copii Din RomaniaDocument9 paginiEducatia in Casele de Copii Din RomaniaDorina Nail SuceavaÎncă nu există evaluări
- Asistență Socială - Resocializarea Copiilor InstituționalizațiDocument6 paginiAsistență Socială - Resocializarea Copiilor InstituționalizațiZauner Ionela CameliaÎncă nu există evaluări
- Institutionalizarea Copiilor o Solutie A Unei Probleme SocialeDocument13 paginiInstitutionalizarea Copiilor o Solutie A Unei Probleme SocialeAdina Ingrid50% (4)
- Asistenta Sociala A Copilului Si FamilieiDocument111 paginiAsistenta Sociala A Copilului Si FamilieiCatalina BerescuÎncă nu există evaluări
- InstitutionalizareaDocument11 paginiInstitutionalizareaMoșneagu Beatrice100% (1)
- Asistenta Familiei Si CopiluluiDocument61 paginiAsistenta Familiei Si CopiluluiAndreea BugeacÎncă nu există evaluări
- Studii de CazDocument6 paginiStudii de CazadadianitaÎncă nu există evaluări
- Problematica Copiilor Din PlasamentDocument4 paginiProblematica Copiilor Din PlasamentFlorin GrasuÎncă nu există evaluări
- Copilul Instituționalizat Și Intervenția Asistenței Sociale În Modificare PersoanlitățiiDocument11 paginiCopilul Instituționalizat Și Intervenția Asistenței Sociale În Modificare PersoanlitățiiM. RomanÎncă nu există evaluări
- Tehnici in Asistenta Sociala. Studiu de Caz Individual - Persoana Dependenta de AlcoolDocument10 paginiTehnici in Asistenta Sociala. Studiu de Caz Individual - Persoana Dependenta de AlcoolMadalina FrunzaÎncă nu există evaluări
- Evaluarea Programelor de Asistenta Sociala PDFDocument2 paginiEvaluarea Programelor de Asistenta Sociala PDFNancy33% (3)
- Referat EvaluareDocument5 paginiReferat EvaluareSabina GurguÎncă nu există evaluări
- Copilul InstitutionalizatDocument9 paginiCopilul InstitutionalizatGabor Eusebiu100% (2)
- Forme de Ocrotire A Copilului Aflat in Dificultate 390Document9 paginiForme de Ocrotire A Copilului Aflat in Dificultate 390Nastasiuc AdrianÎncă nu există evaluări
- Integrarea Socio Profesionala A Tinerilor Ce Parasesc Centrele de PlasamentDocument106 paginiIntegrarea Socio Profesionala A Tinerilor Ce Parasesc Centrele de PlasamentbogdanplotterÎncă nu există evaluări
- Tineri Care Parasesc Sistemul de Protectie StudiuDocument190 paginiTineri Care Parasesc Sistemul de Protectie StudiuServiciul Strategii Programe ProiecteÎncă nu există evaluări
- Abandonul MinorilorDocument41 paginiAbandonul MinorilorAndrei Iancu100% (1)
- Asistenta Sociala in Caz de Adoptie Si PlasamentDocument5 paginiAsistenta Sociala in Caz de Adoptie Si PlasamentTanase Patricia100% (2)
- Asistenţa Socială A Copilului Abandonat 5Document7 paginiAsistenţa Socială A Copilului Abandonat 5cristinsÎncă nu există evaluări
- Abandonul FamilialDocument7 paginiAbandonul Familialcami_1012Încă nu există evaluări
- Copiii Din Sistemul de Protectie A Copilului PDFDocument573 paginiCopiii Din Sistemul de Protectie A Copilului PDFFlavi Sfabu100% (1)
- AS Soc A Familiei - Curs ID - 2018-2019Document53 paginiAS Soc A Familiei - Curs ID - 2018-2019IuliaÎncă nu există evaluări
- Bibliografie LicentaDocument4 paginiBibliografie LicentaRadu DanielaÎncă nu există evaluări
- Consilierea Copiilor Cu Părinții Plecați LaDocument59 paginiConsilierea Copiilor Cu Părinții Plecați LaAde AdriiÎncă nu există evaluări
- Managementul Integrarearii Socioprofesionle A Tinerilor-PostinstitutionalizatiDocument101 paginiManagementul Integrarearii Socioprofesionle A Tinerilor-PostinstitutionalizatiElena Oprea100% (1)
- Institutionalizarea Copiilor o Solutie A Unei Probleme SocialeDocument13 paginiInstitutionalizarea Copiilor o Solutie A Unei Probleme SocialeVictorita - Maria RaducanÎncă nu există evaluări
- Lucrare de Licenta Despre Abandonul Copiilor in MaternitateDocument2 paginiLucrare de Licenta Despre Abandonul Copiilor in MaternitateIuliana Berianu0% (2)
- Copil InstituționalizatDocument3 paginiCopil InstituționalizatBadareu Gheorghe AlaÎncă nu există evaluări
- Abuzul Si Malt Rat Area CopiluluiDocument11 paginiAbuzul Si Malt Rat Area CopiluluiGygy GykanuÎncă nu există evaluări
- Burcă Maria Magdalena Aplicația 1Document8 paginiBurcă Maria Magdalena Aplicația 1Maya Mayutza100% (1)
- Efecte Ale InstitutionalizariiDocument8 paginiEfecte Ale InstitutionalizariitibvalÎncă nu există evaluări
- Protectia Sociala A Copilului Aflat in DificultateDocument8 paginiProtectia Sociala A Copilului Aflat in DificultateGabor EusebiuÎncă nu există evaluări
- Institutionalizarea Copiilor Si EfecteleDocument46 paginiInstitutionalizarea Copiilor Si EfecteleViorel Iorda0% (1)
- Cap IIDocument9 paginiCap IIRoxana Andreea CiupercaÎncă nu există evaluări
- Institutionalizare EfecteDocument8 paginiInstitutionalizare EfecteBarbieru Marina-andreeaÎncă nu există evaluări
- Separarea Copilului de Fam BiologicaDocument8 paginiSepararea Copilului de Fam BiologicaSorina LaviniaÎncă nu există evaluări
- Proiect Management de CazDocument7 paginiProiect Management de CazCarmen IoanaÎncă nu există evaluări
- Fisa Initiala A CazuluiDocument2 paginiFisa Initiala A CazuluiSilvestra DenaÎncă nu există evaluări
- ECOMAPADocument149 paginiECOMAPAtulbyÎncă nu există evaluări
- UNIVERSITATEADocument6 paginiUNIVERSITATEAemanuelneagu70Încă nu există evaluări
- Sistemul de Protecție Socială A Copilului În RomâniaDocument10 paginiSistemul de Protecție Socială A Copilului În RomâniaDelia DimaÎncă nu există evaluări
- Proiect La Dezvoltare ComunitarăDocument7 paginiProiect La Dezvoltare ComunitarăNechita AdrianÎncă nu există evaluări
- Institutiile Rezidentiale Pentru Ocrotirea CopiluluiDocument2 paginiInstitutiile Rezidentiale Pentru Ocrotirea CopiluluiAlex IonescuÎncă nu există evaluări
- Consecințe Şi Dificultăți Întâmpinate de Tinerii Instituționalizați, Din Iaşi, În Integrarea Lor În Societate Şi În Sfera EducaţionalăDocument4 paginiConsecințe Şi Dificultăți Întâmpinate de Tinerii Instituționalizați, Din Iaşi, În Integrarea Lor În Societate Şi În Sfera EducaţionalăMaria Magdalena DoltuÎncă nu există evaluări
- Decizie 1600 - 2016 Ghid POGDocument15 paginiDecizie 1600 - 2016 Ghid POGkaseaÎncă nu există evaluări
- Comisionariat Vamal InfoDocument8 paginiComisionariat Vamal InfokaseaÎncă nu există evaluări
- Jeleu de Limeta Cu MentaDocument1 paginăJeleu de Limeta Cu MentakaseaÎncă nu există evaluări
- Ordonanta de Urgenta NR .97 /2005Document16 paginiOrdonanta de Urgenta NR .97 /2005kaseaÎncă nu există evaluări
- Mazare Cu Menta Sott'OlioDocument2 paginiMazare Cu Menta Sott'OliokaseaÎncă nu există evaluări
- Materiale Limba EnglezaDocument26 paginiMateriale Limba EnglezakaseaÎncă nu există evaluări
- Manualul Copii Istoria Ucrainei Clasa VDocument252 paginiManualul Copii Istoria Ucrainei Clasa Vriana 77Încă nu există evaluări